Zaltrap
f6725df6-50ee-4b0a-b900-d02ba634395d
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
ZALTRAP, in combination with fluorouracil, leucovorin, irinotecan-(FOLFIRI), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen.
Dosage and Administration
4 mg per kg as an intravenous infusion over 1 hour every 2 weeks. ( 2.1 , 2.3 ) Do not administer as an intravenous push or bolus. ( 2.3 )
Contraindications
None.
Warnings and Precautions
Hemorrhage : Severe and sometimes fatal hemorrhage, including gastrointestinal (GI) hemorrhage, has been reported in patients who have received ZALTRAP. Do not administer ZALTRAP to patients with severe hemorrhage. ( 5.1 ) Gastrointestinal Perforation : Discontinue ZALTRAP therapy in patients who experience GI perforation. ( 5.2 ) Impaired Wound Healing : Withhold ZALTRAP for at least 4 weeks prior to elective surgery. Do not administer for at least 4 weeks following major surgery and until wounds have adequately healed. Discontinue ZALTRAP in patients with impaired wound healing. The safety of resumption of ZALTRAP after resolution of wound healing complications has not been established. ( 5.3 ) Fistula Formation : Discontinue ZALTRAP if fistula occurs. ( 2.2 , 5.4 ) Hypertension : Monitor blood pressure and treat hypertension. Temporarily suspend ZALTRAP if hypertension is not controlled. Discontinue ZALTRAP if hypertensive crisis develops. ( 2.2 , 5.5 ) Arterial Thromboembolic Events (ATE) : Discontinue ZALTRAP if ATE develops. ( 5.6 ) Proteinuria : Monitor urine protein. Suspend ZALTRAP for proteinuria of 2 grams per 24 hours or more. Discontinue ZALTRAP if nephrotic syndrome or thrombotic microangiopathy (TMA) develops. ( 2.2 , 5.7 ) Neutropenia and Neutropenic Complications : Delay administration of ZALTRAP/FOLFIRI until neutrophil count is 1.5 × 10 9 /L or higher. ( 5.8 ) Diarrhea and Dehydration : Incidence of severe diarrhea and dehydration is increased. Monitor elderly patients more closely. ( 5.9 , 8.5 ) Reversible Posterior Leukoencephalopathy Syndrome : Discontinue ZALTRAP. ( 5.10 ) Embryo-Fetal Toxicity : Can cause fetal harm. Advise females of potential risk to fetus and need for use of effective contraception. ( 5.11 , 8.1 , 8.3 )
Adverse Reactions
Discontinue ZALTRAP for: Severe hemorrhage [see Warnings and Precautions (5.1) ] Gastrointestinal perforation [see Warnings and Precautions (5.2) ] Impaired wound healing [see Warnings and Precautions (5.3) ] Fistula formation [see Warnings and Precautions (5.4) ] Hypertensive crisis or hypertensive encephalopathy [see Warnings and Precautions (5.5) ] Arterial thromboembolic events (ATE) [see Warnings and Precautions (5.6) ] Nephrotic syndrome or thrombotic microangiopathy (TMA) [see Warnings and Precautions (5.7) ] Reversible posterior leukoencephalopathy syndrome (RPLS) [see Warnings and Precautions (5.10) ] Temporarily suspend ZALTRAP: At least 4 weeks prior to elective surgery [see Warnings and Precautions (5.3) ]. For uncontrolled hypertension until controlled. Upon resumption, permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.5) ] . For proteinuria of 2 grams per 24 hours or more. Resume when proteinuria is less than 2 grams per 24 hours. For recurrent proteinuria, suspend ZALTRAP until proteinuria is less than 2 grams per 24 hours and then permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.7) ] .
Drug Interactions
No dedicated drug-drug interaction studies have been conducted for ZALTRAP. No clinically important pharmacokinetic interactions were found between ziv-aflibercept and irinotecan/SN-38 or fluorouracil [see Clinical Pharmacology (12.3) ] .
How Supplied
ZALTRAP (ziv-aflibercept) injection is a clear, colorless to pale-yellow solution supplied in single-dose vials with a concentration of 25 mg/mL. NDC 0024-5840-01: carton containing one single-dose vial of 100 mg/4 mL (25 mg/mL) NDC 0024-5841-01: carton containing one single-dose vial of 200 mg/8 mL (25 mg/mL)
Storage and Handling
ZALTRAP (ziv-aflibercept) injection is a clear, colorless to pale-yellow solution supplied in single-dose vials with a concentration of 25 mg/mL. NDC 0024-5840-01: carton containing one single-dose vial of 100 mg/4 mL (25 mg/mL) NDC 0024-5841-01: carton containing one single-dose vial of 200 mg/8 mL (25 mg/mL)
Description
ZALTRAP, in combination with fluorouracil, leucovorin, irinotecan-(FOLFIRI), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen.
Medication Information
Warnings and Precautions
Hemorrhage : Severe and sometimes fatal hemorrhage, including gastrointestinal (GI) hemorrhage, has been reported in patients who have received ZALTRAP. Do not administer ZALTRAP to patients with severe hemorrhage. ( 5.1 ) Gastrointestinal Perforation : Discontinue ZALTRAP therapy in patients who experience GI perforation. ( 5.2 ) Impaired Wound Healing : Withhold ZALTRAP for at least 4 weeks prior to elective surgery. Do not administer for at least 4 weeks following major surgery and until wounds have adequately healed. Discontinue ZALTRAP in patients with impaired wound healing. The safety of resumption of ZALTRAP after resolution of wound healing complications has not been established. ( 5.3 ) Fistula Formation : Discontinue ZALTRAP if fistula occurs. ( 2.2 , 5.4 ) Hypertension : Monitor blood pressure and treat hypertension. Temporarily suspend ZALTRAP if hypertension is not controlled. Discontinue ZALTRAP if hypertensive crisis develops. ( 2.2 , 5.5 ) Arterial Thromboembolic Events (ATE) : Discontinue ZALTRAP if ATE develops. ( 5.6 ) Proteinuria : Monitor urine protein. Suspend ZALTRAP for proteinuria of 2 grams per 24 hours or more. Discontinue ZALTRAP if nephrotic syndrome or thrombotic microangiopathy (TMA) develops. ( 2.2 , 5.7 ) Neutropenia and Neutropenic Complications : Delay administration of ZALTRAP/FOLFIRI until neutrophil count is 1.5 × 10 9 /L or higher. ( 5.8 ) Diarrhea and Dehydration : Incidence of severe diarrhea and dehydration is increased. Monitor elderly patients more closely. ( 5.9 , 8.5 ) Reversible Posterior Leukoencephalopathy Syndrome : Discontinue ZALTRAP. ( 5.10 ) Embryo-Fetal Toxicity : Can cause fetal harm. Advise females of potential risk to fetus and need for use of effective contraception. ( 5.11 , 8.1 , 8.3 )
Indications and Usage
ZALTRAP, in combination with fluorouracil, leucovorin, irinotecan-(FOLFIRI), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen.
Dosage and Administration
4 mg per kg as an intravenous infusion over 1 hour every 2 weeks. ( 2.1 , 2.3 ) Do not administer as an intravenous push or bolus. ( 2.3 )
Contraindications
None.
Adverse Reactions
Discontinue ZALTRAP for: Severe hemorrhage [see Warnings and Precautions (5.1) ] Gastrointestinal perforation [see Warnings and Precautions (5.2) ] Impaired wound healing [see Warnings and Precautions (5.3) ] Fistula formation [see Warnings and Precautions (5.4) ] Hypertensive crisis or hypertensive encephalopathy [see Warnings and Precautions (5.5) ] Arterial thromboembolic events (ATE) [see Warnings and Precautions (5.6) ] Nephrotic syndrome or thrombotic microangiopathy (TMA) [see Warnings and Precautions (5.7) ] Reversible posterior leukoencephalopathy syndrome (RPLS) [see Warnings and Precautions (5.10) ] Temporarily suspend ZALTRAP: At least 4 weeks prior to elective surgery [see Warnings and Precautions (5.3) ]. For uncontrolled hypertension until controlled. Upon resumption, permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.5) ] . For proteinuria of 2 grams per 24 hours or more. Resume when proteinuria is less than 2 grams per 24 hours. For recurrent proteinuria, suspend ZALTRAP until proteinuria is less than 2 grams per 24 hours and then permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.7) ] .
Drug Interactions
No dedicated drug-drug interaction studies have been conducted for ZALTRAP. No clinically important pharmacokinetic interactions were found between ziv-aflibercept and irinotecan/SN-38 or fluorouracil [see Clinical Pharmacology (12.3) ] .
Storage and Handling
ZALTRAP (ziv-aflibercept) injection is a clear, colorless to pale-yellow solution supplied in single-dose vials with a concentration of 25 mg/mL. NDC 0024-5840-01: carton containing one single-dose vial of 100 mg/4 mL (25 mg/mL) NDC 0024-5841-01: carton containing one single-dose vial of 200 mg/8 mL (25 mg/mL)
How Supplied
ZALTRAP (ziv-aflibercept) injection is a clear, colorless to pale-yellow solution supplied in single-dose vials with a concentration of 25 mg/mL. NDC 0024-5840-01: carton containing one single-dose vial of 100 mg/4 mL (25 mg/mL) NDC 0024-5841-01: carton containing one single-dose vial of 200 mg/8 mL (25 mg/mL)
Description
ZALTRAP, in combination with fluorouracil, leucovorin, irinotecan-(FOLFIRI), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen.
