Talzenna
f2423edd-6d24-495c-aec1-c2f457f08d9a
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Dosage and Administration
Contraindications
None.
Warnings and Precautions
• Myelodysplastic Syndrome/Acute Myeloid Leukemia (MDS/AML) : MDS/AML occurred in patients exposed to TALZENNA, and some cases were fatal. Monitor patients for hematological toxicity and discontinue if MDS/AML is confirmed. ( 5.1 ) • Myelosuppression : TALZENNA may affect hematopoiesis and can cause anemia, neutropenia, and/or thrombocytopenia. ( 5.2 ) • Embryo-Fetal Toxicity : TALZENNA can cause fetal harm. Advise of the potential risk to the fetus and to use effective contraception. ( 5.3 , 8.1 , 8.3 )
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: • Myelodysplastic Syndrome/Acute Myeloid Leukemia [see Warnings and Precautions (5.1) ] • Myelosuppression [see Warnings and Precautions (5.2) ]
Drug Interactions
How Supplied
TALZENNA is supplied in strengths and package configurations as described in Table 12: Table 12. TALZENNA Capsules Package Configuration Capsule Strength (mg) NDC Print Bottles of 30 capsules 0.1 NDC 0069-1031-30 White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black). Bottles of 30 capsules 0.25 NDC 0069-0296-30 Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black). Bottles of 30 capsules 0.35 NDC 0069-1235-30 Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black). Bottles of 30 capsules 0.5 NDC 0069-1501-30 Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black). Bottles of 30 capsules 0.75 NDC 0069-1751-30 Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black). Bottles of 30 capsules 1 NDC 0069-1195-30 Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black).
Storage and Handling
TALZENNA is supplied in strengths and package configurations as described in Table 12: Table 12. TALZENNA Capsules Package Configuration Capsule Strength (mg) NDC Print Bottles of 30 capsules 0.1 NDC 0069-1031-30 White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black). Bottles of 30 capsules 0.25 NDC 0069-0296-30 Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black). Bottles of 30 capsules 0.35 NDC 0069-1235-30 Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black). Bottles of 30 capsules 0.5 NDC 0069-1501-30 Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black). Bottles of 30 capsules 0.75 NDC 0069-1751-30 Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black). Bottles of 30 capsules 1 NDC 0069-1195-30 Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black).
Description
Medication Information
Warnings and Precautions
• Myelodysplastic Syndrome/Acute Myeloid Leukemia (MDS/AML) : MDS/AML occurred in patients exposed to TALZENNA, and some cases were fatal. Monitor patients for hematological toxicity and discontinue if MDS/AML is confirmed. ( 5.1 ) • Myelosuppression : TALZENNA may affect hematopoiesis and can cause anemia, neutropenia, and/or thrombocytopenia. ( 5.2 ) • Embryo-Fetal Toxicity : TALZENNA can cause fetal harm. Advise of the potential risk to the fetus and to use effective contraception. ( 5.3 , 8.1 , 8.3 )
Indications and Usage
Dosage and Administration
Contraindications
None.
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: • Myelodysplastic Syndrome/Acute Myeloid Leukemia [see Warnings and Precautions (5.1) ] • Myelosuppression [see Warnings and Precautions (5.2) ]
Drug Interactions
Storage and Handling
TALZENNA is supplied in strengths and package configurations as described in Table 12: Table 12. TALZENNA Capsules Package Configuration Capsule Strength (mg) NDC Print Bottles of 30 capsules 0.1 NDC 0069-1031-30 White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black). Bottles of 30 capsules 0.25 NDC 0069-0296-30 Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black). Bottles of 30 capsules 0.35 NDC 0069-1235-30 Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black). Bottles of 30 capsules 0.5 NDC 0069-1501-30 Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black). Bottles of 30 capsules 0.75 NDC 0069-1751-30 Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black). Bottles of 30 capsules 1 NDC 0069-1195-30 Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black).
How Supplied
TALZENNA is supplied in strengths and package configurations as described in Table 12: Table 12. TALZENNA Capsules Package Configuration Capsule Strength (mg) NDC Print Bottles of 30 capsules 0.1 NDC 0069-1031-30 White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black). Bottles of 30 capsules 0.25 NDC 0069-0296-30 Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black). Bottles of 30 capsules 0.35 NDC 0069-1235-30 Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black). Bottles of 30 capsules 0.5 NDC 0069-1501-30 Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black). Bottles of 30 capsules 0.75 NDC 0069-1751-30 Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black). Bottles of 30 capsules 1 NDC 0069-1195-30 Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black).
Description
Section 42229-5
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
Section 42230-3
| This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 6/2025 | |
|
PATIENT INFORMATION
|
|
|
What is the most important information I should know about TALZENNA?
|
|
|
○ weakness ○ weight loss ○ fever ○ frequent infections |
○ blood in urine or stool ○ shortness of breath ○ feeling very tired ○ bruising or bleeding more easily |
|
Your healthcare provider will do blood tests to check your blood cell counts: ○ every month during treatment with TALZENNA. ○ weekly if you have low blood cell counts that last a long time. Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with TALZENNA if you get certain side effects. See “What are the possible side effects of TALZENNA?” below for other side effects of TALZENNA. |
|
|
What is TALZENNA?
It is not known if TALZENNA is safe and effective in children. |
|
|
Before taking TALZENNA, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Taking TALZENNA with certain other medicines can affect how TALZENNA works and may cause side effects. |
|
|
How should I take TALZENNA?
|
|
|
What are the possible side effects of TALZENNA? TALZENNA may cause serious side effects, including: The most common side effects of TALZENNA when taken alone include: |
|
|
|
|
The most common side effects of TALZENNA when taken in combination with enzalutamide include: |
|
|
|
|
TALZENNA may cause fertility problems in males. This may affect your ability to father a child. Talk to your healthcare provider if this is a concern for you. These are not all of the possible side effects of TALZENNA. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
How should I store TALZENNA?
Keep TALZENNA and all medicines out of the reach of children. |
|
|
General information about the safe and effective use of TALZENNA.
|
|
|
What are the ingredients in TALZENNA?
|
Section 44425-7
Storage
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F). [See USP Controlled Room Temperature].
1.1 Brca
TALZENNA is indicated as a single agent for the treatment of adult patients with deleterious or suspected deleterious germline breast cancer susceptibility gene (BRCA)-mutated (gBRCAm) human epidermal growth factor receptor 2 (HER2)-negative locally advanced or metastatic breast cancer. Select patients for therapy based on an FDA-approved companion diagnostic for TALZENNA [see Dosage and Administration (2.1)].
8.1 Pregnancy
Risk Summary
Based on findings from animal studies and its mechanism of action [see Clinical Pharmacology (12.1)], TALZENNA can cause embryo-fetal harm when administered to a pregnant woman. There are no available data on TALZENNA use in pregnant women to inform a drug-associated risk. In an animal reproduction study, the administration of talazoparib to pregnant rats during the period of organogenesis caused fetal malformations and structural skeletal variations and embryo-fetal death at maternal exposures that were 0.24 times the AUC in patients receiving the recommended dose of 1 mg daily (see Data). Apprise pregnant women and females of reproductive potential of the potential risk to a fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the general U.S. population, the estimated background risks of major birth defects and miscarriage in clinically recognized pregnancies are 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In an embryo-fetal development toxicity study, pregnant rats received oral doses of 0.015, 0.05, and 0.15 mg/kg/day talazoparib during the period of organogenesis. Talazoparib caused embryo-fetal death at doses ≥0.015 mg/kg/day (approximately 0.24 times the AUC in patients at the recommended dose of 1 mg daily). A dose of 0.015 mg/kg/day caused decreased fetal body weights and an increased incidence of fetal malformations (depressed eye bulge, small eye, split sternebra, and fused cervical vertebral arch) and structural variations including misshapen or incomplete ossification of the sternebra, skull, rib, and vertebra.
8.2 Lactation
Risk Summary
There are no data on the presence of talazoparib in human milk, the effects of the drug on milk production, or the effects of the drug on the breastfed child. Because of the potential for serious adverse reactions in a breastfed child from talazoparib, advise lactating women not to breastfeed during treatment with TALZENNA and for 1 month after the last dose.
11 Description
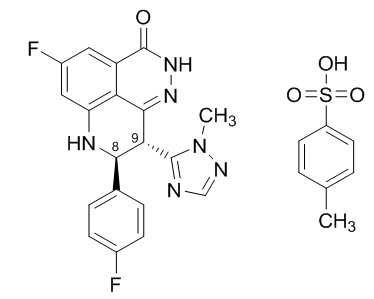
Talazoparib is an inhibitor of mammalian polyadenosine 5'-diphosphoribose (ADP-ribose) polymerase (PARP) enzymes. The chemical name of talazoparib tosylate is (8S,9R)-5-Fluoro-8-(4-fluorophenyl)-9-(1-methyl-1H-1,2,4-triazol-5-yl)-2,7,8,9-tetrahydro-3H-pyrido[4,3,2-de]phthalazin-3-one 4-methylbenzenesulfonate (1:1). The chemical formula of talazoparib tosylate is C26H22F2N6O4S, and the relative molecular mass is 552.56 Daltons. The chemical structure of talazoparib tosylate is shown below:
Talazoparib tosylate is a white to yellow solid. TALZENNA capsules for oral use are available as:
-
•0.1 mg hard hypromellose (HPMC) capsule that contains 0.145 mg talazoparib tosylate equivalent to 0.1 mg talazoparib free base, or
-
•0.25 mg HPMC capsule that contains 0.363 mg talazoparib tosylate equivalent to 0.25 mg talazoparib free base, or
-
•0.35 mg HPMC capsule that contains 0.509 mg talazoparib tosylate equivalent to 0.35 mg talazoparib free base, or
-
•0.5 mg HPMC capsule that contains 0.727 mg talazoparib tosylate equivalent to 0.5 mg talazoparib free base, or
-
•0.75 mg HPMC capsule that contains 1.09 mg talazoparib tosylate equivalent to 0.75 mg talazoparib free base, or
-
•1 mg HPMC capsule that contains 1.453 mg talazoparib tosylate equivalent to 1 mg talazoparib free base.
Inactive ingredients: silicified microcrystalline cellulose (sMCC). The capsule shells contain hypromellose (HPMC), yellow iron oxide, red iron oxide and titanium dioxide; and the printing ink contains shellac, black iron oxide, potassium hydroxide, ammonium hydroxide, and propylene glycol.
8.4 Pediatric Use
The safety and effectiveness of TALZENNA have not been established in pediatric patients.
8.5 Geriatric Use
In clinical trials of TALZENNA enrolling 494 patients with advanced solid tumors who received TALZENNA 1 mg daily as a single agent, 85 (17%) patients were ≥65 years of age, and this included 19 (4%) patients who were ≥75 years old. There were 5 patients ≥85 years old. In the TALAPRO-2 trial, of 197 patients who received TALZENNA, 77% were ≥65 years of age, while 30% were ≥75 years of age. No overall differences in safety or effectiveness of TALZENNA were observed between these patients and younger patients.
2.4 Administration
Take TALZENNA with or without food.
Swallow TALZENNA capsules whole. Do not open or dissolve.
If a patient vomits or misses a dose of TALZENNA, instruct them to take the next prescribed dose at the usual time.
14 Clinical Studies
4 Contraindications
None.
6 Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling:
-
•Myelodysplastic Syndrome/Acute Myeloid Leukemia [see Warnings and Precautions (5.1)]
-
•Myelosuppression [see Warnings and Precautions (5.2)]
7 Drug Interactions
5.2 Myelosuppression
Myelosuppression consisting of anemia, neutropenia, and/or thrombocytopenia, have been reported in patients treated with TALZENNA [see Adverse Reactions (6.1)].
