nitrogen nf bulk liquid
f49fbee2-8a80-477a-969b-f891ee601dc3
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Description
AIR LIQUIDE NITROGEN N.F. Form Number: 2A-ALL-QUA-0003-F Revision: 0 Effective Date: 03/02/06 Page: 1/1 CERTIFICATE OF ANALYSIS Air Liquide large Industries U.S. L.P. – Houston, TX 77056 PRODUCED BY AIR LIQUEFACTION 1.Location Street Address1 2. Carrier ________________ Street Address 2 City, State Zip 3. Lot Number ______________________ 4. Trailer No _____________ PRE-FILL REPORT FILL REPORT 5.Residual Assay 6. Odor 7. Trailer loaded with appropriate product per appropriate (≤10 ppm O 2 ) Detected loading procedure by: _______ ppm Yes No Signature _________________________ ________ ________ Date _____________________________ Initial Initial ANALYSIS REPORT Test required Method of Analysis Specifications Results ASSAY AND 8.PARAMAGNETIC ___ 99.998% N 2 Minimum* 10. ____% IDENTIFICATION MICROFUEL CELL ___ ELECTROCHEMICAL ___ CELL 10 ppm O 2 Maximum 11. _____ppm 9.Analyzer Tag Number 12.DETECTPR TUBE ___ 10 ppm CO Maximum 14. _____ppm CARBON INFARED ANALYZER ___ Expiration Date of Tube 15. ______ MONOXIDE Lot Number of Tube 16. ______ 13. Analyzer Tag Number ODOR Organoleptic (Nasal) None 17. ______ N.F. applies only when used in a medical application or by medical customers properly registered with the FDA. * Plus inerts 18. Analyzed By ________________________ Date ____________ 19. Does this lot require additional testing? ___ NO ___ YES – attach page 2 20. SQCU Review/Release _______________________ Date ____________ MANDATORY FORM User must assure that this revision of the form is current prior to use. Completed forms become permanent records subject to the record retention policy.
Medication Information
Description
AIR LIQUIDE NITROGEN N.F. Form Number: 2A-ALL-QUA-0003-F Revision: 0 Effective Date: 03/02/06 Page: 1/1 CERTIFICATE OF ANALYSIS Air Liquide large Industries U.S. L.P. – Houston, TX 77056 PRODUCED BY AIR LIQUEFACTION 1.Location Street Address1 2. Carrier ________________ Street Address 2 City, State Zip 3. Lot Number ______________________ 4. Trailer No _____________ PRE-FILL REPORT FILL REPORT 5.Residual Assay 6. Odor 7. Trailer loaded with appropriate product per appropriate (≤10 ppm O 2 ) Detected loading procedure by: _______ ppm Yes No Signature _________________________ ________ ________ Date _____________________________ Initial Initial ANALYSIS REPORT Test required Method of Analysis Specifications Results ASSAY AND 8.PARAMAGNETIC ___ 99.998% N 2 Minimum* 10. ____% IDENTIFICATION MICROFUEL CELL ___ ELECTROCHEMICAL ___ CELL 10 ppm O 2 Maximum 11. _____ppm 9.Analyzer Tag Number 12.DETECTPR TUBE ___ 10 ppm CO Maximum 14. _____ppm CARBON INFARED ANALYZER ___ Expiration Date of Tube 15. ______ MONOXIDE Lot Number of Tube 16. ______ 13. Analyzer Tag Number ODOR Organoleptic (Nasal) None 17. ______ N.F. applies only when used in a medical application or by medical customers properly registered with the FDA. * Plus inerts 18. Analyzed By ________________________ Date ____________ 19. Does this lot require additional testing? ___ NO ___ YES – attach page 2 20. SQCU Review/Release _______________________ Date ____________ MANDATORY FORM User must assure that this revision of the form is current prior to use. Completed forms become permanent records subject to the record retention policy.