Section 42229-5
Preparation
Inspect vials visually prior to use. ZALTRAP is a clear, colorless to pale yellow solution. Do not use vial if the solution is discolored or cloudy or if the solution contains particles.
Withdraw the prescribed dose of ZALTRAP and dilute in 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to achieve a final concentration of 0.6 mg/mL to 8 mg/mL.
Do not re-enter the vial after the initial puncture. Discard any unused portion left in the vial.
Use polyvinyl chloride (PVC) infusion bags containing bis (2-ethylhexyl) phthalate (DEHP) or polyolefin infusion bags.
Store diluted ZALTRAP refrigerated at 2°C to 8°C (36°F to 46°F) for up to 24 hours or at controlled room temperature of 20°C to 25°C (68°F to 77°F) for up to 8 hours. Discard any unused portion left in the infusion bag.
Section 44425-7
Store ZALTRAP vials in a refrigerator at 2°C to 8°C (36°F to 46°F). Keep the vials in the original outer carton to protect from light. Discard unused portion.
11 Description
Ziv-aflibercept is a vascular endothelial growth factor inhibitor. It is a recombinant fusion protein consisting of Vascular Endothelial Growth Factor (VEGF)-binding portions from the extracellular domains of human VEGF Receptors 1 and 2 fused to the Fc portion of the human IgG1. Ziv-aflibercept is produced by recombinant DNA technology in a Chinese hamster ovary (CHO) K-1 mammalian expression system. Ziv-aflibercept is a dimeric glycoprotein with a protein molecular weight of 97 kilodaltons (kDa) and contains glycosylation, constituting an additional 15% of the total molecular mass, resulting in a total molecular weight of 115 kDa.
ZALTRAP (ziv-aflibercept) injection is a sterile, clear, colorless to pale-yellow, non-pyrogenic, preservative-free, solution for intravenous use. ZALTRAP is supplied in single-dose vials of 100 mg/4 mL and 200 mg/8 mL formulated as 25 mg/mL ziv-aflibercept in polysorbate 20 (1 mg/mL), sodium chloride (5.84 mg/mL), sodium citrate (1.45 mg/mL), sodium phosphate (0.8 mg/mL), and sucrose (200 mg/mL), in Water for Injection, USP, at a pH of 6.2.
5.1 Hemorrhage
Patients treated with ZALTRAP have an increased risk of hemorrhage, including severe and sometimes fatal hemorrhagic events. In patients with mCRC, bleeding/hemorrhage (all grades) was reported in 38% of patients treated with ZALTRAP/FOLFIRI compared to 19% of patients treated with placebo/FOLFIRI. Grade 3–4 hemorrhagic events, including gastrointestinal hemorrhage, hematuria, and post-procedural hemorrhage, were reported in 3% of patients receiving ZALTRAP/FOLFIRI compared with 1% of patients receiving placebo/FOLFIRI. Severe intracranial hemorrhage and pulmonary hemorrhage/hemoptysis including fatal events have also occurred in patients receiving ZALTRAP.
Monitor patients for signs and symptoms of bleeding. Do not initiate ZALTRAP in patients with severe hemorrhage. Discontinue ZALTRAP in patients who develop severe hemorrhage [see Dosage and Administration (2.2)].
5.7 Proteinuria
Severe proteinuria, nephrotic syndrome, and thrombotic microangiopathy (TMA) occurred more frequently in patients treated with ZALTRAP. In patients with mCRC, proteinuria was reported in 62% patients treated with ZALTRAP/FOLFIRI compared to 41% patients treated with placebo/FOLFIRI. Grade 3–4 proteinuria occurred in 8% of patients treated with ZALTRAP/FOLFIRI compared to 1% of patients treated with placebo/FOLFIRI [see Adverse Reactions (6.1)]. Nephrotic syndrome occurred in 2 patients (0.5%) treated with ZALTRAP/FOLFIRI compared to none of the patients treated with placebo/FOLFIRI. TMA was reported in 3 of 2258 patients with cancer enrolled across completed studies.
Monitor proteinuria by urine dipstick analysis and/or urinary protein creatinine ratio (UPCR) for the development or worsening of proteinuria during ZALTRAP therapy. Patients with a dipstick of ≥2+ for protein or a UPCR greater than 1 should undergo a 24-hour urine collection.
Suspend ZALTRAP administration for proteinuria 2 grams per 24 hours or more, and resume when proteinuria is less than 2 grams per 24 hours. If recurrent, suspend until proteinuria is less than 2 grams per 24 hours and then permanently reduce the ZALTRAP dose to 2 mg per kg. Discontinue ZALTRAP in patients who develop nephrotic syndrome or TMA [see Dosage and Administration (2.2)].
5.5 Hypertension
ZALTRAP increases the risk of Grade 3–4 hypertension. There is no clinical trial experience administering ZALTRAP to patients with NYHA class III or IV heart failure. In patients with mCRC, Grade 3 hypertension (defined as requiring adjustment in existing antihypertensive therapy or treatment with more than one drug) was reported in 1.5% of patients treated with placebo/FOLFIRI and 19% of patients treated with ZALTRAP/FOLFIRI. Grade 4 hypertension (hypertensive crisis) was reported in 1 patient (0.2%) treated with ZALTRAP/FOLFIRI. Among those patients treated with ZALTRAP/FOLFIRI developing Grade 3–4 hypertension, 54% had onset during the first two cycles of treatment.
Monitor blood pressure every two weeks or more frequently as clinically indicated during treatment with ZALTRAP. Treat with appropriate antihypertensive therapy and continue monitoring blood pressure regularly. Temporarily suspend ZALTRAP in patients with uncontrolled hypertension until controlled and permanently reduce the ZALTRAP dose to 2 mg per kg for subsequent cycles. Discontinue ZALTRAP in patients with hypertensive crisis or hypertensive encephalopathy [see Dosage and Administration (2.2)].
8.4 Pediatric Use
The safety and effectiveness in pediatric patients have not been established. Safety and efficacy were assessed, but not established in a dose-escalation, safety, and tolerability study (NCT00622414) in 21 patients with solid tumors 2 to 21 years of age (median age 12.9). The mean elimination half-life of free ziv-aflibercept determined after the first dose in 8 pediatric patients aged 5 to 17 years was within the range of values previously observed in adults. The maximum tolerated dose based on body weight in these pediatric patients was lower than the dose known to be safe and effective in adults with mCRC.
8.5 Geriatric Use
Of the 611 patients with mCRC, patients treated with ZALTRAP/FOLFIRI, 205 (34%) were 65 years or older, and 33 (5%) were 75 years or older. Elderly patients (≥65 years of age) experienced higher incidences (≥5%) of diarrhea, dizziness, asthenia, weight decrease, and dehydration when compared to younger patients. Monitor elderly patients more closely for diarrhea and dehydration [see Warnings and Precautions (5.9)].
The effect of ZALTRAP on overall survival was similar in patients <65 years old and ≥65 years old who received ZALTRAP/FOLFIRI.
6.2 Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described below with the incidence of antibodies in other studies or to other products may be misleading.
In patients with various cancers across 15 studies, 1.4% (41/2862) of patients tested positive for antiproduct antibody (APA) at baseline. The incidence of APA development was 3.1% (53/1687) in patients receiving intravenous ziv-aflibercept and 1.7% (19/1134) in patients receiving placebo. Among patients who tested positive for APA and had sufficient samples for further testing, neutralizing antibodies were detected in 17 of 48 ziv-aflibercept-treated patients and in 2 of 40 patients receiving placebo.
The mean free ziv-aflibercept trough concentrations were lower in patients with positive neutralizing antibodies than in the overall population. The impact of neutralizing antibodies on efficacy and safety could not be assessed based on limited available data.
14 Clinical Studies
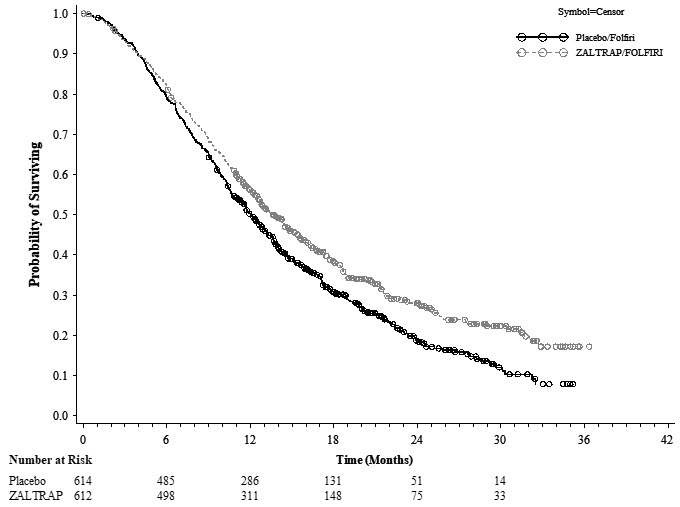
The efficacy of ZALTRAP was evaluated in VELOUR (NCT00561470), a randomized (1:1), double-blind, placebo-controlled study in patients with mCRC who are resistant to or have progressed during or within 6 months of receiving oxaliplatin-based combination chemotherapy, with or without prior bevacizumab. Patients were randomized to receive either ZALTRAP 4 mg per kg intravenously over 1 hour on day 1 or placebo in combination with FOLFIRI (irinotecan 180 mg/m2 intravenously over 90 minutes and leucovorin [dl racemic] 400 mg/m2 intravenously over 2 hours at the same time on day 1 using a Y-line, followed by fluorouracil 400 mg/m2 as an intravenous bolus and then by fluorouracil 2400 mg/m2 as a continuous intravenous infusion over 46 hours). The treatment cycles on both arms were repeated every 2 weeks. Patients were treated until disease progression or unacceptable toxicity. Randomization was stratified by the Eastern Cooperative Oncology Group performance status (PS) (0 versus 1 versus 2) and according to prior therapy with bevacizumab (yes or no). The major efficacy outcome measure was overall survival (OS). Additional efficacy outcome measures were progression-free survival (PFS) and overall response rate (ORR).