Grade ≥3 anemia, neutropenia, and thrombocytopenia were reported, respectively, in 39%, 21%, and 15% of patients receiving TALZENNA as a single agent. Discontinuation due to anemia, neutropenia, and thrombocytopenia occurred, respectively, in 0.7%, 0.3%, and 0.3% of patients.
In TALAPRO-2, Grade ≥3 anemia, neutropenia, and thrombocytopenia were reported, respectively, in 48%, 19%, and 9% of patients receiving TALZENNA and enzalutamide. Forty-two percent of patients (216/511) required a red blood cell transfusion, including 25% (127/511) who required more than one transfusion. Discontinuation due to anemia, neutropenia, and thrombocytopenia occurred, respectively, in 8%, 3%, and 0.4% of patients.
Withhold TALZENNA until patients have adequately recovered from hematological toxicity caused by previous therapy. Monitor blood counts monthly during treatment with TALZENNA. If hematological toxicities do not resolve within 28 days, discontinue TALZENNA and refer the patient to a hematologist for further investigations including bone marrow analysis and blood sample for cytogenetics [see Dosage and Administration (2.5)].
8.7 Renal Impairment
Reduce the recommended dosage of TALZENNA in patients with moderate (CLcr 30 – 59 mL/min) and severe (CLcr 15 – 29 mL/min) renal impairment [see Dosage and Administration (2.7)]. Monitor patients with severe renal impairment for increased adverse reactions and modify the dosage as recommended for adverse reactions [see Dosage and Administration (2.5)].
No dose adjustment is recommended for patients with mild renal impairment (CLcr 60 – 89 mL/min). TALZENNA has not been studied in patients requiring hemodialysis.
12.2 Pharmacodynamics
The exposure-response relationship and time course of pharmacodynamic response for the safety and effectiveness of TALZENNA have not been fully characterized.
Cardiac Electrophysiology
At a dose of 1 mg (the recommended dosage for treatment of breast cancer), TALZENNA had no large QTc prolongation (i.e., >20 ms).
12.3 Pharmacokinetics
After administration of TALZENNA 1 mg orally once daily as a single agent (the recommended dosage for breast cancer), the mean [% coefficient of variation (CV%)] AUC and maximum observed plasma concentration (Cmax) of talazoparib at steady-state was 208 (37%) ng.hr/mL and 16.4 (32%) ng/mL, respectively. The mean (CV%) steady-state Ctrough was 3.53 (61%) ng/mL.
After administration of TALZENNA 0.5 mg orally once daily (the recommended dosage for prostate cancer) with enzalutamide, the mean (CV%) steady-state Ctrough ranged from 3.29 to 3.68 ng/mL (45% to 48%).
The pharmacokinetics (PK) of talazoparib is linear from 0.025 mg to 2 mg (2 times the recommended dose for breast cancer). The median accumulation ratio of talazoparib following 1 mg orally once daily is 2.3 to 5.2. Talazoparib plasma concentrations reached steady-state within 2 to 3 weeks when administered as a single agent and within 9 weeks when coadministered with enzalutamide.
Absorption
The median time to Cmax (Tmax) was generally between 1 to 2 hours after dosing.
Food Effect
Following a single TALZENNA 0.5 mg dose with high-fat, high-calorie food (approximately 800 to 1000 calories with 150, 250, and 500 to 600 calories from protein, carbohydrate, and fat, respectively), the mean Cmax was decreased by 46%, the median Tmax was delayed from 1 to 4 hours, and AUC was not affected.
Distribution
The mean apparent volume of distribution of talazoparib is 420 L. In vitro, protein binding of talazoparib is 74% and is independent of talazoparib concentration.
Elimination
The mean terminal plasma half-life (±standard deviation) is 90 (±58) hours and the mean apparent oral clearance (inter-subject variability) is 6.45 L/h (31%).
Metabolism
Talazoparib undergoes minimal hepatic metabolism. The identified metabolic pathways include mono-oxidation, dehydrogenation, cysteine conjugation of mono-desfluoro-talazoparib, and glucuronide conjugation.
Excretion
Excretion of talazoparib in urine was the major route of elimination. Approximately 68.7% (54.6% unchanged) of the total administered radiolabeled dose of talazoparib was recovered in urine, and 19.7% (13.6% unchanged) was recovered in feces.
Specific Populations
Age (18 to 88 years), sex, race (361 White, 41 Asian, 16 Black, 9 Others, and 63 Not Reported), body weight (36 to 162 kg), and mild to severe hepatic impairment had no clinically significant effect on the PK of talazoparib.
Patients with Renal Impairment
Mild (eGFR 60 – 89 mL/min/1.73 m2) renal impairment had no clinically significant effect on talazoparib pharmacokinetics. Talazoparib steady-state total exposure (AUC) increased by 43% in subjects with moderate (eGFR 30 – 59 mL/min/1.73 m2) renal impairment and 163% in patients with severe (eGFR 15 – 29 mL/min/1.73 m2) renal impairment relative to subjects with normal renal function (eGFR ≥ 90 mL/min/1.73 m2). Talazoparib steady-state peak concentration (Cmax) increased by 32% in subjects with moderate renal impairment and 89% in subjects with severe renal impairment, relative to subjects with normal renal function. Similar increases in AUC were observed with talazoparib when given with enzalutamide for patients with moderate and severe renal impairment. The PK of talazoparib has not been studied in patients requiring hemodialysis. There was no evidence of a relationship between the protein binding of talazoparib and renal function.
Drug Interaction Studies
Clinical Studies
Effect of P-gp Inhibitors: Coadministration of a P-gp inhibitor (itraconazole) with a single 0.5 mg dose of TALZENNA increased talazoparib AUC and Cmax by approximately 56% and 40%, respectively. Coadministration with the following other P-gp inhibitors: amiodarone, carvedilol, clarithromycin, itraconazole, and verapamil increased talazoparib exposure by 45%.
Coadministration with other P-gp inhibitors (including azithromycin, atorvastatin, diltiazem, felodipine, fluvoxamine, and quercetin) had no clinically significant effect on talazoparib pharmacokinetics.
Effect of P-gp Inducers: Coadministration of a P-gp inducer (rifampin) with a single 1 mg dose of TALZENNA increased talazoparib Cmax by 37% with no effect on talazoparib AUC.
Effect of Acid-Reducing Agents: Coadministration of acid-reducing agents including proton pump inhibitors (PPI), histamine receptor 2 antagonists (H2RA), or other acid-reducing agents has no effect on the absorption of talazoparib.
Enzalutamide: Coadministration of enzalutamide with TALZENNA increased talazoparib exposure approximately 2-fold.
In Vitro Studies
Transporters: Talazoparib is a substrate of P-gp and BCRP transporters, but not a substrate of OATP1B1, OATP1B3, OCT1, OCT2, OAT1, OAT3, BSEP, MATE1, or MATE2-K.
Talazoparib is not an inhibitor of P-gp, BCRP, OATP1B1, OATP1B3, OCT1, OCT2, OAT1, OAT3, BSEP, MATE1, or MATE2-K.
CYP Enzymes: Talazoparib is not an inhibitor of CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, or CYP3A4/5.
Talazoparib is not an inducer of CYP1A2, CYP2B6, or CYP3A4.
UGT: Talazoparib is not an inhibitor of UGT isoforms (1A1, 1A4, 1A6, 1A9, 2B7, and 2B15).
2.1 Patient Selection
Information on the FDA-approved tests for the detection of genetic mutations is available at http://www.fda.gov/companiondiagnostics.
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
Select patients for the treatment of advanced breast cancer with TALZENNA based on the presence of germline BRCA mutations [see Indications and Usage (1.1), Clinical Studies (14.1)].
HRR Gene-mutated Metastatic Castration-Resistant Prostate Cancer
Select patients for the treatment of HRR gene-mutated mCRPC with TALZENNA based on the presence of alterations in genes directly or indirectly involved in HRR (ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, or RAD51C) [see Indications and Usage (1.2), Clinical Studies (14.2)].
An FDA-approved test for the detection of HRR gene mutations for use with TALZENNA is not currently available.
8.6 Hepatic Impairment
No dosage modification is recommended for patients with hepatic impairment [see Clinical Pharmacology (12.3)].
1 Indications and Usage
12 Clinical Pharmacology
12.1 Mechanism of Action
Talazoparib is an inhibitor of PARP enzymes, including PARP1 and PARP2, which play a role in DNA repair. In vitro studies with cancer cell lines that harbored defects in DNA repair genes, including BRCA1 and BRCA2, have shown that talazoparib-induced cytotoxicity may involve inhibition of PARP enzymatic activity and increased formation of PARP-DNA complexes resulting in DNA damage, decreased cell proliferation, and apoptosis. Talazoparib anti-tumor activity was observed in patient-derived xenograft breast cancer models bearing mutated BRCA1 or mutated BRCA2 or wild type BRCA1 and BRCA2.
13 Nonclinical Toxicology
5.3 Embryo Fetal Toxicity
Based on its mechanism of action and findings from animal data, TALZENNA can cause fetal harm when administered to a pregnant woman. In an animal reproduction study, administration of talazoparib to pregnant rats during the period of organogenesis caused fetal malformations and structural skeletal variations, and embryo-fetal death at exposures that were 0.24 times the area under the concentration-time curve (AUC) in patients receiving the recommended human dose of 1 mg daily. Apprise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment and for 7 months following the last dose of TALZENNA [see Use in Specific Populations (8.1, 8.3), Clinical Pharmacology (12.1)].
Based on findings from genetic toxicity and animal reproduction studies, advise male patients with female partners of reproductive potential or who are pregnant to use effective contraception during treatment and for 4 months following the last dose of TALZENNA [see Use in Specific Populations (8.1, 8.3), Nonclinical Toxicology (13.1)].
5 Warnings and Precautions
-
•Myelodysplastic Syndrome/Acute Myeloid Leukemia (MDS/AML): MDS/AML occurred in patients exposed to TALZENNA, and some cases were fatal. Monitor patients for hematological toxicity and discontinue if MDS/AML is confirmed. (5.1)
-
•Myelosuppression: TALZENNA may affect hematopoiesis and can cause anemia, neutropenia, and/or thrombocytopenia. (5.2)
-
•Embryo-Fetal Toxicity: TALZENNA can cause fetal harm. Advise of the potential risk to the fetus and to use effective contraception. (5.3, 8.1, 8.3)
14.2 Hrr Gene Mutated Mcrpc
The efficacy of TALZENNA with enzalutamide was evaluated in TALAPRO-2 (NCT03395197), a randomized, double-blind, placebo-controlled, multi-cohort trial in which 399 patients with HRR gene-mutated (HRRm) mCRPC were randomized 1:1 to receive enzalutamide 160 mg daily plus either TALZENNA 0.5 mg or placebo daily until unacceptable toxicity or disease progression. Mutation status of HRR genes was determined prospectively using solid tumor tissue or circulating tumor DNA (ctDNA)-based next generation sequencing assays. Patients were required to have a mutation in at least one of 12 genes involved directly or indirectly in the HRR pathway (ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, or RAD51C). All patients received a GnRH analog or had prior bilateral orchiectomy and needed to have progressed on prior androgen deprivation therapy. Prior treatment with a CYP17 inhibitor or docetaxel for metastatic castration-sensitive prostate cancer (mCSPC) was permitted. Randomization was stratified by previous treatment with a CYP17 inhibitor or docetaxel (yes/no).