Nitrogen N.f. Coa
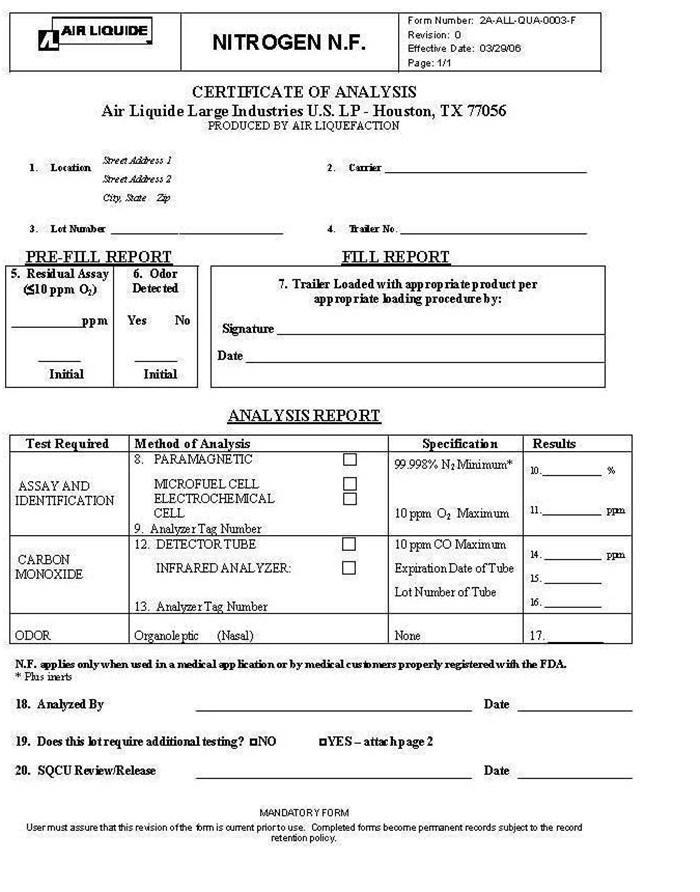
AIR LIQUIDE NITROGEN N.F. Form Number: 2A-ALL-QUA-0003-F
Revision: 0
Effective Date: 03/02/06
Page: 1/1
CERTIFICATE OF ANALYSIS
Air Liquide large Industries U.S. L.P. – Houston, TX 77056
PRODUCED BY AIR LIQUEFACTION
1.Location Street Address1 2. Carrier ________________
Street Address 2
City, State Zip
3. Lot Number ______________________ 4. Trailer No _____________
PRE-FILL REPORT FILL REPORT
5.Residual Assay 6. Odor 7. Trailer loaded with appropriate product per appropriate
(≤10 ppm O2) Detected loading procedure by:
_______ ppm Yes No Signature _________________________
________ ________ Date _____________________________
Initial Initial
ANALYSIS REPORT
Test required Method of Analysis Specifications Results
ASSAY AND 8.PARAMAGNETIC ___ 99.998% N2 Minimum* 10. ____%
IDENTIFICATION MICROFUEL CELL ___
ELECTROCHEMICAL ___
CELL 10 ppm O2 Maximum 11. _____ppm
9.Analyzer Tag Number
12.DETECTPR TUBE ___ 10 ppm CO Maximum 14. _____ppm
CARBON INFARED ANALYZER ___ Expiration Date of Tube 15. ______
MONOXIDE Lot Number of Tube 16. ______
13. Analyzer Tag Number
ODOR Organoleptic (Nasal) None 17. ______
N.F. applies only when used in a medical application or by medical customers properly registered with the FDA.
* Plus inerts
18. Analyzed By ________________________ Date ____________
19. Does this lot require additional testing? ___ NO ___ YES – attach page 2
20. SQCU Review/Release _______________________ Date ____________
MANDATORY FORM
User must assure that this revision of the form is current prior to use. Completed forms become permanent records subject to the record retention policy.
Structured Label Content
Nitrogen N.f. Coa (Nitrogen N.F. COA)
AIR LIQUIDE NITROGEN N.F. Form Number: 2A-ALL-QUA-0003-F
Revision: 0
Effective Date: 03/02/06
Page: 1/1
CERTIFICATE OF ANALYSIS
Air Liquide large Industries U.S. L.P. – Houston, TX 77056
PRODUCED BY AIR LIQUEFACTION
1.Location Street Address1 2. Carrier ________________
Street Address 2
City, State Zip
3. Lot Number ______________________ 4. Trailer No _____________
PRE-FILL REPORT FILL REPORT
5.Residual Assay 6. Odor 7. Trailer loaded with appropriate product per appropriate
(≤10 ppm O2) Detected loading procedure by:
_______ ppm Yes No Signature _________________________
________ ________ Date _____________________________
Initial Initial
ANALYSIS REPORT
Test required Method of Analysis Specifications Results
ASSAY AND 8.PARAMAGNETIC ___ 99.998% N2 Minimum* 10. ____%
IDENTIFICATION MICROFUEL CELL ___
ELECTROCHEMICAL ___
CELL 10 ppm O2 Maximum 11. _____ppm
9.Analyzer Tag Number
12.DETECTPR TUBE ___ 10 ppm CO Maximum 14. _____ppm
CARBON INFARED ANALYZER ___ Expiration Date of Tube 15. ______
MONOXIDE Lot Number of Tube 16. ______
13. Analyzer Tag Number
ODOR Organoleptic (Nasal) None 17. ______
N.F. applies only when used in a medical application or by medical customers properly registered with the FDA.
* Plus inerts
18. Analyzed By ________________________ Date ____________
19. Does this lot require additional testing? ___ NO ___ YES – attach page 2
20. SQCU Review/Release _______________________ Date ____________
MANDATORY FORM
User must assure that this revision of the form is current prior to use. Completed forms become permanent records subject to the record retention policy.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:45:02.406878 · Updated: 2026-03-14T22:21:43.238921