Demographics characteristics were similar between treatment arms. A total of 1226 patients were randomized, 612 to the ZALTRAP arm and 614 to the placebo arm. The median age was 61 years, 59% were men, 87% were White, 7% were Asian, 3.5% were Black, and 98% had a baseline ECOG PS of 0 or 1. Among the 1226 randomized patients, 89% and 90% of patients treated with placebo/FOLFIRI and ZALTRAP/FOLFIRI, respectively, received prior oxaliplatin-based combination chemotherapy in the metastatic/advanced setting. A total of 346 patients (28%) received bevacizumab in combination with the prior oxaliplatin-based treatment.
Efficacy results are summarized in Figure 1 and Table 2.
Figure 1: Kaplan-Meier Curves of Overall Survival for VELOUR
| ZALTRAP/FOLFIRI N=612 |
Placebo/FOLFIRI N=614 |
|
|---|---|---|
| Overall Survival | ||
| Number of deaths, n (%) | 403 (65.8%) | 460 (74.9%) |
| Median overall survival (95% CI) (months) | 13.50 (12.52, 14.95) | 12.06 (11.07, 13.08) |
| Stratified Hazard ratio (95% CI) | 0.817 (0.714, 0.935) | |
| Stratified Log-Rank test p-value | 0.0032 | |
| Progression Free Survival (PFS) | ||
| Number of events, n (%) | 393 (64.2%) | 454 (73.9%) |
| Median PFS (95% CI) (months) | 6.90 (6.51, 7.20) | 4.67 (4.21, 5.36) |
| Stratified Hazard ratio (95% CI) | 0.758 (0.661, 0.869) | |
| Stratified Log-Rank test p-value Stratified on ECOG Performance Status (0 vs 1 vs 2) and Prior Bevacizumab (yes vs no)
|
0.00007 | |
| Overall Response Rate (ORR) | ||
| ORR (CR+PR) (95% CI) Overall objective response rate by IRC
|
19.8% (16.4%, 23.2%) | 11.1% (8.5%, 13.8%) |
| Stratified Cochran-Mantel-Haenszel test p-value | 0.0001 |
Planned subgroup analyses for overall survival based on stratification factors at randomization yielded an HR of 0.86 (95% CI: 0.68, 1.1) in patients who received prior bevacizumab and an HR of 0.79 (95% CI: 0.67, 0.93) in patients without prior bevacizumab exposure.
4 Contraindications
None.
6 Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hemorrhage [see Warnings and Precautions (5.1)]
- Gastrointestinal Perforation [see Warnings and Precautions (5.2)]
- Impaired Wound Healing [see Warnings and Precautions (5.3)]
- Fistula Formation [see Warnings and Precautions (5.4)]
- Hypertension [see Warnings and Precautions (5.5)]
- Arterial Thromboembolic Events [see Warnings and Precautions (5.6)]
- Proteinuria [see Warnings and Precautions (5.7)]
- Neutropenia and Neutropenic Complications [see Warnings and Precautions (5.8)]
- Diarrhea and Dehydration [see Warnings and Precautions (5.9)]
- Reversible Posterior Leukoencephalopathy Syndrome [see Warnings and Precautions (5.10)]
7 Drug Interactions
No dedicated drug-drug interaction studies have been conducted for ZALTRAP. No clinically important pharmacokinetic interactions were found between ziv-aflibercept and irinotecan/SN-38 or fluorouracil [see Clinical Pharmacology (12.3)].
8.6 Renal Impairment
No dosage modification is recommended for patients with renal impairment [see Clinical Pharmacology (12.3)].
12.3 Pharmacokinetics
Plasma concentrations of free and VEGF-bound ziv-aflibercept were measured using specific enzyme-linked immunosorbent assays (ELISA). Free ziv-aflibercept concentrations appear to exhibit linear pharmacokinetics in the dose range of 2 mg per kg to 9 mg per kg. Steady state concentrations of free ziv-aflibercept were reached by the second dose. The accumulation ratio for free ziv-aflibercept was approximately 1.2 after administration of 4 mg per kg every two weeks.
5.4 Fistula Formation
Fistula formation involving gastrointestinal and non-gastrointestinal sites occurs at a higher incidence in patients treated with ZALTRAP. In patients with mCRC, fistulas (anal, enterovesical, enterocutaneous, colovaginal, intestinal sites) were reported in 9 of 611 patients (1.5%) treated with ZALTRAP/FOLFIRI regimen and 3 of 605 patients (0.5%) treated with placebo/FOLFIRI regimen. Grade 3 GI fistula formation occurred in 2 patients treated with ZALTRAP (0.3%) and in 1 patient treated with placebo (0.2%).
Discontinue ZALTRAP therapy in patients who develop fistula [see Dosage and Administration (2.2)].
8.7 Hepatic Impairment
No dosage modification is recommended for patients with mild (total bilirubin >1 to 1.5 times upper limit normal [ULN] and any aspartate transaminase [AST]) and moderate (total bilirubin >1.5 to 3 times ULN and any AST) hepatic impairment [see Clinical Pharmacology (12.3)]. ZALTRAP has not been studied in patients with severe hepatic impairment (total bilirubin >3 times ULN and any AST).
1 Indications and Usage
ZALTRAP, in combination with fluorouracil, leucovorin, irinotecan-(FOLFIRI), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen.
12.1 Mechanism of Action
Ziv-aflibercept acts as a soluble receptor that binds to human VEGF-A (equilibrium dissociation constant KD of 0.5 pM for VEGF-A165 and 0.36 pM for VEGF-A121), to human VEGF-B (KD of 1.92 pM), and to human PlGF (KD of 39 pM for PlGF-2). By binding to these endogenous ligands, ziv-aflibercept can inhibit the binding and activation of their cognate receptors. This inhibition can result in decreased neovascularization and decreased vascular permeability.
In animals, ziv-aflibercept was shown to inhibit the proliferation of endothelial cells, thereby inhibiting the growth of new blood vessels. Ziv-aflibercept inhibited the growth of xenotransplanted colon tumors in mice.
5 Warnings and Precautions
- Hemorrhage: Severe and sometimes fatal hemorrhage, including gastrointestinal (GI) hemorrhage, has been reported in patients who have received ZALTRAP. Do not administer ZALTRAP to patients with severe hemorrhage. (5.1)
- Gastrointestinal Perforation: Discontinue ZALTRAP therapy in patients who experience GI perforation. (5.2)
- Impaired Wound Healing: Withhold ZALTRAP for at least 4 weeks prior to elective surgery. Do not administer for at least 4 weeks following major surgery and until wounds have adequately healed. Discontinue ZALTRAP in patients with impaired wound healing. The safety of resumption of ZALTRAP after resolution of wound healing complications has not been established. (5.3)
- Fistula Formation: Discontinue ZALTRAP if fistula occurs. (2.2, 5.4)
- Hypertension: Monitor blood pressure and treat hypertension. Temporarily suspend ZALTRAP if hypertension is not controlled. Discontinue ZALTRAP if hypertensive crisis develops. (2.2, 5.5)
- Arterial Thromboembolic Events (ATE): Discontinue ZALTRAP if ATE develops. (5.6)
- Proteinuria: Monitor urine protein. Suspend ZALTRAP for proteinuria of 2 grams per 24 hours or more. Discontinue ZALTRAP if nephrotic syndrome or thrombotic microangiopathy (TMA) develops. (2.2, 5.7)
- Neutropenia and Neutropenic Complications: Delay administration of ZALTRAP/FOLFIRI until neutrophil count is 1.5 × 109/L or higher. (5.8)
- Diarrhea and Dehydration: Incidence of severe diarrhea and dehydration is increased. Monitor elderly patients more closely. (5.9, 8.5)
- Reversible Posterior Leukoencephalopathy Syndrome: Discontinue ZALTRAP. (5.10)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of potential risk to fetus and need for use of effective contraception. (5.11, 8.1, 8.3)
5.11 Embryo Fetal Toxicity
Based on findings from animal studies and its mechanism of action, ZALTRAP can cause fetal harm when administered to pregnant women. Administration of ziv-aflibercept during the period of organogenesis was embryotoxic and teratogenic in rabbits at exposure levels approximately 0.3 times the human exposure at the 4 mg per kg dose. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with ZALTRAP and for 3 months following the last dose [see Use in Specific Populations (8.1, 8.3)].
5.3 Impaired Wound Healing
Grade 3 impaired wound healing was reported in 2 patients (0.3%) treated with ZALTRAP/FOLFIRI regimen.