The median age was 70 years (range: 41 to 90); 100% were male; 68% were White, 21% Asian, 2.8% Black, 0.8% Other, 7% unknown/not reported; 12% were Hispanic/Latino; and baseline ECOG performance status was 0 (62%) or 1 (38%). Thirty-nine percent of patients had bone-only disease; 15% had visceral disease. In the mCSPC setting, 29% percent of patients had received docetaxel and 9% had received a prior CYP17 inhibitor. The most commonly mutated HRR genes (>5%), including co-occurring mutations, were: BRCA2 (34%), ATM (22%), CDK12 (19%), CHEK2 (18%), and BRCA1 (6%).
The major efficacy outcome measure was radiographic progression-free survival (rPFS) evaluated according to RECIST, version 1.1 and Prostate Cancer Working Group (PCWG3) (bone) criteria, assessed by BICR. An additional efficacy outcome measure was OS.
A statistically significant improvement in rPFS and OS were demonstrated in patients randomized to TALZENNA with enzalutamide compared with placebo with enzalutamide. Efficacy results are presented in Table 10, and Figures 3 and 4.
| Abbreviations: BICR=blinded independent central review; CI=confidence interval; CSPC=castration-sensitive prostate cancer; HRR=homologous recombination repair; mCRPC=metastatic castration-resistant prostate cancer; N=number of patients; NR=not reached. | ||
|
TALZENNA with Enzalutamide N=200 |
Placebo with Enzalutamide N=199 |
|
|
Radiographic Progression-free Survival (rPFS) by BICR |
||
|
Number of events, n (%) |
66 (33) |
104 (52) |
|
Median months (95% CI) |
NR (21.9, NR) |
13.8 (11.0, 16.7) |
|
Hazard ratio (95% CI) Hazard ratio and CI are based on Cox PH model stratified by previous treatment for CSPC.
|
0.45 (0.33, 0.61) |
|
|
p-value p-value (2-sided) is based on log-rank test stratified by previous treatment for CSPC.
|
p<0.0001 |
|
|
|
||
|
Overall Survival (OS) |
||
|
Deaths, n (%) |
93 (47) |
126 (63) |
|
Median months (95% CI) |
45.1 (35.4, NR) |
31.1 (27.3, 35.4) |
|
Hazard ratio (95% CI) |
0.62 (0.48, 0.81) |
|
|
p-value |
p=0.0005 |
Figure 3. Kaplan-Meier Curves of rPFS - TALAPRO-2 (HRR Gene-mutated mCRPC)
Abbreviations: HRR=homologous recombination repair; mCRPC=metastatic castration-resistant prostate cancer; rPFS=radiographic progression-free survival.
Figure 4. Kaplan-Meier Curves of OS – TALAPRO-2 (HRR Gene-mutated mCRPC)
Abbreviations: HRR=homologous recombination repair; mCRPC=metastatic castration-resistant prostate cancer; OS=overall survival.
Exploratory subgroup analyses of rPFS and OS for patients with BRCA-mutated (BRCAm) and non-BRCAm HRRm are presented in Table 11.
| Abbreviations: BRCAm=breast cancer susceptibility gene-mutated; CI=confidence interval; CSPC=castration-sensitive prostate cancer; HRRm=homologous recombination repair gene-mutated; NR=not reached; rPFS=radiographic progression-free survival. | ||||
|
BRCAm |
Non-BRCAm HRRm Includes 4 patients who were incorrectly randomized in the HRRm stratum who did not have HRR gene mutations.
|
|||
|
TALZENNA with Enzalutamide N=71 |
Placebo with Enzalutamide N=84 |
TALZENNA with Enzalutamide N=129 |
Placebo with Enzalutamide N=115 |
|
|
rPFS |
||||
|
Number of events, n (%) |
15 (21) |
54 (64) |
51 (40) |
50 (43) |
|
Median months (95% CI) |
NR (NR, NR) |
11.0 (8.3, 11.1) |
24.7 (16.4, NR) |
16.7 (13.8, 27.7) |
|
Hazard ratio (95% CI) |
0.20 (0.11, 0.36) |
0.74 (0.50, 1.09) |
||
|
|
||||
|
Overall Survival (OS) |
||||
|
Deaths, n (%) |
30 (42) |
56 (67) |
63 (49) |
70 (61) |
|
Median months (95% CI) |
NR (35.4, NR) |
28.5 (24.5, 34.4) |
42.4 (34.2, NR) |
32.6 (28.0, 42.2) |
|
Hazard ratio (95% CI) Hazard ratio and CI are based on Cox PH model unstratified by previous treatment for CSPC.
|
0.48 (0.31, 0.75) |
0.71 (0.51, 1.00) |
2 Dosage and Administration
3 Dosage Forms and Strengths
|
Capsule Strength |
Description |
|
0.1 mg |
White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black) |
|
0.25 mg |
Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black) |
|
0.35 mg |
Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black) |
|
0.5 mg |
Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black) |
|
0.75 mg |
Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black) |
|
1 mg |
Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black) |
8 Use in Specific Populations
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in the WARNINGS AND PRECAUTIONS section reflect exposure to single agent TALZENNA in solid tumor clinical studies, including 286 patients enrolled in EMBRACA trial and to TALZENNA 0.5 mg daily with enzalutamide in 511 patients enrolled in the TALAPRO-2 trial that included 197 patients with HRR gene-mutated mCRPC.
2.2 Recommended Dosage for Gbrca
The recommended dosage of TALZENNA is 1 mg taken orally once daily, until disease progression or unacceptable toxicity.
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
-
•MDS/AML: Advise patients to contact their healthcare provider if they experience weakness, feeling tired, fever, weight loss, frequent infections, bruising, bleeding easily, breathlessness, blood in urine or stool, and/or laboratory findings of low blood cell counts, or a need for blood transfusions. This may be a sign of hematological toxicity or a more serious uncommon bone marrow problem called MDS or AML, which have been reported in patients who received PARP inhibitors [see Warnings and Precautions (5.1)].
-
•Myelosuppression: Advise patients that TALZENNA may affect hematopoiesis and can cause anemia, leukopenia/neutropenia, and/or thrombocytopenia [see Warnings and Precautions (5.2)].
-
•Administration Instructions: Advise patients that TALZENNA can be taken once daily with or without food. Instruct patients that if they miss a dose of TALZENNA, they should take their next normal dose at the usual time. Also advise patients to swallow each capsule whole, and that capsules must not be opened or dissolved [see Dosage and Administration (2.4)].
-
•Embryo-Fetal Toxicity: Advise females to inform their healthcare provider if they are pregnant or become pregnant. Inform female patients of the risk to a fetus and potential loss of the pregnancy [see Use in Specific Populations (8.1)]. Advise females of reproductive potential to use effective contraception during treatment with TALZENNA and for 7 months after the last dose. Advise male patients with female partners of reproductive potential or who are pregnant to use effective contraception during treatment and for 4 months after receiving the last dose of TALZENNA [see Warnings and Precautions (5.3), Use in Specific Populations (8.1, 8.3)].
-
•Lactation: Advise patients not to breastfeed while taking TALZENNA and for 1 month after receiving the last dose [see Use in Specific Populations (8.2)].
16 How Supplied/storage and Handling
TALZENNA is supplied in strengths and package configurations as described in Table 12:
|
Package Configuration |
Capsule Strength (mg) |
NDC |
|
|
Bottles of 30 capsules |
0.1 |
NDC 0069-1031-30 |
White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black). |
|
Bottles of 30 capsules |
0.25 |
NDC 0069-0296-30 |
Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black). |
|
Bottles of 30 capsules |
0.35 |
NDC 0069-1235-30 |
Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black). |
|
Bottles of 30 capsules |
0.5 |
NDC 0069-1501-30 |
Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black). |
|
Bottles of 30 capsules |
0.75 |
NDC 0069-1751-30 |
Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black). |
|
Bottles of 30 capsules |
1 |
NDC 0069-1195-30 |
Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black). |
7.1 Effect of Other Drugs On Talzenna
Effect of P-gp Inhibitors
Breast Cancer
Avoid coadministration of TALZENNA with the following P-gp inhibitors: itraconazole, amiodarone, carvedilol, clarithromycin, itraconazole, and verapamil. If coadministration of TALZENNA with these P-gp inhibitors cannot be avoided, reduce the dose of TALZENNA [see Dosage and Administration (2.7)]. When the P-gp inhibitor is discontinued, increase the dose of TALZENNA [see Dosage and Administration (2.7)].
Coadministration of TALZENNA with these P-gp inhibitors increased talazoparib concentrations [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions.
Monitor for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with other P-gp inhibitors [see Dosage and Administration (2.5)].
HRR Gene-mutated mCRPC
The effect of coadministration of P-gp inhibitors on talazoparib exposure when TALZENNA is taken with enzalutamide has not been studied. Monitor patients for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with a P-gp inhibitor [see Dosage and Administration (2.5)].
Effect of Breast Cancer Resistance Protein (BCRP) Inhibitors
Monitor patients for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with a BCRP inhibitor [see Dosage and Administration (2.5)].
Coadministration of TALZENNA with BCRP inhibitors may increase talazoparib exposure [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions.
2.5 Dosage Modifications for Adverse Reactions
To manage adverse reactions, consider interruption of treatment with or without dose reduction based on severity and clinical presentation. Recommended dose reductions are indicated in Table 1 and Table 2. Treatment with TALZENNA should be discontinued if more than 3 dose reductions are required.
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
|
Dose Reductions |
Dose Level |
|
Recommended starting dose |
1 mg once daily |
|
First dose reduction |
0.75 mg once daily |
|
Second dose reduction |
0.5 mg once daily |
|
Third dose reduction |
0.25 mg once daily |
HRR Gene-mutated mCRPC
|
Dose Reductions |
Dose Level |
|
Recommended starting dose |
0.5 mg once daily |
|
First dose reduction |
0.35 mg once daily |
|
Second dose reduction |
0.25 mg once daily |
|
Third dose reduction |
0.1 mg once daily |
Refer to the enzalutamide prescribing information for dose modifications for adverse reactions associated with enzalutamide.
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer and HRR Gene-mutated mCRPC
Monitor complete blood counts monthly and as clinically indicated [see Warnings and Precautions (5.2)].
|
Adverse Reactions |
Withhold TALZENNA |
Resume TALZENNA |
|
Hemoglobin <8 g/dL |
≥9 g/dL |
Resume TALZENNA at a reduced dose |
|
Platelet count <50,000/μL |
≥75,000/μL |
|
|
Neutrophil count <1,000/μL |
≥1500/µL |
|
|
Non-hematologic Grade 3 or Grade 4 |
≤Grade 1 |
Consider resuming TALZENNA at a reduced dose or discontinue |
8.3 Females and Males of Reproductive Potential
TALZENNA can cause fetal harm when administered to pregnant women [see Use in Specific Populations (8.1)].
Pregnancy Testing
Verify pregnancy status in females of reproductive potential prior to initiating TALZENNA treatment.
Contraception
Females
Advise females of reproductive potential to use effective contraception during treatment and for 7 months following the last dose of TALZENNA.
Males
Based on genotoxicity and animal reproduction studies, advise male patients with female partners of reproductive potential and pregnant partners to use effective contraception during treatment with TALZENNA and for 4 months following the last dose [see Use in Specific Populations (8.1), Nonclinical Toxicology (13.1)].
Infertility
Males
Based on animal studies, TALZENNA may impair fertility in males of reproductive potential [see Nonclinical Toxicology (13.1)].
2.3 Recommended Dosage for Hrr Gene Mutated Mcrpc
The recommended dosage of TALZENNA is 0.5 mg taken orally once daily with enzalutamide until disease progression or unacceptable toxicity.