Withhold ZALTRAP for at least 4 weeks prior to elective surgery. Do not administer ZALTRAP for at least 4 weeks after major surgery and until wounds have adequately healed. For minor surgery such as central venous access port placement, biopsy, and tooth extraction, ZALTRAP may be initiated/resumed once the surgical wound is fully healed. Discontinue ZALTRAP in patients with impaired wound healing. The safety of resumption of ZALTRAP after resolution of wound healing complications has not been established [see Dosage and Administration (2.2)].
2 Dosage and Administration
3 Dosage Forms and Strengths
ZALTRAP is a clear, colorless to pale-yellow solution available as:
- Injection: 100 mg/4 mL (25 mg/mL) solution in a single-dose vial
- Injection: 200 mg/8 mL (25 mg/mL) solution in a single-dose vial
5.9 Diarrhea and Dehydration
The incidence of severe diarrhea is increased in patients treated with ZALTRAP/FOLFIRI. In patients with mCRC, Grade 3–4 diarrhea was reported in 19% of patients treated with ZALTRAP/FOLFIRI compared to 8% of patients treated with placebo/FOLFIRI. Grade 3–4 dehydration was reported in 4% of patients treated with ZALTRAP/FOLFIRI compared to 1% of patients treated with placebo/FOLFIRI [see Adverse Reactions (6.1)]. The incidence of diarrhea is increased in patients who are age 65 years or older as compared to patients younger than 65 years of age [see Use in Specific Populations (8.5)]. Monitor elderly patients closely for diarrhea.
6.3 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of ZALTRAP. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Musculoskeletal and connective tissue disorders: Osteonecrosis of the jaw
Cardiac disorders: Cardiac failure, ejection fraction decreased
Vascular disorders: Arterial (including aortic) aneurysms, dissections, and rupture
8 Use in Specific Populations
- Lactation: Advise not to breastfeed. (8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of ZALTRAP in combination with FOLFIRI was evaluated in VELOUR (EFC102621) [see Clinical Studies (14)]. Patients received ZALTRAP 4 mg per kg (N=611) or placebo (N=605) intravenously every two weeks (one cycle) in combination with FOLFIRI. Patients received a median of 9 cycles of ZALTRAP/FOLFIRI.
The most common Grade 3–4 adverse reactions (≥5%) in the ZALTRAP/FOLFIRI arm were neutropenia, diarrhea, hypertension, leukopenia, stomatitis, fatigue, proteinuria, and asthenia.
The most frequent adverse reactions leading to permanent discontinuation in ≥1% of patients treated with ZALTRAP/FOLFIRI regimen were asthenia/fatigue, infections, diarrhea, dehydration, hypertension, stomatitis, venous thromboembolic events, neutropenia, and proteinuria.
The ZALTRAP dose was reduced and/or omitted in 17% of patients. Cycle delays >7 days occurred in 60% of patients treated with ZALTRAP/FOLFIRI.
The most common adverse reactions (≥20%) in the ZALTRAP/FOLFIRI arm were leukopenia, diarrhea, neutropenia, proteinuria, AST increased, stomatitis, fatigue, thrombocytopenia, ALT increased, hypertension, weight decreased, decreased appetite, epistaxis, abdominal pain, dysphonia, serum creatinine increased, and headache.
Adverse reactions and laboratory abnormalities that occurred in ≥5% (all grades) of patients receiving ZALTRAP in combination with FOLFIRI and which occurred at ≥2% higher frequency in patients who received ZALTRAP/FOLFIRI compared to those who received placebo/FOLFIRI in VELOUR are shown in Table 1. VELOUR was not designed to demonstrate a statistically significant difference in adverse reaction rates for ZALTRAP/FOLFIRI as compared to placebo/FOLFIRI for any adverse reactions listed below.
| Primary System Organ Class Preferred Term |
ZALTRAP/ FOLFIRI (N=611) |
Placebo/ FOLFIRI (N=605) |
||
|---|---|---|---|---|
| All grades (%) | Grades 3–4 (%) | All grades (%) | Grades 3–4 (%) | |
| Note: Adverse Reactions are reported using MedDRA version 13.1 and graded using NCI CTC version 3.0 | ||||
| Blood and lymphatic system disorders | ||||
| Leukopenia | 78 | 16 | 72 | 12 |
| Neutropenia | 67 | 37 | 57 | 30 |
| Thrombocytopenia | 48 | 3 | 35 | 2 |
| Gastrointestinal disorders | ||||
| Diarrhea | 69 | 19 | 57 | 8 |
| Stomatitis | 50 | 13 | 33 | 5 |
| Abdominal Pain | 27 | 4 | 24 | 2 |
| Abdominal Pain Upper | 11 | 1 | 8 | 1 |
| Hemorrhoids | 6 | 0 | 2 | 0 |
| Rectal Hemorrhage | 5 | 0.7 | 2 | 0.5 |
| Proctalgia | 5 | 0.3 | 2 | 0.3 |
| Investigations | ||||
| AST increased | 62 | 3 | 54 | 2 |
| ALT increased | 50 | 3 | 39 | 2 |
| Weight decreased | 32 | 3 | 14 | 0.8 |
| Renal and urinary disorders | ||||
| Proteinuria Compilation of clinical and laboratory data
|
62 | 8 | 41 | 1 |
| Serum creatinine increased | 23 | 0 | 19 | 0.5 |
| General disorders and administration site conditions | ||||
| Fatigue | 48 | 13 | 39 | 8 |
| Asthenia | 18 | 5 | 13 | 3 |
| Vascular disorders | ||||
| Hypertension | 41 | 19 | 11 | 1.5 |
| Metabolism and nutrition disorders | ||||
| Decreased Appetite | 32 | 3 | 24 | 2 |
| Dehydration | 9 | 4 | 3 | 1 |
| Respiratory, thoracic and mediastinal disorders | ||||
| Epistaxis | 28 | 0.2 | 7 | 0 |
| Dysphonia | 25 | 0.5 | 3 | 0 |
| Dyspnea | 12 | 0.8 | 9 | 0.8 |
| Oropharyngeal Pain | 8 | 0.2 | 3 | 0 |
| Rhinorrhea | 6 | 0 | 2 | 0 |
| Nervous system disorders | ||||
| Headache | 22 | 2 | 9 | 0.3 |
| Skin and subcutaneous tissue disorders | ||||
| Palmar-Plantar Erythrodysesthesia Syndrome | 11 | 3 | 4 | 0.5 |
| Skin Hyperpigmentation | 8 | 0 | 3 | 0 |
| Infections | ||||
| Urinary Tract Infection | 9 | 0.8 | 6 | 0.8 |
Infections occurred at a higher frequency in patients receiving ZALTRAP/FOLFIRI (46%, all grades; 12%, Grade 3–4) than in patients receiving placebo/FOLFIRI (33%, all grades; 7%, Grade 3–4), including urinary tract infection, nasopharyngitis, upper respiratory tract infection, pneumonia, catheter site infection, and tooth infection.
In patients with mCRC, severe hypersensitivity reactions have been reported with ZALTRAP/FOLFIRI (0.3%) and placebo/FOLFIRI (0.5%).
In patients with mCRC, venous thromboembolic events (VTE), consisting primarily of deep venous thrombosis and pulmonary embolism, occurred in 9% of patients treated with ZALTRAP/FOLFIRI and 7% of patients treated with placebo/FOLFIRI. Grade 3–4 VTE occurred in 8% of patients treated with ZALTRAP/FOLFIRI and in 6% of patients treated with placebo/FOLFIRI. Pulmonary embolism occurred in 5% of patients treated with ZALTRAP/FOLFIRI and 3.4% of patients treated with placebo/FOLFIRI.
5.2 Gastrointestinal Perforation
Gastrointestinal (GI) perforation including fatal GI perforation can occur in patients receiving ZALTRAP. Across three placebo-controlled clinical studies (colorectal, pancreatic, and lung cancer populations), the incidence of GI perforation (all grades) was 0.8% for patients treated with ZALTRAP and 0.3% for patients treated with placebo. Grade 3–4 GI perforation occurred in 0.8% of patients treated with ZALTRAP and 0.2% of patients treated with placebo.
Monitor patients for signs and symptoms of GI perforation. Discontinue ZALTRAP therapy in patients who experience GI perforation [see Dosage and Administration (2.2)].
2.1 Recommended Dose and Schedule
The recommended dosage of ZALTRAP is 4 mg per kg of actual body weight as an intravenous infusion over 1 hour every two weeks in combination with FOLFIRI until disease progression or unacceptable toxicity. Administer ZALTRAP prior to any component of the FOLFIRI regimen on the day of treatment.
Refer to prescribing information for irinotecan, fluorouracil, and leucovorin for the recommended dosage and dosage modifications for these drugs.
5.6 Arterial Thromboembolic Events
ATE, including transient ischemic attack, cerebrovascular accident, and angina pectoris, occurred more frequently in patients who have received ZALTRAP. In patients with mCRC, ATE was reported in 2.6% of patients treated with ZALTRAP/FOLFIRI and 1.7% of patients treated with placebo/FOLFIRI. Grade 3–4 events occurred in 11 patients (1.8%) treated with ZALTRAP/FOLFIRI and 4 patients (0.7%) treated with placebo/FOLFIRI.
Discontinue ZALTRAP in patients who experience an ATE [see Dosage and Administration (2.2)].
16 How Supplied/storage and Handling
ZALTRAP (ziv-aflibercept) injection is a clear, colorless to pale-yellow solution supplied in single-dose vials with a concentration of 25 mg/mL.