Refer to the enzalutamide prescribing information for recommended enzalutamide dosing information.
Patients receiving TALZENNA and enzalutamide should also receive a gonadotropin-releasing hormone (GnRH) analog concurrently or should have had bilateral orchiectomy.
5.1 Myelodysplastic Syndrome/acute Myeloid Leukemia
Myelodysplastic Syndrome/Acute Myeloid Leukemia (MDS/AML), including cases with a fatal outcome, has been reported in patients who received TALZENNA.
Overall, MDS/AML has been reported in 0.4% (3 out of 788) of solid tumor patients treated with TALZENNA as a single agent in clinical studies. In TALAPRO-2, MDS/AML occurred in 2 out of 511 (0.4%) patients treated with TALZENNA and enzalutamide and in 0 out of 517 (0%) patients treated with placebo and enzalutamide [see Adverse Reactions (6.1)]. The durations of TALZENNA treatment in these 5 patients prior to developing MDS/AML were 0.3, 1, 2, 3, and 5 years. Most of these patients had received previous chemotherapy with platinum agents and/or other DNA damaging agents including radiotherapy.
Do not start TALZENNA until patients have adequately recovered from hematological toxicity caused by previous chemotherapy. Monitor blood counts monthly during treatment with TALZENNA. For prolonged hematological toxicities, interrupt TALZENNA and monitor blood counts weekly until recovery. If counts do not recover within 4 weeks, refer the patient to a hematologist for further investigations including bone marrow analysis and blood sample for cytogenetics. If MDS/AML is confirmed, discontinue TALZENNA.
Principal Display Panel 1 Mg Capsule Bottle Label
Pfizer
NDC 0069-1195-30
Talzenna®
(talazoparib) capsules
1 mg
30 Capsules
Rx only
Principal Display Panel 1 Mg Capsule Bottle Carton
Pfizer
NDC 0069-1195-30
Talzenna®
(talazoparib)
capsules
1 mg
30 Capsules
Rx only
Principal Display Panel 0.1 Mg Capsule Bottle Label
Pfizer
NDC 0069-1031-30
Talzenna®
(talazoparib) capsules
0.1 mg
30 Capsules
Rx only
Principal Display Panel 0.5 Mg Capsule Bottle Label
Pfizer
NDC 0069-1501-30
Talzenna®
(talazoparib) capsules
0.5 mg
30 Capsules
Rx only
2.7 Dosage Modifications for P Glycoprotein Inhibitors
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
Avoid coadministration of TALZENNA with the following P-glycoprotein (P-gp) inhibitors: itraconazole, amiodarone, carvedilol, clarithromycin, itraconazole, and verapamil. If coadministration of TALZENNA with these P-gp inhibitors cannot be avoided, reduce the dose of TALZENNA to 0.75 mg taken orally once daily. When the P-gp inhibitor is discontinued, increase the dose of TALZENNA (after 3 – 5 half-lives of the P-gp inhibitor) to the dose of TALZENNA that was used before starting the P-gp inhibitor [see Drug Interactions (7.1)].
Monitor for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with other P-gp inhibitors [see Dosage and Administration (2.5)].
Principal Display Panel 0.1 Mg Capsule Bottle Carton
Pfizer
NDC 0069-1031-30
Talzenna®
(talazoparib)
capsules
0.1 mg
30 Capsules
Rx only
Principal Display Panel 0.25 Mg Capsule Bottle Label
Pfizer
NDC 0069-0296-30
Talzenna®
(talazoparib) capsules
0.25 mg
30 Capsules
Rx only
Principal Display Panel 0.35 Mg Capsule Bottle Label
Pfizer
NDC 0069-1235-30
Talzenna®
(talazoparib) capsules
0.35 mg
30 Capsules
Rx only
Principal Display Panel 0.5 Mg Capsule Bottle Carton
Pfizer
NDC 0069-1501-30
Talzenna®
(talazoparib)
capsules
0.5 mg
30 Capsules
Rx only
Principal Display Panel 0.75 Mg Capsule Bottle Label
Pfizer
NDC 0069-1751-30
Talzenna®
(talazoparib) capsules
0.75 mg
30 Capsules
Rx only
14.1 Deleterious Or Suspected Deleterious Germline Brca
EMBRACA (NCT01945775) was an open-label study in which patients (N=431) with gBRCAm HER2-negative locally advanced or metastatic breast cancer were randomized 2:1 to receive TALZENNA 1 mg or healthcare provider's choice of chemotherapy (capecitabine, eribulin, gemcitabine, or vinorelbine) until disease progression or unacceptable toxicity. Randomization was stratified by prior lines of chemotherapy for metastatic disease (0 versus 1, 2, or 3), by triple-negative disease status [triple-negative breast cancer (TNBC) versus non-TNBC], and history of central nervous system (CNS) metastasis (yes versus no).
Patients received no more than 3 prior cytotoxic chemotherapy regimens for their metastatic or locally advanced disease. Patients were required to have received treatment with an anthracycline and/or a taxane (unless contraindicated) in the neoadjuvant, adjuvant, and/or metastatic treatment setting. First-line treatment for advanced or metastatic disease with no prior adjuvant chemotherapy was allowed if the investigator determined that 1 of the 4 chemotherapy choices in the control arm would be an appropriate treatment option for the patient. Patients with prior platinum therapy for advanced disease were required to have no evidence of disease progression during platinum therapy. No prior treatment with a PARP inhibitor was permitted. Of the 431 patients randomized in the EMBRACA study, 408 (95%) were centrally confirmed to have a deleterious or suspected deleterious gBRCAm using a clinical trial assay; out of which 354 (82%) were confirmed using the BRACAnalysis CDx®. BRCA mutation status [breast cancer susceptibility gene 1 (BRCA1)-positive or breast cancer susceptibility gene 2 (BRCA2)-positive] was similar across both treatment arms.
The median age of patients treated with TALZENNA was 46 years (range 28 to 84) and 51 years (range 24 to 89) among patients treated with chemotherapy. Among all randomized patients, 1% versus 2% were males, 67% versus 75% were White; 11% versus 11% were Asian, and 4% versus 1% were Black or African American in the TALZENNA and chemotherapy arms, respectively. Almost all patients (98%) in both arms had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Approximately 56% of patients had estrogen receptor-positive and/or progesterone receptor-positive disease; 44% of patients had triple-negative disease, and the proportions were balanced across both treatment arms. Fifteen percent (15%) of patients in the TALZENNA arm and 14% of patients in the chemotherapy arm had a history of CNS metastases. Ninety-one percent (91%) of patients in the TALZENNA arm had received prior taxane therapy, and 85% had received prior anthracycline therapy in any setting. Sixteen percent (16%) of patients in the TALZENNA arm and 21% of patients in the chemotherapy arm had received prior platinum treatment in any setting. The median number of prior cytotoxic regimens for patients with advanced breast cancer was one; 38% received no prior cytotoxic regimens for advanced or metastatic disease, 37% received one, 20% received two, and 5% received three or more prior cytotoxic regimens.
The major efficacy outcome measure was progression-free survival (PFS) evaluated according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, as assessed by blinded independent central review (BICR). A statistically significant improvement in PFS was demonstrated for TALZENNA compared to chemotherapy. A sensitivity analysis of investigator-assessed PFS was consistent with the BICR-assessed PFS results. Consistent PFS results were observed across patient subgroups defined by study stratification factors (prior lines of chemotherapy, TNBC status, and history of CNS metastases). Efficacy data from the EMBRACA study are summarized in Table 9, and the Kaplan-Meier curves for PFS are shown in Figure 1 and final overall survival (OS) in Figure 2.
| Abbreviations: BICR=blinded independent central review; CI=confidence interval; DOR=duration of response; ITT=intent-to-treat; N=number of patients; ORR=objective response rate; OS=overall survival; PFS=progression-free survival. | ||
|
TALZENNA |
Chemotherapy |
|
|
PFS by BICR |
N=287 |
N=144 |
|
Disease progression or deaths, n (%) |
186 (65) |
83 (58) |
|
Median months (95% CI) |
8.6 (7.2, 9.3) |
5.6 (4.2, 6.7) |
|
Hazard ratio (95% CI) Hazard ratio is estimated from a Cox proportional hazards model stratified by prior use of chemotherapy for metastatic disease (0 versus 1, 2, or 3), by triple-negative disease status [triple-negative breast cancer (TNBC) versus non-TNBC], and by history of central nervous system metastasis (yes versus no) and is relative to overall chemotherapy with <1 favoring talazoparib.
|
0.54 (0.41, 0.71) |
|
|
p-value p-values (2-sided) from the log-rank test stratified by number of prior cytotoxic chemotherapy regimens, triple-negative status and history of central nervous system metastasis.
|
p<0.0001 |
|
|
Patients with Measurable Disease by Investigator Conducted in ITT population with measurable disease at baseline.
|
N=219 |
N=114 |
|
ORR, % (95% CI) Response rate based on confirmed responses.
|
50.2 (43.4, 57.0) |
18.4 (11.8, 26.8) |
|
Median Median estimated from Kaplan-Meier probabilities. DOR months (95% CI)
|
6.4 (5.4, 9.5) |
3.9 (3.0, 7.6) |
|
OS |
N=287 |
N=144 |
|
Deaths, n (%) |
216 (75) |
108 (75) |
|
Median months (95% CI) |
19.3 (16.6, 22.5) |
19.5 (17.4, 22.4) |
|
Hazard ratio (95% CI) |
0.85 (0.67, 1.07) |
|
|
p-value |
p=0.1693 |
Figure 1. Kaplan-Meier Curves of PFS – EMBRACA Study
| Abbreviation: PFS=progression-free survival. |
Figure 2. Kaplan-Meier Curves of OS – EMBRACA Study (ITT Population)
| Abbreviations: ITT=intent-to-treat; OS=overall survival. |
Principal Display Panel 0.25 Mg Capsule Bottle Carton
Pfizer
NDC 0069-0296-30
Talzenna®
(talazoparib)
capsules
0.25 mg
30 Capsules
Rx only
Principal Display Panel 0.35 Mg Capsule Bottle Carton
Pfizer
NDC 0069-1235-30
Talzenna®
(talazoparib)
capsules
0.35 mg
30 Capsules
Rx only
Principal Display Panel 0.75 Mg Capsule Bottle Carton
Pfizer
NDC 0069-1751-30
Talzenna®
(talazoparib)
capsules
0.75 mg
30 Capsules
Rx only
2.6 Recommended Dosage in Patients With Renal Impairment
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
The recommended dosage of TALZENNA for patients with moderate renal impairment (CLcr 30 - 59 mL/min) is 0.75 mg taken orally once daily [see Use in Specific Populations (8.7)].
The recommended dosage of TALZENNA for patients with severe renal impairment (CLcr 15 - 29 mL/min) is 0.5 mg taken orally once daily [see Use in Specific Populations (8.7)].
HRR Gene-mutated mCRPC
The recommended dosage of TALZENNA for patients with moderate renal impairment (CLcr 30 - 59 mL/min) is 0.35 mg taken orally once daily with enzalutamide [see Use in Specific Populations (8.7)].
The recommended dosage of TALZENNA for patients with severe renal impairment (CLcr 15 - 29 mL/min) is 0.25 mg taken orally once daily with enzalutamide [see Use in Specific Populations (8.7)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with talazoparib.
Talazoparib was clastogenic in an in vitro chromosomal aberration assay in human peripheral blood lymphocytes and in an in vivo bone marrow micronucleus assay in rats. This clastogenicity is consistent with genomic instability resulting from the primary pharmacology of talazoparib, indicating the potential for genotoxicity in humans. Talazoparib was not mutagenic in a bacterial reverse mutation (Ames) test.
Fertility studies in animals have not been conducted with talazoparib. In repeat-dose toxicity studies up to 3-months duration, talazoparib-related findings in the testis and epididymis at doses ≥0.04 mg/kg/day in rats and ≥0.01 mg/kg/day in dogs included decreased organ weights, luminal cellular debris, reduced sperm, and degeneration/atrophy. These doses in rats and dogs resulted in approximately 1.0 times and 0.2 times, respectively, the exposure (AUC) in humans at the recommended dose of 1 mg daily. Follicular atresia of the ovary was observed in rats at doses ≥1 mg/kg/day talazoparib, approximately 9.5 times the AUC in patients at the recommended dose of 1 mg daily.
1.2 Hrr Gene Mutated Metastatic Castration Resistant Prostate Cancer (mcrpc)
TALZENNA is indicated in combination with enzalutamide for the treatment of adult patients with homologous recombination repair (HRR) gene-mutated metastatic castration-resistant prostate cancer (mCRPC) [see Dosage and Administration (2.3)].
Structured Label Content
Section 42229-5 (42229-5)
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
Section 42230-3 (42230-3)
| This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 6/2025 | |
|
PATIENT INFORMATION
|
|
|
What is the most important information I should know about TALZENNA?
|
|
|
○ weakness ○ weight loss ○ fever ○ frequent infections |
○ blood in urine or stool ○ shortness of breath ○ feeling very tired ○ bruising or bleeding more easily |
|
Your healthcare provider will do blood tests to check your blood cell counts: ○ every month during treatment with TALZENNA. ○ weekly if you have low blood cell counts that last a long time. Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with TALZENNA if you get certain side effects. See “What are the possible side effects of TALZENNA?” below for other side effects of TALZENNA. |
|
|
What is TALZENNA?
It is not known if TALZENNA is safe and effective in children. |
|
|
Before taking TALZENNA, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Taking TALZENNA with certain other medicines can affect how TALZENNA works and may cause side effects. |
|
|
How should I take TALZENNA?
|
|
|
What are the possible side effects of TALZENNA? TALZENNA may cause serious side effects, including: The most common side effects of TALZENNA when taken alone include: |
|
|
|
|
The most common side effects of TALZENNA when taken in combination with enzalutamide include: |
|
|
|
|
TALZENNA may cause fertility problems in males. This may affect your ability to father a child. Talk to your healthcare provider if this is a concern for you. These are not all of the possible side effects of TALZENNA. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
How should I store TALZENNA?
Keep TALZENNA and all medicines out of the reach of children. |
|
|
General information about the safe and effective use of TALZENNA.
|
|
|
What are the ingredients in TALZENNA?
|
Section 44425-7 (44425-7)
Storage
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F). [See USP Controlled Room Temperature].
1.1 Brca (1.1 BRCA)
TALZENNA is indicated as a single agent for the treatment of adult patients with deleterious or suspected deleterious germline breast cancer susceptibility gene (BRCA)-mutated (gBRCAm) human epidermal growth factor receptor 2 (HER2)-negative locally advanced or metastatic breast cancer. Select patients for therapy based on an FDA-approved companion diagnostic for TALZENNA [see Dosage and Administration (2.1)].
8.1 Pregnancy
Risk Summary
Based on findings from animal studies and its mechanism of action [see Clinical Pharmacology (12.1)], TALZENNA can cause embryo-fetal harm when administered to a pregnant woman. There are no available data on TALZENNA use in pregnant women to inform a drug-associated risk. In an animal reproduction study, the administration of talazoparib to pregnant rats during the period of organogenesis caused fetal malformations and structural skeletal variations and embryo-fetal death at maternal exposures that were 0.24 times the AUC in patients receiving the recommended dose of 1 mg daily (see Data). Apprise pregnant women and females of reproductive potential of the potential risk to a fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the general U.S. population, the estimated background risks of major birth defects and miscarriage in clinically recognized pregnancies are 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In an embryo-fetal development toxicity study, pregnant rats received oral doses of 0.015, 0.05, and 0.15 mg/kg/day talazoparib during the period of organogenesis. Talazoparib caused embryo-fetal death at doses ≥0.015 mg/kg/day (approximately 0.24 times the AUC in patients at the recommended dose of 1 mg daily). A dose of 0.015 mg/kg/day caused decreased fetal body weights and an increased incidence of fetal malformations (depressed eye bulge, small eye, split sternebra, and fused cervical vertebral arch) and structural variations including misshapen or incomplete ossification of the sternebra, skull, rib, and vertebra.
8.2 Lactation
Risk Summary
There are no data on the presence of talazoparib in human milk, the effects of the drug on milk production, or the effects of the drug on the breastfed child. Because of the potential for serious adverse reactions in a breastfed child from talazoparib, advise lactating women not to breastfeed during treatment with TALZENNA and for 1 month after the last dose.
11 Description (11 DESCRIPTION)
Talazoparib is an inhibitor of mammalian polyadenosine 5'-diphosphoribose (ADP-ribose) polymerase (PARP) enzymes. The chemical name of talazoparib tosylate is (8S,9R)-5-Fluoro-8-(4-fluorophenyl)-9-(1-methyl-1H-1,2,4-triazol-5-yl)-2,7,8,9-tetrahydro-3H-pyrido[4,3,2-de]phthalazin-3-one 4-methylbenzenesulfonate (1:1). The chemical formula of talazoparib tosylate is C26H22F2N6O4S, and the relative molecular mass is 552.56 Daltons. The chemical structure of talazoparib tosylate is shown below:
Talazoparib tosylate is a white to yellow solid. TALZENNA capsules for oral use are available as:
-
•0.1 mg hard hypromellose (HPMC) capsule that contains 0.145 mg talazoparib tosylate equivalent to 0.1 mg talazoparib free base, or
-
•0.25 mg HPMC capsule that contains 0.363 mg talazoparib tosylate equivalent to 0.25 mg talazoparib free base, or
-
•0.35 mg HPMC capsule that contains 0.509 mg talazoparib tosylate equivalent to 0.35 mg talazoparib free base, or
-
•0.5 mg HPMC capsule that contains 0.727 mg talazoparib tosylate equivalent to 0.5 mg talazoparib free base, or
-
•0.75 mg HPMC capsule that contains 1.09 mg talazoparib tosylate equivalent to 0.75 mg talazoparib free base, or
-
•1 mg HPMC capsule that contains 1.453 mg talazoparib tosylate equivalent to 1 mg talazoparib free base.
Inactive ingredients: silicified microcrystalline cellulose (sMCC). The capsule shells contain hypromellose (HPMC), yellow iron oxide, red iron oxide and titanium dioxide; and the printing ink contains shellac, black iron oxide, potassium hydroxide, ammonium hydroxide, and propylene glycol.
8.4 Pediatric Use
The safety and effectiveness of TALZENNA have not been established in pediatric patients.
8.5 Geriatric Use
In clinical trials of TALZENNA enrolling 494 patients with advanced solid tumors who received TALZENNA 1 mg daily as a single agent, 85 (17%) patients were ≥65 years of age, and this included 19 (4%) patients who were ≥75 years old. There were 5 patients ≥85 years old. In the TALAPRO-2 trial, of 197 patients who received TALZENNA, 77% were ≥65 years of age, while 30% were ≥75 years of age. No overall differences in safety or effectiveness of TALZENNA were observed between these patients and younger patients.
2.4 Administration
Take TALZENNA with or without food.
Swallow TALZENNA capsules whole. Do not open or dissolve.
If a patient vomits or misses a dose of TALZENNA, instruct them to take the next prescribed dose at the usual time.
14 Clinical Studies (14 CLINICAL STUDIES)
4 Contraindications (4 CONTRAINDICATIONS)
None.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are described elsewhere in the labeling:
-
•Myelodysplastic Syndrome/Acute Myeloid Leukemia [see Warnings and Precautions (5.1)]
-
•Myelosuppression [see Warnings and Precautions (5.2)]
7 Drug Interactions (7 DRUG INTERACTIONS)
5.2 Myelosuppression
Myelosuppression consisting of anemia, neutropenia, and/or thrombocytopenia, have been reported in patients treated with TALZENNA [see Adverse Reactions (6.1)].
Grade ≥3 anemia, neutropenia, and thrombocytopenia were reported, respectively, in 39%, 21%, and 15% of patients receiving TALZENNA as a single agent. Discontinuation due to anemia, neutropenia, and thrombocytopenia occurred, respectively, in 0.7%, 0.3%, and 0.3% of patients.
In TALAPRO-2, Grade ≥3 anemia, neutropenia, and thrombocytopenia were reported, respectively, in 48%, 19%, and 9% of patients receiving TALZENNA and enzalutamide. Forty-two percent of patients (216/511) required a red blood cell transfusion, including 25% (127/511) who required more than one transfusion. Discontinuation due to anemia, neutropenia, and thrombocytopenia occurred, respectively, in 8%, 3%, and 0.4% of patients.
Withhold TALZENNA until patients have adequately recovered from hematological toxicity caused by previous therapy. Monitor blood counts monthly during treatment with TALZENNA. If hematological toxicities do not resolve within 28 days, discontinue TALZENNA and refer the patient to a hematologist for further investigations including bone marrow analysis and blood sample for cytogenetics [see Dosage and Administration (2.5)].
8.7 Renal Impairment
Reduce the recommended dosage of TALZENNA in patients with moderate (CLcr 30 – 59 mL/min) and severe (CLcr 15 – 29 mL/min) renal impairment [see Dosage and Administration (2.7)]. Monitor patients with severe renal impairment for increased adverse reactions and modify the dosage as recommended for adverse reactions [see Dosage and Administration (2.5)].
No dose adjustment is recommended for patients with mild renal impairment (CLcr 60 – 89 mL/min). TALZENNA has not been studied in patients requiring hemodialysis.
12.2 Pharmacodynamics
The exposure-response relationship and time course of pharmacodynamic response for the safety and effectiveness of TALZENNA have not been fully characterized.
Cardiac Electrophysiology
At a dose of 1 mg (the recommended dosage for treatment of breast cancer), TALZENNA had no large QTc prolongation (i.e., >20 ms).
12.3 Pharmacokinetics
After administration of TALZENNA 1 mg orally once daily as a single agent (the recommended dosage for breast cancer), the mean [% coefficient of variation (CV%)] AUC and maximum observed plasma concentration (Cmax) of talazoparib at steady-state was 208 (37%) ng.hr/mL and 16.4 (32%) ng/mL, respectively. The mean (CV%) steady-state Ctrough was 3.53 (61%) ng/mL.
After administration of TALZENNA 0.5 mg orally once daily (the recommended dosage for prostate cancer) with enzalutamide, the mean (CV%) steady-state Ctrough ranged from 3.29 to 3.68 ng/mL (45% to 48%).
The pharmacokinetics (PK) of talazoparib is linear from 0.025 mg to 2 mg (2 times the recommended dose for breast cancer). The median accumulation ratio of talazoparib following 1 mg orally once daily is 2.3 to 5.2. Talazoparib plasma concentrations reached steady-state within 2 to 3 weeks when administered as a single agent and within 9 weeks when coadministered with enzalutamide.
Absorption
The median time to Cmax (Tmax) was generally between 1 to 2 hours after dosing.
Food Effect
Following a single TALZENNA 0.5 mg dose with high-fat, high-calorie food (approximately 800 to 1000 calories with 150, 250, and 500 to 600 calories from protein, carbohydrate, and fat, respectively), the mean Cmax was decreased by 46%, the median Tmax was delayed from 1 to 4 hours, and AUC was not affected.