NDC 0024-5840-01: carton containing one single-dose vial of 100 mg/4 mL (25 mg/mL)
NDC 0024-5841-01: carton containing one single-dose vial of 200 mg/8 mL (25 mg/mL)
13.2 Animal Toxicology And/or Pharmacology
Repeated administration of ziv-aflibercept resulted in a delay in wound healing in rabbits. In full-thickness excisional and incisional skin wound models, ziv-aflibercept administration reduced fibrous response, neovascularization, epidermal hyperplasia/re-epithelialization, and tensile strength.
5.8 Neutropenia and Neutropenic Complications
A higher incidence of neutropenic complications (febrile neutropenia and neutropenic infection) occurred in patients receiving ZALTRAP. In patients with mCRC, Grade 3–4 neutropenia occurred in 37% of patients treated with ZALTRAP/FOLFIRI compared to 30% patients treated with placebo/FOLFIRI [see Adverse Reactions (6.1)]. Grade 3–4 febrile neutropenia occurred in 4% of patients treated with ZALTRAP/FOLFIRI compared to 2% of patients treated with placebo/FOLFIRI. Grade 3–4 neutropenic infection/sepsis occurred in 1.5% of patients treated with ZALTRAP/FOLFIRI and 1.2% of patients treated with placebo/FOLFIRI.
Monitor CBC with differential count at baseline and prior to initiation of each cycle of ZALTRAP. Delay ZALTRAP/FOLFIRI until neutrophil count is at or above 1.5 × 109/L.
2.2 Dosage Modifications for Adverse Reactions
Discontinue ZALTRAP for:
- Severe hemorrhage [see Warnings and Precautions (5.1)]
- Gastrointestinal perforation [see Warnings and Precautions (5.2)]
- Impaired wound healing [see Warnings and Precautions (5.3)]
- Fistula formation [see Warnings and Precautions (5.4)]
- Hypertensive crisis or hypertensive encephalopathy [see Warnings and Precautions (5.5)]
- Arterial thromboembolic events (ATE) [see Warnings and Precautions (5.6)]
- Nephrotic syndrome or thrombotic microangiopathy (TMA) [see Warnings and Precautions (5.7)]
- Reversible posterior leukoencephalopathy syndrome (RPLS) [see Warnings and Precautions (5.10)]
Temporarily suspend ZALTRAP:
- At least 4 weeks prior to elective surgery [see Warnings and Precautions (5.3)].
- For uncontrolled hypertension until controlled. Upon resumption, permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.5)].
- For proteinuria of 2 grams per 24 hours or more. Resume when proteinuria is less than 2 grams per 24 hours. For recurrent proteinuria, suspend ZALTRAP until proteinuria is less than 2 grams per 24 hours and then permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.7)].
8.3 Females and Males of Reproductive Potential
ZALTRAP can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Principal Display Panel 100 Mg/4 Ml Vial Carton
NDC 0024-5840-01
ZALTRAP®
(ziv-aflibercept)
Injection for
Intravenous Infusion
100 mg/4 mL
(25 mg/mL)
For intravenous infusion only.
Not to be administered by
other routes.
Hyperosmotic, must be diluted.
Single-dose vial.
Discard unused portion
Rx ONLY
sanofi
Principal Display Panel 200 Mg/8 Ml Vial Carton
NDC 0024-5841-01
ZALTRAP®
(ziv-aflibercept)
Injection for
Intravenous Infusion
200 mg/8 mL
(25 mg/mL)
For intravenous infusion only.
Not to be administered by
other routes.
Hyperosmotic, must be diluted.
Single-dose vial.
Discard unused portion
Rx ONLY
sanofi
5.10 Reversible Posterior Leukoencephalopathy Syndrome
RPLS (also known as posterior reversible encephalopathy syndrome) was reported in 0.5% of 3795 patients treated with ZALTRAP monotherapy or in combination with chemotherapy.
Confirm the diagnosis of RPLS with magnetic resonance imaging (MRI) and discontinue ZALTRAP in patients who develop RPLS. Symptoms usually resolve or improve within days, although some patients have experienced ongoing neurologic sequelae or death [see Dosage and Administration (2.2)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies have been conducted to evaluate carcinogenicity or mutagenicity of ziv-aflibercept.
Ziv-aflibercept impaired reproductive function and fertility in monkeys. In a 6-month repeat-dose toxicology study in sexually mature monkeys, ziv-aflibercept inhibited ovarian function and follicular development, as evidenced by: decreased ovary weight, decreased amount of luteal tissue, decreased number of maturing follicles, atrophy of uterine endometrium and myometrium, vaginal atrophy, abrogation of progesterone peaks and menstrual bleeding. Alterations in sperm morphology and decreased sperm motility were present in male monkeys. These effects were observed at all doses tested including the lowest dose tested, 3 mg per kg. Reversibility was observed within 18 weeks after cessation of treatment. Systemic exposure (AUC) with a 3 mg per kg per dose in monkeys was approximately 0.6 times the AUC in patients at the 4 mg per kg dose.
Structured Label Content
Section 42229-5 (42229-5)
Preparation
Inspect vials visually prior to use. ZALTRAP is a clear, colorless to pale yellow solution. Do not use vial if the solution is discolored or cloudy or if the solution contains particles.
Withdraw the prescribed dose of ZALTRAP and dilute in 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to achieve a final concentration of 0.6 mg/mL to 8 mg/mL.
Do not re-enter the vial after the initial puncture. Discard any unused portion left in the vial.
Use polyvinyl chloride (PVC) infusion bags containing bis (2-ethylhexyl) phthalate (DEHP) or polyolefin infusion bags.
Store diluted ZALTRAP refrigerated at 2°C to 8°C (36°F to 46°F) for up to 24 hours or at controlled room temperature of 20°C to 25°C (68°F to 77°F) for up to 8 hours. Discard any unused portion left in the infusion bag.
Section 44425-7 (44425-7)
Store ZALTRAP vials in a refrigerator at 2°C to 8°C (36°F to 46°F). Keep the vials in the original outer carton to protect from light. Discard unused portion.
11 Description (11 DESCRIPTION)
Ziv-aflibercept is a vascular endothelial growth factor inhibitor. It is a recombinant fusion protein consisting of Vascular Endothelial Growth Factor (VEGF)-binding portions from the extracellular domains of human VEGF Receptors 1 and 2 fused to the Fc portion of the human IgG1. Ziv-aflibercept is produced by recombinant DNA technology in a Chinese hamster ovary (CHO) K-1 mammalian expression system. Ziv-aflibercept is a dimeric glycoprotein with a protein molecular weight of 97 kilodaltons (kDa) and contains glycosylation, constituting an additional 15% of the total molecular mass, resulting in a total molecular weight of 115 kDa.
ZALTRAP (ziv-aflibercept) injection is a sterile, clear, colorless to pale-yellow, non-pyrogenic, preservative-free, solution for intravenous use. ZALTRAP is supplied in single-dose vials of 100 mg/4 mL and 200 mg/8 mL formulated as 25 mg/mL ziv-aflibercept in polysorbate 20 (1 mg/mL), sodium chloride (5.84 mg/mL), sodium citrate (1.45 mg/mL), sodium phosphate (0.8 mg/mL), and sucrose (200 mg/mL), in Water for Injection, USP, at a pH of 6.2.
5.1 Hemorrhage
Patients treated with ZALTRAP have an increased risk of hemorrhage, including severe and sometimes fatal hemorrhagic events. In patients with mCRC, bleeding/hemorrhage (all grades) was reported in 38% of patients treated with ZALTRAP/FOLFIRI compared to 19% of patients treated with placebo/FOLFIRI. Grade 3–4 hemorrhagic events, including gastrointestinal hemorrhage, hematuria, and post-procedural hemorrhage, were reported in 3% of patients receiving ZALTRAP/FOLFIRI compared with 1% of patients receiving placebo/FOLFIRI. Severe intracranial hemorrhage and pulmonary hemorrhage/hemoptysis including fatal events have also occurred in patients receiving ZALTRAP.
Monitor patients for signs and symptoms of bleeding. Do not initiate ZALTRAP in patients with severe hemorrhage. Discontinue ZALTRAP in patients who develop severe hemorrhage [see Dosage and Administration (2.2)].
5.7 Proteinuria
Severe proteinuria, nephrotic syndrome, and thrombotic microangiopathy (TMA) occurred more frequently in patients treated with ZALTRAP. In patients with mCRC, proteinuria was reported in 62% patients treated with ZALTRAP/FOLFIRI compared to 41% patients treated with placebo/FOLFIRI. Grade 3–4 proteinuria occurred in 8% of patients treated with ZALTRAP/FOLFIRI compared to 1% of patients treated with placebo/FOLFIRI [see Adverse Reactions (6.1)]. Nephrotic syndrome occurred in 2 patients (0.5%) treated with ZALTRAP/FOLFIRI compared to none of the patients treated with placebo/FOLFIRI. TMA was reported in 3 of 2258 patients with cancer enrolled across completed studies.
Monitor proteinuria by urine dipstick analysis and/or urinary protein creatinine ratio (UPCR) for the development or worsening of proteinuria during ZALTRAP therapy. Patients with a dipstick of ≥2+ for protein or a UPCR greater than 1 should undergo a 24-hour urine collection.