Distribution
The mean apparent volume of distribution of talazoparib is 420 L. In vitro, protein binding of talazoparib is 74% and is independent of talazoparib concentration.
Elimination
The mean terminal plasma half-life (±standard deviation) is 90 (±58) hours and the mean apparent oral clearance (inter-subject variability) is 6.45 L/h (31%).
Metabolism
Talazoparib undergoes minimal hepatic metabolism. The identified metabolic pathways include mono-oxidation, dehydrogenation, cysteine conjugation of mono-desfluoro-talazoparib, and glucuronide conjugation.
Excretion
Excretion of talazoparib in urine was the major route of elimination. Approximately 68.7% (54.6% unchanged) of the total administered radiolabeled dose of talazoparib was recovered in urine, and 19.7% (13.6% unchanged) was recovered in feces.
Specific Populations
Age (18 to 88 years), sex, race (361 White, 41 Asian, 16 Black, 9 Others, and 63 Not Reported), body weight (36 to 162 kg), and mild to severe hepatic impairment had no clinically significant effect on the PK of talazoparib.
Patients with Renal Impairment
Mild (eGFR 60 – 89 mL/min/1.73 m2) renal impairment had no clinically significant effect on talazoparib pharmacokinetics. Talazoparib steady-state total exposure (AUC) increased by 43% in subjects with moderate (eGFR 30 – 59 mL/min/1.73 m2) renal impairment and 163% in patients with severe (eGFR 15 – 29 mL/min/1.73 m2) renal impairment relative to subjects with normal renal function (eGFR ≥ 90 mL/min/1.73 m2). Talazoparib steady-state peak concentration (Cmax) increased by 32% in subjects with moderate renal impairment and 89% in subjects with severe renal impairment, relative to subjects with normal renal function. Similar increases in AUC were observed with talazoparib when given with enzalutamide for patients with moderate and severe renal impairment. The PK of talazoparib has not been studied in patients requiring hemodialysis. There was no evidence of a relationship between the protein binding of talazoparib and renal function.
Drug Interaction Studies
Clinical Studies
Effect of P-gp Inhibitors: Coadministration of a P-gp inhibitor (itraconazole) with a single 0.5 mg dose of TALZENNA increased talazoparib AUC and Cmax by approximately 56% and 40%, respectively. Coadministration with the following other P-gp inhibitors: amiodarone, carvedilol, clarithromycin, itraconazole, and verapamil increased talazoparib exposure by 45%.
Coadministration with other P-gp inhibitors (including azithromycin, atorvastatin, diltiazem, felodipine, fluvoxamine, and quercetin) had no clinically significant effect on talazoparib pharmacokinetics.
Effect of P-gp Inducers: Coadministration of a P-gp inducer (rifampin) with a single 1 mg dose of TALZENNA increased talazoparib Cmax by 37% with no effect on talazoparib AUC.
Effect of Acid-Reducing Agents: Coadministration of acid-reducing agents including proton pump inhibitors (PPI), histamine receptor 2 antagonists (H2RA), or other acid-reducing agents has no effect on the absorption of talazoparib.
Enzalutamide: Coadministration of enzalutamide with TALZENNA increased talazoparib exposure approximately 2-fold.
In Vitro Studies
Transporters: Talazoparib is a substrate of P-gp and BCRP transporters, but not a substrate of OATP1B1, OATP1B3, OCT1, OCT2, OAT1, OAT3, BSEP, MATE1, or MATE2-K.
Talazoparib is not an inhibitor of P-gp, BCRP, OATP1B1, OATP1B3, OCT1, OCT2, OAT1, OAT3, BSEP, MATE1, or MATE2-K.
CYP Enzymes: Talazoparib is not an inhibitor of CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, or CYP3A4/5.
Talazoparib is not an inducer of CYP1A2, CYP2B6, or CYP3A4.
UGT: Talazoparib is not an inhibitor of UGT isoforms (1A1, 1A4, 1A6, 1A9, 2B7, and 2B15).
2.1 Patient Selection
Information on the FDA-approved tests for the detection of genetic mutations is available at http://www.fda.gov/companiondiagnostics.
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
Select patients for the treatment of advanced breast cancer with TALZENNA based on the presence of germline BRCA mutations [see Indications and Usage (1.1), Clinical Studies (14.1)].
HRR Gene-mutated Metastatic Castration-Resistant Prostate Cancer
Select patients for the treatment of HRR gene-mutated mCRPC with TALZENNA based on the presence of alterations in genes directly or indirectly involved in HRR (ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, or RAD51C) [see Indications and Usage (1.2), Clinical Studies (14.2)].
An FDA-approved test for the detection of HRR gene mutations for use with TALZENNA is not currently available.
8.6 Hepatic Impairment
No dosage modification is recommended for patients with hepatic impairment [see Clinical Pharmacology (12.3)].
1 Indications and Usage (1 INDICATIONS AND USAGE)
12 Clinical Pharmacology (12 CLINICAL PHARMACOLOGY)
12.1 Mechanism of Action
Talazoparib is an inhibitor of PARP enzymes, including PARP1 and PARP2, which play a role in DNA repair. In vitro studies with cancer cell lines that harbored defects in DNA repair genes, including BRCA1 and BRCA2, have shown that talazoparib-induced cytotoxicity may involve inhibition of PARP enzymatic activity and increased formation of PARP-DNA complexes resulting in DNA damage, decreased cell proliferation, and apoptosis. Talazoparib anti-tumor activity was observed in patient-derived xenograft breast cancer models bearing mutated BRCA1 or mutated BRCA2 or wild type BRCA1 and BRCA2.
13 Nonclinical Toxicology (13 NONCLINICAL TOXICOLOGY)
5.3 Embryo Fetal Toxicity (5.3 Embryo-Fetal Toxicity)
Based on its mechanism of action and findings from animal data, TALZENNA can cause fetal harm when administered to a pregnant woman. In an animal reproduction study, administration of talazoparib to pregnant rats during the period of organogenesis caused fetal malformations and structural skeletal variations, and embryo-fetal death at exposures that were 0.24 times the area under the concentration-time curve (AUC) in patients receiving the recommended human dose of 1 mg daily. Apprise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment and for 7 months following the last dose of TALZENNA [see Use in Specific Populations (8.1, 8.3), Clinical Pharmacology (12.1)].
Based on findings from genetic toxicity and animal reproduction studies, advise male patients with female partners of reproductive potential or who are pregnant to use effective contraception during treatment and for 4 months following the last dose of TALZENNA [see Use in Specific Populations (8.1, 8.3), Nonclinical Toxicology (13.1)].
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
-
•Myelodysplastic Syndrome/Acute Myeloid Leukemia (MDS/AML): MDS/AML occurred in patients exposed to TALZENNA, and some cases were fatal. Monitor patients for hematological toxicity and discontinue if MDS/AML is confirmed. (5.1)
-
•Myelosuppression: TALZENNA may affect hematopoiesis and can cause anemia, neutropenia, and/or thrombocytopenia. (5.2)
-
•Embryo-Fetal Toxicity: TALZENNA can cause fetal harm. Advise of the potential risk to the fetus and to use effective contraception. (5.3, 8.1, 8.3)
14.2 Hrr Gene Mutated Mcrpc (14.2 HRR Gene-mutated mCRPC)
The efficacy of TALZENNA with enzalutamide was evaluated in TALAPRO-2 (NCT03395197), a randomized, double-blind, placebo-controlled, multi-cohort trial in which 399 patients with HRR gene-mutated (HRRm) mCRPC were randomized 1:1 to receive enzalutamide 160 mg daily plus either TALZENNA 0.5 mg or placebo daily until unacceptable toxicity or disease progression. Mutation status of HRR genes was determined prospectively using solid tumor tissue or circulating tumor DNA (ctDNA)-based next generation sequencing assays. Patients were required to have a mutation in at least one of 12 genes involved directly or indirectly in the HRR pathway (ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, or RAD51C). All patients received a GnRH analog or had prior bilateral orchiectomy and needed to have progressed on prior androgen deprivation therapy. Prior treatment with a CYP17 inhibitor or docetaxel for metastatic castration-sensitive prostate cancer (mCSPC) was permitted. Randomization was stratified by previous treatment with a CYP17 inhibitor or docetaxel (yes/no).
The median age was 70 years (range: 41 to 90); 100% were male; 68% were White, 21% Asian, 2.8% Black, 0.8% Other, 7% unknown/not reported; 12% were Hispanic/Latino; and baseline ECOG performance status was 0 (62%) or 1 (38%). Thirty-nine percent of patients had bone-only disease; 15% had visceral disease. In the mCSPC setting, 29% percent of patients had received docetaxel and 9% had received a prior CYP17 inhibitor. The most commonly mutated HRR genes (>5%), including co-occurring mutations, were: BRCA2 (34%), ATM (22%), CDK12 (19%), CHEK2 (18%), and BRCA1 (6%).
The major efficacy outcome measure was radiographic progression-free survival (rPFS) evaluated according to RECIST, version 1.1 and Prostate Cancer Working Group (PCWG3) (bone) criteria, assessed by BICR. An additional efficacy outcome measure was OS.
A statistically significant improvement in rPFS and OS were demonstrated in patients randomized to TALZENNA with enzalutamide compared with placebo with enzalutamide. Efficacy results are presented in Table 10, and Figures 3 and 4.
| Abbreviations: BICR=blinded independent central review; CI=confidence interval; CSPC=castration-sensitive prostate cancer; HRR=homologous recombination repair; mCRPC=metastatic castration-resistant prostate cancer; N=number of patients; NR=not reached. | ||
|
TALZENNA with Enzalutamide N=200 |
Placebo with Enzalutamide N=199 |
|
|
Radiographic Progression-free Survival (rPFS) by BICR |
||
|
Number of events, n (%) |
66 (33) |
104 (52) |
|
Median months (95% CI) |
NR (21.9, NR) |
13.8 (11.0, 16.7) |
|
Hazard ratio (95% CI) Hazard ratio and CI are based on Cox PH model stratified by previous treatment for CSPC.
|
0.45 (0.33, 0.61) |
|
|
p-value p-value (2-sided) is based on log-rank test stratified by previous treatment for CSPC.
|
p<0.0001 |
|
|
|
||
|
Overall Survival (OS) |
||
|
Deaths, n (%) |
93 (47) |
126 (63) |
|
Median months (95% CI) |
45.1 (35.4, NR) |
31.1 (27.3, 35.4) |
|
Hazard ratio (95% CI) |
0.62 (0.48, 0.81) |
|
|
p-value |
p=0.0005 |
Figure 3. Kaplan-Meier Curves of rPFS - TALAPRO-2 (HRR Gene-mutated mCRPC)
Abbreviations: HRR=homologous recombination repair; mCRPC=metastatic castration-resistant prostate cancer; rPFS=radiographic progression-free survival.
Figure 4. Kaplan-Meier Curves of OS – TALAPRO-2 (HRR Gene-mutated mCRPC)
Abbreviations: HRR=homologous recombination repair; mCRPC=metastatic castration-resistant prostate cancer; OS=overall survival.
Exploratory subgroup analyses of rPFS and OS for patients with BRCA-mutated (BRCAm) and non-BRCAm HRRm are presented in Table 11.
| Abbreviations: BRCAm=breast cancer susceptibility gene-mutated; CI=confidence interval; CSPC=castration-sensitive prostate cancer; HRRm=homologous recombination repair gene-mutated; NR=not reached; rPFS=radiographic progression-free survival. | ||||
|
BRCAm |
Non-BRCAm HRRm Includes 4 patients who were incorrectly randomized in the HRRm stratum who did not have HRR gene mutations.
|
|||
|
TALZENNA with Enzalutamide N=71 |
Placebo with Enzalutamide N=84 |
TALZENNA with Enzalutamide N=129 |
Placebo with Enzalutamide N=115 |
|
|
rPFS |
||||
|
Number of events, n (%) |
15 (21) |
54 (64) |
51 (40) |
50 (43) |
|
Median months (95% CI) |
NR (NR, NR) |
11.0 (8.3, 11.1) |
24.7 (16.4, NR) |
16.7 (13.8, 27.7) |
|
Hazard ratio (95% CI) |
0.20 (0.11, 0.36) |
0.74 (0.50, 1.09) |
||
|
|
||||
|
Overall Survival (OS) |
||||
|
Deaths, n (%) |
30 (42) |
56 (67) |
63 (49) |
70 (61) |
|
Median months (95% CI) |
NR (35.4, NR) |
28.5 (24.5, 34.4) |
42.4 (34.2, NR) |
32.6 (28.0, 42.2) |
|
Hazard ratio (95% CI) Hazard ratio and CI are based on Cox PH model unstratified by previous treatment for CSPC.
|
0.48 (0.31, 0.75) |
0.71 (0.51, 1.00) |
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
|
Capsule Strength |
Description |
|
0.1 mg |
White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black) |
|
0.25 mg |
Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black) |
|
0.35 mg |
Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black) |
|
0.5 mg |
Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black) |
|
0.75 mg |
Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black) |
|
1 mg |
Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black) |
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in the WARNINGS AND PRECAUTIONS section reflect exposure to single agent TALZENNA in solid tumor clinical studies, including 286 patients enrolled in EMBRACA trial and to TALZENNA 0.5 mg daily with enzalutamide in 511 patients enrolled in the TALAPRO-2 trial that included 197 patients with HRR gene-mutated mCRPC.
2.2 Recommended Dosage for Gbrca (2.2 Recommended Dosage for gBRCA)
The recommended dosage of TALZENNA is 1 mg taken orally once daily, until disease progression or unacceptable toxicity.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise the patient to read the FDA-approved patient labeling (Patient Information).
-
•MDS/AML: Advise patients to contact their healthcare provider if they experience weakness, feeling tired, fever, weight loss, frequent infections, bruising, bleeding easily, breathlessness, blood in urine or stool, and/or laboratory findings of low blood cell counts, or a need for blood transfusions. This may be a sign of hematological toxicity or a more serious uncommon bone marrow problem called MDS or AML, which have been reported in patients who received PARP inhibitors [see Warnings and Precautions (5.1)].
-
•Myelosuppression: Advise patients that TALZENNA may affect hematopoiesis and can cause anemia, leukopenia/neutropenia, and/or thrombocytopenia [see Warnings and Precautions (5.2)].
-
•Administration Instructions: Advise patients that TALZENNA can be taken once daily with or without food. Instruct patients that if they miss a dose of TALZENNA, they should take their next normal dose at the usual time. Also advise patients to swallow each capsule whole, and that capsules must not be opened or dissolved [see Dosage and Administration (2.4)].
-
•Embryo-Fetal Toxicity: Advise females to inform their healthcare provider if they are pregnant or become pregnant. Inform female patients of the risk to a fetus and potential loss of the pregnancy [see Use in Specific Populations (8.1)]. Advise females of reproductive potential to use effective contraception during treatment with TALZENNA and for 7 months after the last dose. Advise male patients with female partners of reproductive potential or who are pregnant to use effective contraception during treatment and for 4 months after receiving the last dose of TALZENNA [see Warnings and Precautions (5.3), Use in Specific Populations (8.1, 8.3)].
-
•Lactation: Advise patients not to breastfeed while taking TALZENNA and for 1 month after receiving the last dose [see Use in Specific Populations (8.2)].
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
TALZENNA is supplied in strengths and package configurations as described in Table 12:
|
Package Configuration |
Capsule Strength (mg) |
NDC |
|
|
Bottles of 30 capsules |
0.1 |
NDC 0069-1031-30 |
White cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.1” in black). |
|
Bottles of 30 capsules |
0.25 |
NDC 0069-0296-30 |
Ivory cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.25” in black). |
|
Bottles of 30 capsules |
0.35 |
NDC 0069-1235-30 |
Ivory cap (printed with “Pfizer” in black) and an ivory body (printed with “TLZ 0.35” in black). |
|
Bottles of 30 capsules |
0.5 |
NDC 0069-1501-30 |
Light pink cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.5” in black). |
|
Bottles of 30 capsules |
0.75 |
NDC 0069-1751-30 |
Light orange cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 0.75” in black). |
|
Bottles of 30 capsules |
1 |
NDC 0069-1195-30 |
Light red cap (printed with “Pfizer” in black) and a white body (printed with “TLZ 1” in black). |
7.1 Effect of Other Drugs On Talzenna (7.1 Effect of Other Drugs on TALZENNA)
Effect of P-gp Inhibitors
Breast Cancer
Avoid coadministration of TALZENNA with the following P-gp inhibitors: itraconazole, amiodarone, carvedilol, clarithromycin, itraconazole, and verapamil. If coadministration of TALZENNA with these P-gp inhibitors cannot be avoided, reduce the dose of TALZENNA [see Dosage and Administration (2.7)]. When the P-gp inhibitor is discontinued, increase the dose of TALZENNA [see Dosage and Administration (2.7)].
Coadministration of TALZENNA with these P-gp inhibitors increased talazoparib concentrations [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions.
Monitor for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with other P-gp inhibitors [see Dosage and Administration (2.5)].
HRR Gene-mutated mCRPC
The effect of coadministration of P-gp inhibitors on talazoparib exposure when TALZENNA is taken with enzalutamide has not been studied. Monitor patients for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with a P-gp inhibitor [see Dosage and Administration (2.5)].
Effect of Breast Cancer Resistance Protein (BCRP) Inhibitors
Monitor patients for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with a BCRP inhibitor [see Dosage and Administration (2.5)].
Coadministration of TALZENNA with BCRP inhibitors may increase talazoparib exposure [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions.
2.5 Dosage Modifications for Adverse Reactions
To manage adverse reactions, consider interruption of treatment with or without dose reduction based on severity and clinical presentation. Recommended dose reductions are indicated in Table 1 and Table 2. Treatment with TALZENNA should be discontinued if more than 3 dose reductions are required.
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
|
Dose Reductions |
Dose Level |
|
Recommended starting dose |
1 mg once daily |
|
First dose reduction |
0.75 mg once daily |
|
Second dose reduction |
0.5 mg once daily |
|
Third dose reduction |
0.25 mg once daily |
HRR Gene-mutated mCRPC
|
Dose Reductions |
Dose Level |
|
Recommended starting dose |
0.5 mg once daily |
|
First dose reduction |
0.35 mg once daily |
|
Second dose reduction |
0.25 mg once daily |
|
Third dose reduction |
0.1 mg once daily |
Refer to the enzalutamide prescribing information for dose modifications for adverse reactions associated with enzalutamide.
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer and HRR Gene-mutated mCRPC
Monitor complete blood counts monthly and as clinically indicated [see Warnings and Precautions (5.2)].
|
Adverse Reactions |
Withhold TALZENNA |
Resume TALZENNA |
|
Hemoglobin <8 g/dL |
≥9 g/dL |
Resume TALZENNA at a reduced dose |
|
Platelet count <50,000/μL |
≥75,000/μL |
|
|
Neutrophil count <1,000/μL |
≥1500/µL |
|
|
Non-hematologic Grade 3 or Grade 4 |
≤Grade 1 |
Consider resuming TALZENNA at a reduced dose or discontinue |
8.3 Females and Males of Reproductive Potential
TALZENNA can cause fetal harm when administered to pregnant women [see Use in Specific Populations (8.1)].
Pregnancy Testing
Verify pregnancy status in females of reproductive potential prior to initiating TALZENNA treatment.
Contraception
Females
Advise females of reproductive potential to use effective contraception during treatment and for 7 months following the last dose of TALZENNA.
Males
Based on genotoxicity and animal reproduction studies, advise male patients with female partners of reproductive potential and pregnant partners to use effective contraception during treatment with TALZENNA and for 4 months following the last dose [see Use in Specific Populations (8.1), Nonclinical Toxicology (13.1)].
Infertility
Males
Based on animal studies, TALZENNA may impair fertility in males of reproductive potential [see Nonclinical Toxicology (13.1)].
2.3 Recommended Dosage for Hrr Gene Mutated Mcrpc (2.3 Recommended Dosage for HRR Gene-mutated mCRPC)
The recommended dosage of TALZENNA is 0.5 mg taken orally once daily with enzalutamide until disease progression or unacceptable toxicity.
Refer to the enzalutamide prescribing information for recommended enzalutamide dosing information.
Patients receiving TALZENNA and enzalutamide should also receive a gonadotropin-releasing hormone (GnRH) analog concurrently or should have had bilateral orchiectomy.
5.1 Myelodysplastic Syndrome/acute Myeloid Leukemia (5.1 Myelodysplastic Syndrome/Acute Myeloid Leukemia)
Myelodysplastic Syndrome/Acute Myeloid Leukemia (MDS/AML), including cases with a fatal outcome, has been reported in patients who received TALZENNA.
Overall, MDS/AML has been reported in 0.4% (3 out of 788) of solid tumor patients treated with TALZENNA as a single agent in clinical studies. In TALAPRO-2, MDS/AML occurred in 2 out of 511 (0.4%) patients treated with TALZENNA and enzalutamide and in 0 out of 517 (0%) patients treated with placebo and enzalutamide [see Adverse Reactions (6.1)]. The durations of TALZENNA treatment in these 5 patients prior to developing MDS/AML were 0.3, 1, 2, 3, and 5 years. Most of these patients had received previous chemotherapy with platinum agents and/or other DNA damaging agents including radiotherapy.
Do not start TALZENNA until patients have adequately recovered from hematological toxicity caused by previous chemotherapy. Monitor blood counts monthly during treatment with TALZENNA. For prolonged hematological toxicities, interrupt TALZENNA and monitor blood counts weekly until recovery. If counts do not recover within 4 weeks, refer the patient to a hematologist for further investigations including bone marrow analysis and blood sample for cytogenetics. If MDS/AML is confirmed, discontinue TALZENNA.
Principal Display Panel 1 Mg Capsule Bottle Label (PRINCIPAL DISPLAY PANEL - 1 mg Capsule Bottle Label)
Pfizer
NDC 0069-1195-30
Talzenna®
(talazoparib) capsules
1 mg
30 Capsules
Rx only
Principal Display Panel 1 Mg Capsule Bottle Carton (PRINCIPAL DISPLAY PANEL - 1 mg Capsule Bottle Carton)
Pfizer
NDC 0069-1195-30
Talzenna®
(talazoparib)
capsules
1 mg
30 Capsules
Rx only
Principal Display Panel 0.1 Mg Capsule Bottle Label (PRINCIPAL DISPLAY PANEL - 0.1 mg Capsule Bottle Label)
Pfizer
NDC 0069-1031-30
Talzenna®
(talazoparib) capsules
0.1 mg
30 Capsules
Rx only
Principal Display Panel 0.5 Mg Capsule Bottle Label (PRINCIPAL DISPLAY PANEL - 0.5 mg Capsule Bottle Label)
Pfizer
NDC 0069-1501-30
Talzenna®
(talazoparib) capsules
0.5 mg
30 Capsules
Rx only
2.7 Dosage Modifications for P Glycoprotein Inhibitors (2.7 Dosage Modifications for P-glycoprotein Inhibitors)
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
Avoid coadministration of TALZENNA with the following P-glycoprotein (P-gp) inhibitors: itraconazole, amiodarone, carvedilol, clarithromycin, itraconazole, and verapamil. If coadministration of TALZENNA with these P-gp inhibitors cannot be avoided, reduce the dose of TALZENNA to 0.75 mg taken orally once daily. When the P-gp inhibitor is discontinued, increase the dose of TALZENNA (after 3 – 5 half-lives of the P-gp inhibitor) to the dose of TALZENNA that was used before starting the P-gp inhibitor [see Drug Interactions (7.1)].