Suspend ZALTRAP administration for proteinuria 2 grams per 24 hours or more, and resume when proteinuria is less than 2 grams per 24 hours. If recurrent, suspend until proteinuria is less than 2 grams per 24 hours and then permanently reduce the ZALTRAP dose to 2 mg per kg. Discontinue ZALTRAP in patients who develop nephrotic syndrome or TMA [see Dosage and Administration (2.2)].
5.5 Hypertension
ZALTRAP increases the risk of Grade 3–4 hypertension. There is no clinical trial experience administering ZALTRAP to patients with NYHA class III or IV heart failure. In patients with mCRC, Grade 3 hypertension (defined as requiring adjustment in existing antihypertensive therapy or treatment with more than one drug) was reported in 1.5% of patients treated with placebo/FOLFIRI and 19% of patients treated with ZALTRAP/FOLFIRI. Grade 4 hypertension (hypertensive crisis) was reported in 1 patient (0.2%) treated with ZALTRAP/FOLFIRI. Among those patients treated with ZALTRAP/FOLFIRI developing Grade 3–4 hypertension, 54% had onset during the first two cycles of treatment.
Monitor blood pressure every two weeks or more frequently as clinically indicated during treatment with ZALTRAP. Treat with appropriate antihypertensive therapy and continue monitoring blood pressure regularly. Temporarily suspend ZALTRAP in patients with uncontrolled hypertension until controlled and permanently reduce the ZALTRAP dose to 2 mg per kg for subsequent cycles. Discontinue ZALTRAP in patients with hypertensive crisis or hypertensive encephalopathy [see Dosage and Administration (2.2)].
8.4 Pediatric Use
The safety and effectiveness in pediatric patients have not been established. Safety and efficacy were assessed, but not established in a dose-escalation, safety, and tolerability study (NCT00622414) in 21 patients with solid tumors 2 to 21 years of age (median age 12.9). The mean elimination half-life of free ziv-aflibercept determined after the first dose in 8 pediatric patients aged 5 to 17 years was within the range of values previously observed in adults. The maximum tolerated dose based on body weight in these pediatric patients was lower than the dose known to be safe and effective in adults with mCRC.
8.5 Geriatric Use
Of the 611 patients with mCRC, patients treated with ZALTRAP/FOLFIRI, 205 (34%) were 65 years or older, and 33 (5%) were 75 years or older. Elderly patients (≥65 years of age) experienced higher incidences (≥5%) of diarrhea, dizziness, asthenia, weight decrease, and dehydration when compared to younger patients. Monitor elderly patients more closely for diarrhea and dehydration [see Warnings and Precautions (5.9)].
The effect of ZALTRAP on overall survival was similar in patients <65 years old and ≥65 years old who received ZALTRAP/FOLFIRI.
6.2 Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described below with the incidence of antibodies in other studies or to other products may be misleading.
In patients with various cancers across 15 studies, 1.4% (41/2862) of patients tested positive for antiproduct antibody (APA) at baseline. The incidence of APA development was 3.1% (53/1687) in patients receiving intravenous ziv-aflibercept and 1.7% (19/1134) in patients receiving placebo. Among patients who tested positive for APA and had sufficient samples for further testing, neutralizing antibodies were detected in 17 of 48 ziv-aflibercept-treated patients and in 2 of 40 patients receiving placebo.
The mean free ziv-aflibercept trough concentrations were lower in patients with positive neutralizing antibodies than in the overall population. The impact of neutralizing antibodies on efficacy and safety could not be assessed based on limited available data.
14 Clinical Studies (14 CLINICAL STUDIES)
The efficacy of ZALTRAP was evaluated in VELOUR (NCT00561470), a randomized (1:1), double-blind, placebo-controlled study in patients with mCRC who are resistant to or have progressed during or within 6 months of receiving oxaliplatin-based combination chemotherapy, with or without prior bevacizumab. Patients were randomized to receive either ZALTRAP 4 mg per kg intravenously over 1 hour on day 1 or placebo in combination with FOLFIRI (irinotecan 180 mg/m2 intravenously over 90 minutes and leucovorin [dl racemic] 400 mg/m2 intravenously over 2 hours at the same time on day 1 using a Y-line, followed by fluorouracil 400 mg/m2 as an intravenous bolus and then by fluorouracil 2400 mg/m2 as a continuous intravenous infusion over 46 hours). The treatment cycles on both arms were repeated every 2 weeks. Patients were treated until disease progression or unacceptable toxicity. Randomization was stratified by the Eastern Cooperative Oncology Group performance status (PS) (0 versus 1 versus 2) and according to prior therapy with bevacizumab (yes or no). The major efficacy outcome measure was overall survival (OS). Additional efficacy outcome measures were progression-free survival (PFS) and overall response rate (ORR).
Demographics characteristics were similar between treatment arms. A total of 1226 patients were randomized, 612 to the ZALTRAP arm and 614 to the placebo arm. The median age was 61 years, 59% were men, 87% were White, 7% were Asian, 3.5% were Black, and 98% had a baseline ECOG PS of 0 or 1. Among the 1226 randomized patients, 89% and 90% of patients treated with placebo/FOLFIRI and ZALTRAP/FOLFIRI, respectively, received prior oxaliplatin-based combination chemotherapy in the metastatic/advanced setting. A total of 346 patients (28%) received bevacizumab in combination with the prior oxaliplatin-based treatment.
Efficacy results are summarized in Figure 1 and Table 2.
Figure 1: Kaplan-Meier Curves of Overall Survival for VELOUR
| ZALTRAP/FOLFIRI N=612 |
Placebo/FOLFIRI N=614 |
|
|---|---|---|
| Overall Survival | ||
| Number of deaths, n (%) | 403 (65.8%) | 460 (74.9%) |
| Median overall survival (95% CI) (months) | 13.50 (12.52, 14.95) | 12.06 (11.07, 13.08) |
| Stratified Hazard ratio (95% CI) | 0.817 (0.714, 0.935) | |
| Stratified Log-Rank test p-value | 0.0032 | |
| Progression Free Survival (PFS) | ||
| Number of events, n (%) | 393 (64.2%) | 454 (73.9%) |
| Median PFS (95% CI) (months) | 6.90 (6.51, 7.20) | 4.67 (4.21, 5.36) |
| Stratified Hazard ratio (95% CI) | 0.758 (0.661, 0.869) | |
| Stratified Log-Rank test p-value Stratified on ECOG Performance Status (0 vs 1 vs 2) and Prior Bevacizumab (yes vs no)
|
0.00007 | |
| Overall Response Rate (ORR) | ||
| ORR (CR+PR) (95% CI) Overall objective response rate by IRC
|
19.8% (16.4%, 23.2%) | 11.1% (8.5%, 13.8%) |
| Stratified Cochran-Mantel-Haenszel test p-value | 0.0001 |
Planned subgroup analyses for overall survival based on stratification factors at randomization yielded an HR of 0.86 (95% CI: 0.68, 1.1) in patients who received prior bevacizumab and an HR of 0.79 (95% CI: 0.67, 0.93) in patients without prior bevacizumab exposure.
4 Contraindications (4 CONTRAINDICATIONS)
None.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hemorrhage [see Warnings and Precautions (5.1)]
- Gastrointestinal Perforation [see Warnings and Precautions (5.2)]
- Impaired Wound Healing [see Warnings and Precautions (5.3)]
- Fistula Formation [see Warnings and Precautions (5.4)]
- Hypertension [see Warnings and Precautions (5.5)]
- Arterial Thromboembolic Events [see Warnings and Precautions (5.6)]
- Proteinuria [see Warnings and Precautions (5.7)]
- Neutropenia and Neutropenic Complications [see Warnings and Precautions (5.8)]
- Diarrhea and Dehydration [see Warnings and Precautions (5.9)]
- Reversible Posterior Leukoencephalopathy Syndrome [see Warnings and Precautions (5.10)]
7 Drug Interactions (7 DRUG INTERACTIONS)
No dedicated drug-drug interaction studies have been conducted for ZALTRAP. No clinically important pharmacokinetic interactions were found between ziv-aflibercept and irinotecan/SN-38 or fluorouracil [see Clinical Pharmacology (12.3)].
8.6 Renal Impairment
No dosage modification is recommended for patients with renal impairment [see Clinical Pharmacology (12.3)].
12.3 Pharmacokinetics
Plasma concentrations of free and VEGF-bound ziv-aflibercept were measured using specific enzyme-linked immunosorbent assays (ELISA). Free ziv-aflibercept concentrations appear to exhibit linear pharmacokinetics in the dose range of 2 mg per kg to 9 mg per kg. Steady state concentrations of free ziv-aflibercept were reached by the second dose. The accumulation ratio for free ziv-aflibercept was approximately 1.2 after administration of 4 mg per kg every two weeks.
5.4 Fistula Formation
Fistula formation involving gastrointestinal and non-gastrointestinal sites occurs at a higher incidence in patients treated with ZALTRAP. In patients with mCRC, fistulas (anal, enterovesical, enterocutaneous, colovaginal, intestinal sites) were reported in 9 of 611 patients (1.5%) treated with ZALTRAP/FOLFIRI regimen and 3 of 605 patients (0.5%) treated with placebo/FOLFIRI regimen. Grade 3 GI fistula formation occurred in 2 patients treated with ZALTRAP (0.3%) and in 1 patient treated with placebo (0.2%).
Discontinue ZALTRAP therapy in patients who develop fistula [see Dosage and Administration (2.2)].
8.7 Hepatic Impairment
No dosage modification is recommended for patients with mild (total bilirubin >1 to 1.5 times upper limit normal [ULN] and any aspartate transaminase [AST]) and moderate (total bilirubin >1.5 to 3 times ULN and any AST) hepatic impairment [see Clinical Pharmacology (12.3)]. ZALTRAP has not been studied in patients with severe hepatic impairment (total bilirubin >3 times ULN and any AST).
1 Indications and Usage (1 INDICATIONS AND USAGE)
ZALTRAP, in combination with fluorouracil, leucovorin, irinotecan-(FOLFIRI), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) that is resistant to or has progressed following an oxaliplatin-containing regimen.
12.1 Mechanism of Action
Ziv-aflibercept acts as a soluble receptor that binds to human VEGF-A (equilibrium dissociation constant KD of 0.5 pM for VEGF-A165 and 0.36 pM for VEGF-A121), to human VEGF-B (KD of 1.92 pM), and to human PlGF (KD of 39 pM for PlGF-2). By binding to these endogenous ligands, ziv-aflibercept can inhibit the binding and activation of their cognate receptors. This inhibition can result in decreased neovascularization and decreased vascular permeability.
In animals, ziv-aflibercept was shown to inhibit the proliferation of endothelial cells, thereby inhibiting the growth of new blood vessels. Ziv-aflibercept inhibited the growth of xenotransplanted colon tumors in mice.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Hemorrhage: Severe and sometimes fatal hemorrhage, including gastrointestinal (GI) hemorrhage, has been reported in patients who have received ZALTRAP. Do not administer ZALTRAP to patients with severe hemorrhage. (5.1)
- Gastrointestinal Perforation: Discontinue ZALTRAP therapy in patients who experience GI perforation. (5.2)
- Impaired Wound Healing: Withhold ZALTRAP for at least 4 weeks prior to elective surgery. Do not administer for at least 4 weeks following major surgery and until wounds have adequately healed. Discontinue ZALTRAP in patients with impaired wound healing. The safety of resumption of ZALTRAP after resolution of wound healing complications has not been established. (5.3)
- Fistula Formation: Discontinue ZALTRAP if fistula occurs. (2.2, 5.4)
- Hypertension: Monitor blood pressure and treat hypertension. Temporarily suspend ZALTRAP if hypertension is not controlled. Discontinue ZALTRAP if hypertensive crisis develops. (2.2, 5.5)
- Arterial Thromboembolic Events (ATE): Discontinue ZALTRAP if ATE develops. (5.6)
- Proteinuria: Monitor urine protein. Suspend ZALTRAP for proteinuria of 2 grams per 24 hours or more. Discontinue ZALTRAP if nephrotic syndrome or thrombotic microangiopathy (TMA) develops. (2.2, 5.7)
- Neutropenia and Neutropenic Complications: Delay administration of ZALTRAP/FOLFIRI until neutrophil count is 1.5 × 109/L or higher. (5.8)
- Diarrhea and Dehydration: Incidence of severe diarrhea and dehydration is increased. Monitor elderly patients more closely. (5.9, 8.5)
- Reversible Posterior Leukoencephalopathy Syndrome: Discontinue ZALTRAP. (5.10)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of potential risk to fetus and need for use of effective contraception. (5.11, 8.1, 8.3)
5.11 Embryo Fetal Toxicity (5.11 Embryo-Fetal Toxicity)
Based on findings from animal studies and its mechanism of action, ZALTRAP can cause fetal harm when administered to pregnant women. Administration of ziv-aflibercept during the period of organogenesis was embryotoxic and teratogenic in rabbits at exposure levels approximately 0.3 times the human exposure at the 4 mg per kg dose. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with ZALTRAP and for 3 months following the last dose [see Use in Specific Populations (8.1, 8.3)].
5.3 Impaired Wound Healing
Grade 3 impaired wound healing was reported in 2 patients (0.3%) treated with ZALTRAP/FOLFIRI regimen.
Withhold ZALTRAP for at least 4 weeks prior to elective surgery. Do not administer ZALTRAP for at least 4 weeks after major surgery and until wounds have adequately healed. For minor surgery such as central venous access port placement, biopsy, and tooth extraction, ZALTRAP may be initiated/resumed once the surgical wound is fully healed. Discontinue ZALTRAP in patients with impaired wound healing. The safety of resumption of ZALTRAP after resolution of wound healing complications has not been established [see Dosage and Administration (2.2)].
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
ZALTRAP is a clear, colorless to pale-yellow solution available as:
- Injection: 100 mg/4 mL (25 mg/mL) solution in a single-dose vial
- Injection: 200 mg/8 mL (25 mg/mL) solution in a single-dose vial
5.9 Diarrhea and Dehydration
The incidence of severe diarrhea is increased in patients treated with ZALTRAP/FOLFIRI. In patients with mCRC, Grade 3–4 diarrhea was reported in 19% of patients treated with ZALTRAP/FOLFIRI compared to 8% of patients treated with placebo/FOLFIRI. Grade 3–4 dehydration was reported in 4% of patients treated with ZALTRAP/FOLFIRI compared to 1% of patients treated with placebo/FOLFIRI [see Adverse Reactions (6.1)]. The incidence of diarrhea is increased in patients who are age 65 years or older as compared to patients younger than 65 years of age [see Use in Specific Populations (8.5)]. Monitor elderly patients closely for diarrhea.
6.3 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of ZALTRAP. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Musculoskeletal and connective tissue disorders: Osteonecrosis of the jaw
Cardiac disorders: Cardiac failure, ejection fraction decreased
Vascular disorders: Arterial (including aortic) aneurysms, dissections, and rupture
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Lactation: Advise not to breastfeed. (8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of ZALTRAP in combination with FOLFIRI was evaluated in VELOUR (EFC102621) [see Clinical Studies (14)]. Patients received ZALTRAP 4 mg per kg (N=611) or placebo (N=605) intravenously every two weeks (one cycle) in combination with FOLFIRI. Patients received a median of 9 cycles of ZALTRAP/FOLFIRI.
The most common Grade 3–4 adverse reactions (≥5%) in the ZALTRAP/FOLFIRI arm were neutropenia, diarrhea, hypertension, leukopenia, stomatitis, fatigue, proteinuria, and asthenia.
The most frequent adverse reactions leading to permanent discontinuation in ≥1% of patients treated with ZALTRAP/FOLFIRI regimen were asthenia/fatigue, infections, diarrhea, dehydration, hypertension, stomatitis, venous thromboembolic events, neutropenia, and proteinuria.
The ZALTRAP dose was reduced and/or omitted in 17% of patients. Cycle delays >7 days occurred in 60% of patients treated with ZALTRAP/FOLFIRI.
The most common adverse reactions (≥20%) in the ZALTRAP/FOLFIRI arm were leukopenia, diarrhea, neutropenia, proteinuria, AST increased, stomatitis, fatigue, thrombocytopenia, ALT increased, hypertension, weight decreased, decreased appetite, epistaxis, abdominal pain, dysphonia, serum creatinine increased, and headache.
Adverse reactions and laboratory abnormalities that occurred in ≥5% (all grades) of patients receiving ZALTRAP in combination with FOLFIRI and which occurred at ≥2% higher frequency in patients who received ZALTRAP/FOLFIRI compared to those who received placebo/FOLFIRI in VELOUR are shown in Table 1. VELOUR was not designed to demonstrate a statistically significant difference in adverse reaction rates for ZALTRAP/FOLFIRI as compared to placebo/FOLFIRI for any adverse reactions listed below.
| Primary System Organ Class Preferred Term |
ZALTRAP/ FOLFIRI (N=611) |
Placebo/ FOLFIRI (N=605) |
||
|---|---|---|---|---|
| All grades (%) | Grades 3–4 (%) | All grades (%) | Grades 3–4 (%) | |
| Note: Adverse Reactions are reported using MedDRA version 13.1 and graded using NCI CTC version 3.0 | ||||
| Blood and lymphatic system disorders | ||||
| Leukopenia | 78 | 16 | 72 | 12 |
| Neutropenia | 67 | 37 | 57 | 30 |
| Thrombocytopenia | 48 | 3 | 35 | 2 |
| Gastrointestinal disorders | ||||
| Diarrhea | 69 | 19 | 57 | 8 |
| Stomatitis | 50 | 13 | 33 | 5 |
| Abdominal Pain | 27 | 4 | 24 | 2 |
| Abdominal Pain Upper | 11 | 1 | 8 | 1 |
| Hemorrhoids | 6 | 0 | 2 | 0 |
| Rectal Hemorrhage | 5 | 0.7 | 2 | 0.5 |
| Proctalgia | 5 | 0.3 | 2 | 0.3 |
| Investigations | ||||
| AST increased | 62 | 3 | 54 | 2 |
| ALT increased | 50 | 3 | 39 | 2 |
| Weight decreased | 32 | 3 | 14 | 0.8 |
| Renal and urinary disorders | ||||
| Proteinuria Compilation of clinical and laboratory data
|
62 | 8 | 41 | 1 |
| Serum creatinine increased | 23 | 0 | 19 | 0.5 |
| General disorders and administration site conditions | ||||
| Fatigue | 48 | 13 | 39 | 8 |
| Asthenia | 18 | 5 | 13 | 3 |
| Vascular disorders | ||||
| Hypertension | 41 | 19 | 11 | 1.5 |
| Metabolism and nutrition disorders | ||||
| Decreased Appetite | 32 | 3 | 24 | 2 |
| Dehydration | 9 | 4 | 3 | 1 |
| Respiratory, thoracic and mediastinal disorders | ||||
| Epistaxis | 28 | 0.2 | 7 | 0 |
| Dysphonia | 25 | 0.5 | 3 | 0 |
| Dyspnea | 12 | 0.8 | 9 | 0.8 |
| Oropharyngeal Pain | 8 | 0.2 | 3 | 0 |
| Rhinorrhea | 6 | 0 | 2 | 0 |
| Nervous system disorders | ||||
| Headache | 22 | 2 | 9 | 0.3 |
| Skin and subcutaneous tissue disorders | ||||
| Palmar-Plantar Erythrodysesthesia Syndrome | 11 | 3 | 4 | 0.5 |
| Skin Hyperpigmentation | 8 | 0 | 3 | 0 |
| Infections | ||||
| Urinary Tract Infection | 9 | 0.8 | 6 | 0.8 |
Infections occurred at a higher frequency in patients receiving ZALTRAP/FOLFIRI (46%, all grades; 12%, Grade 3–4) than in patients receiving placebo/FOLFIRI (33%, all grades; 7%, Grade 3–4), including urinary tract infection, nasopharyngitis, upper respiratory tract infection, pneumonia, catheter site infection, and tooth infection.
In patients with mCRC, severe hypersensitivity reactions have been reported with ZALTRAP/FOLFIRI (0.3%) and placebo/FOLFIRI (0.5%).
In patients with mCRC, venous thromboembolic events (VTE), consisting primarily of deep venous thrombosis and pulmonary embolism, occurred in 9% of patients treated with ZALTRAP/FOLFIRI and 7% of patients treated with placebo/FOLFIRI. Grade 3–4 VTE occurred in 8% of patients treated with ZALTRAP/FOLFIRI and in 6% of patients treated with placebo/FOLFIRI. Pulmonary embolism occurred in 5% of patients treated with ZALTRAP/FOLFIRI and 3.4% of patients treated with placebo/FOLFIRI.
5.2 Gastrointestinal Perforation
Gastrointestinal (GI) perforation including fatal GI perforation can occur in patients receiving ZALTRAP. Across three placebo-controlled clinical studies (colorectal, pancreatic, and lung cancer populations), the incidence of GI perforation (all grades) was 0.8% for patients treated with ZALTRAP and 0.3% for patients treated with placebo. Grade 3–4 GI perforation occurred in 0.8% of patients treated with ZALTRAP and 0.2% of patients treated with placebo.
Monitor patients for signs and symptoms of GI perforation. Discontinue ZALTRAP therapy in patients who experience GI perforation [see Dosage and Administration (2.2)].
2.1 Recommended Dose and Schedule
The recommended dosage of ZALTRAP is 4 mg per kg of actual body weight as an intravenous infusion over 1 hour every two weeks in combination with FOLFIRI until disease progression or unacceptable toxicity. Administer ZALTRAP prior to any component of the FOLFIRI regimen on the day of treatment.
Refer to prescribing information for irinotecan, fluorouracil, and leucovorin for the recommended dosage and dosage modifications for these drugs.
5.6 Arterial Thromboembolic Events
ATE, including transient ischemic attack, cerebrovascular accident, and angina pectoris, occurred more frequently in patients who have received ZALTRAP. In patients with mCRC, ATE was reported in 2.6% of patients treated with ZALTRAP/FOLFIRI and 1.7% of patients treated with placebo/FOLFIRI. Grade 3–4 events occurred in 11 patients (1.8%) treated with ZALTRAP/FOLFIRI and 4 patients (0.7%) treated with placebo/FOLFIRI.
Discontinue ZALTRAP in patients who experience an ATE [see Dosage and Administration (2.2)].
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
ZALTRAP (ziv-aflibercept) injection is a clear, colorless to pale-yellow solution supplied in single-dose vials with a concentration of 25 mg/mL.
NDC 0024-5840-01: carton containing one single-dose vial of 100 mg/4 mL (25 mg/mL)
NDC 0024-5841-01: carton containing one single-dose vial of 200 mg/8 mL (25 mg/mL)
13.2 Animal Toxicology And/or Pharmacology (13.2 Animal Toxicology and/or Pharmacology)
Repeated administration of ziv-aflibercept resulted in a delay in wound healing in rabbits. In full-thickness excisional and incisional skin wound models, ziv-aflibercept administration reduced fibrous response, neovascularization, epidermal hyperplasia/re-epithelialization, and tensile strength.
5.8 Neutropenia and Neutropenic Complications
A higher incidence of neutropenic complications (febrile neutropenia and neutropenic infection) occurred in patients receiving ZALTRAP. In patients with mCRC, Grade 3–4 neutropenia occurred in 37% of patients treated with ZALTRAP/FOLFIRI compared to 30% patients treated with placebo/FOLFIRI [see Adverse Reactions (6.1)]. Grade 3–4 febrile neutropenia occurred in 4% of patients treated with ZALTRAP/FOLFIRI compared to 2% of patients treated with placebo/FOLFIRI. Grade 3–4 neutropenic infection/sepsis occurred in 1.5% of patients treated with ZALTRAP/FOLFIRI and 1.2% of patients treated with placebo/FOLFIRI.
Monitor CBC with differential count at baseline and prior to initiation of each cycle of ZALTRAP. Delay ZALTRAP/FOLFIRI until neutrophil count is at or above 1.5 × 109/L.
2.2 Dosage Modifications for Adverse Reactions
Discontinue ZALTRAP for:
- Severe hemorrhage [see Warnings and Precautions (5.1)]
- Gastrointestinal perforation [see Warnings and Precautions (5.2)]
- Impaired wound healing [see Warnings and Precautions (5.3)]
- Fistula formation [see Warnings and Precautions (5.4)]
- Hypertensive crisis or hypertensive encephalopathy [see Warnings and Precautions (5.5)]
- Arterial thromboembolic events (ATE) [see Warnings and Precautions (5.6)]
- Nephrotic syndrome or thrombotic microangiopathy (TMA) [see Warnings and Precautions (5.7)]
- Reversible posterior leukoencephalopathy syndrome (RPLS) [see Warnings and Precautions (5.10)]
Temporarily suspend ZALTRAP:
- At least 4 weeks prior to elective surgery [see Warnings and Precautions (5.3)].
- For uncontrolled hypertension until controlled. Upon resumption, permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.5)].
- For proteinuria of 2 grams per 24 hours or more. Resume when proteinuria is less than 2 grams per 24 hours. For recurrent proteinuria, suspend ZALTRAP until proteinuria is less than 2 grams per 24 hours and then permanently reduce the ZALTRAP dose to 2 mg per kg [see Warnings and Precautions (5.7)].
8.3 Females and Males of Reproductive Potential
ZALTRAP can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Principal Display Panel 100 Mg/4 Ml Vial Carton (PRINCIPAL DISPLAY PANEL - 100 mg/4 mL Vial Carton)
NDC 0024-5840-01
ZALTRAP®
(ziv-aflibercept)
Injection for
Intravenous Infusion
100 mg/4 mL
(25 mg/mL)
For intravenous infusion only.
Not to be administered by
other routes.
Hyperosmotic, must be diluted.
Single-dose vial.
Discard unused portion
Rx ONLY
sanofi
Principal Display Panel 200 Mg/8 Ml Vial Carton (PRINCIPAL DISPLAY PANEL - 200 mg/8 mL Vial Carton)
NDC 0024-5841-01
ZALTRAP®
(ziv-aflibercept)
Injection for
Intravenous Infusion
200 mg/8 mL
(25 mg/mL)
For intravenous infusion only.
Not to be administered by
other routes.
Hyperosmotic, must be diluted.
Single-dose vial.
Discard unused portion
Rx ONLY
sanofi
5.10 Reversible Posterior Leukoencephalopathy Syndrome
RPLS (also known as posterior reversible encephalopathy syndrome) was reported in 0.5% of 3795 patients treated with ZALTRAP monotherapy or in combination with chemotherapy.
Confirm the diagnosis of RPLS with magnetic resonance imaging (MRI) and discontinue ZALTRAP in patients who develop RPLS. Symptoms usually resolve or improve within days, although some patients have experienced ongoing neurologic sequelae or death [see Dosage and Administration (2.2)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies have been conducted to evaluate carcinogenicity or mutagenicity of ziv-aflibercept.
Ziv-aflibercept impaired reproductive function and fertility in monkeys. In a 6-month repeat-dose toxicology study in sexually mature monkeys, ziv-aflibercept inhibited ovarian function and follicular development, as evidenced by: decreased ovary weight, decreased amount of luteal tissue, decreased number of maturing follicles, atrophy of uterine endometrium and myometrium, vaginal atrophy, abrogation of progesterone peaks and menstrual bleeding. Alterations in sperm morphology and decreased sperm motility were present in male monkeys. These effects were observed at all doses tested including the lowest dose tested, 3 mg per kg. Reversibility was observed within 18 weeks after cessation of treatment. Systemic exposure (AUC) with a 3 mg per kg per dose in monkeys was approximately 0.6 times the AUC in patients at the 4 mg per kg dose.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:47:15.746244 · Updated: 2026-03-14T22:48:18.981660