Monitor for increased adverse reactions and modify the dosage as recommended for adverse reactions when TALZENNA is coadministered with other P-gp inhibitors [see Dosage and Administration (2.5)].
Principal Display Panel 0.1 Mg Capsule Bottle Carton (PRINCIPAL DISPLAY PANEL - 0.1 mg Capsule Bottle Carton)
Pfizer
NDC 0069-1031-30
Talzenna®
(talazoparib)
capsules
0.1 mg
30 Capsules
Rx only
Principal Display Panel 0.25 Mg Capsule Bottle Label (PRINCIPAL DISPLAY PANEL - 0.25 mg Capsule Bottle Label)
Pfizer
NDC 0069-0296-30
Talzenna®
(talazoparib) capsules
0.25 mg
30 Capsules
Rx only
Principal Display Panel 0.35 Mg Capsule Bottle Label (PRINCIPAL DISPLAY PANEL - 0.35 mg Capsule Bottle Label)
Pfizer
NDC 0069-1235-30
Talzenna®
(talazoparib) capsules
0.35 mg
30 Capsules
Rx only
Principal Display Panel 0.5 Mg Capsule Bottle Carton (PRINCIPAL DISPLAY PANEL - 0.5 mg Capsule Bottle Carton)
Pfizer
NDC 0069-1501-30
Talzenna®
(talazoparib)
capsules
0.5 mg
30 Capsules
Rx only
Principal Display Panel 0.75 Mg Capsule Bottle Label (PRINCIPAL DISPLAY PANEL - 0.75 mg Capsule Bottle Label)
Pfizer
NDC 0069-1751-30
Talzenna®
(talazoparib) capsules
0.75 mg
30 Capsules
Rx only
14.1 Deleterious Or Suspected Deleterious Germline Brca (14.1 Deleterious or Suspected Deleterious Germline BRCA)
EMBRACA (NCT01945775) was an open-label study in which patients (N=431) with gBRCAm HER2-negative locally advanced or metastatic breast cancer were randomized 2:1 to receive TALZENNA 1 mg or healthcare provider's choice of chemotherapy (capecitabine, eribulin, gemcitabine, or vinorelbine) until disease progression or unacceptable toxicity. Randomization was stratified by prior lines of chemotherapy for metastatic disease (0 versus 1, 2, or 3), by triple-negative disease status [triple-negative breast cancer (TNBC) versus non-TNBC], and history of central nervous system (CNS) metastasis (yes versus no).
Patients received no more than 3 prior cytotoxic chemotherapy regimens for their metastatic or locally advanced disease. Patients were required to have received treatment with an anthracycline and/or a taxane (unless contraindicated) in the neoadjuvant, adjuvant, and/or metastatic treatment setting. First-line treatment for advanced or metastatic disease with no prior adjuvant chemotherapy was allowed if the investigator determined that 1 of the 4 chemotherapy choices in the control arm would be an appropriate treatment option for the patient. Patients with prior platinum therapy for advanced disease were required to have no evidence of disease progression during platinum therapy. No prior treatment with a PARP inhibitor was permitted. Of the 431 patients randomized in the EMBRACA study, 408 (95%) were centrally confirmed to have a deleterious or suspected deleterious gBRCAm using a clinical trial assay; out of which 354 (82%) were confirmed using the BRACAnalysis CDx®. BRCA mutation status [breast cancer susceptibility gene 1 (BRCA1)-positive or breast cancer susceptibility gene 2 (BRCA2)-positive] was similar across both treatment arms.
The median age of patients treated with TALZENNA was 46 years (range 28 to 84) and 51 years (range 24 to 89) among patients treated with chemotherapy. Among all randomized patients, 1% versus 2% were males, 67% versus 75% were White; 11% versus 11% were Asian, and 4% versus 1% were Black or African American in the TALZENNA and chemotherapy arms, respectively. Almost all patients (98%) in both arms had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Approximately 56% of patients had estrogen receptor-positive and/or progesterone receptor-positive disease; 44% of patients had triple-negative disease, and the proportions were balanced across both treatment arms. Fifteen percent (15%) of patients in the TALZENNA arm and 14% of patients in the chemotherapy arm had a history of CNS metastases. Ninety-one percent (91%) of patients in the TALZENNA arm had received prior taxane therapy, and 85% had received prior anthracycline therapy in any setting. Sixteen percent (16%) of patients in the TALZENNA arm and 21% of patients in the chemotherapy arm had received prior platinum treatment in any setting. The median number of prior cytotoxic regimens for patients with advanced breast cancer was one; 38% received no prior cytotoxic regimens for advanced or metastatic disease, 37% received one, 20% received two, and 5% received three or more prior cytotoxic regimens.
The major efficacy outcome measure was progression-free survival (PFS) evaluated according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, as assessed by blinded independent central review (BICR). A statistically significant improvement in PFS was demonstrated for TALZENNA compared to chemotherapy. A sensitivity analysis of investigator-assessed PFS was consistent with the BICR-assessed PFS results. Consistent PFS results were observed across patient subgroups defined by study stratification factors (prior lines of chemotherapy, TNBC status, and history of CNS metastases). Efficacy data from the EMBRACA study are summarized in Table 9, and the Kaplan-Meier curves for PFS are shown in Figure 1 and final overall survival (OS) in Figure 2.
| Abbreviations: BICR=blinded independent central review; CI=confidence interval; DOR=duration of response; ITT=intent-to-treat; N=number of patients; ORR=objective response rate; OS=overall survival; PFS=progression-free survival. | ||
|
TALZENNA |
Chemotherapy |
|
|
PFS by BICR |
N=287 |
N=144 |
|
Disease progression or deaths, n (%) |
186 (65) |
83 (58) |
|
Median months (95% CI) |
8.6 (7.2, 9.3) |
5.6 (4.2, 6.7) |
|
Hazard ratio (95% CI) Hazard ratio is estimated from a Cox proportional hazards model stratified by prior use of chemotherapy for metastatic disease (0 versus 1, 2, or 3), by triple-negative disease status [triple-negative breast cancer (TNBC) versus non-TNBC], and by history of central nervous system metastasis (yes versus no) and is relative to overall chemotherapy with <1 favoring talazoparib.
|
0.54 (0.41, 0.71) |
|
|
p-value p-values (2-sided) from the log-rank test stratified by number of prior cytotoxic chemotherapy regimens, triple-negative status and history of central nervous system metastasis.
|
p<0.0001 |
|
|
Patients with Measurable Disease by Investigator Conducted in ITT population with measurable disease at baseline.
|
N=219 |
N=114 |
|
ORR, % (95% CI) Response rate based on confirmed responses.
|
50.2 (43.4, 57.0) |
18.4 (11.8, 26.8) |
|
Median Median estimated from Kaplan-Meier probabilities. DOR months (95% CI)
|
6.4 (5.4, 9.5) |
3.9 (3.0, 7.6) |
|
OS |
N=287 |
N=144 |
|
Deaths, n (%) |
216 (75) |
108 (75) |
|
Median months (95% CI) |
19.3 (16.6, 22.5) |
19.5 (17.4, 22.4) |
|
Hazard ratio (95% CI) |
0.85 (0.67, 1.07) |
|
|
p-value |
p=0.1693 |
Figure 1. Kaplan-Meier Curves of PFS – EMBRACA Study
| Abbreviation: PFS=progression-free survival. |
Figure 2. Kaplan-Meier Curves of OS – EMBRACA Study (ITT Population)
| Abbreviations: ITT=intent-to-treat; OS=overall survival. |
Principal Display Panel 0.25 Mg Capsule Bottle Carton (PRINCIPAL DISPLAY PANEL - 0.25 mg Capsule Bottle Carton)
Pfizer
NDC 0069-0296-30
Talzenna®
(talazoparib)
capsules
0.25 mg
30 Capsules
Rx only
Principal Display Panel 0.35 Mg Capsule Bottle Carton (PRINCIPAL DISPLAY PANEL - 0.35 mg Capsule Bottle Carton)
Pfizer
NDC 0069-1235-30
Talzenna®
(talazoparib)
capsules
0.35 mg
30 Capsules
Rx only
Principal Display Panel 0.75 Mg Capsule Bottle Carton (PRINCIPAL DISPLAY PANEL - 0.75 mg Capsule Bottle Carton)
Pfizer
NDC 0069-1751-30
Talzenna®
(talazoparib)
capsules
0.75 mg
30 Capsules
Rx only
2.6 Recommended Dosage in Patients With Renal Impairment (2.6 Recommended Dosage in Patients with Renal Impairment)
gBRCAm HER2-negative Locally Advanced or Metastatic Breast Cancer
The recommended dosage of TALZENNA for patients with moderate renal impairment (CLcr 30 - 59 mL/min) is 0.75 mg taken orally once daily [see Use in Specific Populations (8.7)].
The recommended dosage of TALZENNA for patients with severe renal impairment (CLcr 15 - 29 mL/min) is 0.5 mg taken orally once daily [see Use in Specific Populations (8.7)].
HRR Gene-mutated mCRPC
The recommended dosage of TALZENNA for patients with moderate renal impairment (CLcr 30 - 59 mL/min) is 0.35 mg taken orally once daily with enzalutamide [see Use in Specific Populations (8.7)].
The recommended dosage of TALZENNA for patients with severe renal impairment (CLcr 15 - 29 mL/min) is 0.25 mg taken orally once daily with enzalutamide [see Use in Specific Populations (8.7)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with talazoparib.
Talazoparib was clastogenic in an in vitro chromosomal aberration assay in human peripheral blood lymphocytes and in an in vivo bone marrow micronucleus assay in rats. This clastogenicity is consistent with genomic instability resulting from the primary pharmacology of talazoparib, indicating the potential for genotoxicity in humans. Talazoparib was not mutagenic in a bacterial reverse mutation (Ames) test.
Fertility studies in animals have not been conducted with talazoparib. In repeat-dose toxicity studies up to 3-months duration, talazoparib-related findings in the testis and epididymis at doses ≥0.04 mg/kg/day in rats and ≥0.01 mg/kg/day in dogs included decreased organ weights, luminal cellular debris, reduced sperm, and degeneration/atrophy. These doses in rats and dogs resulted in approximately 1.0 times and 0.2 times, respectively, the exposure (AUC) in humans at the recommended dose of 1 mg daily. Follicular atresia of the ovary was observed in rats at doses ≥1 mg/kg/day talazoparib, approximately 9.5 times the AUC in patients at the recommended dose of 1 mg daily.
1.2 Hrr Gene Mutated Metastatic Castration Resistant Prostate Cancer (mcrpc) (1.2 HRR Gene-mutated Metastatic Castration-Resistant Prostate Cancer (mCRPC))
TALZENNA is indicated in combination with enzalutamide for the treatment of adult patients with homologous recombination repair (HRR) gene-mutated metastatic castration-resistant prostate cancer (mCRPC) [see Dosage and Administration (2.3)].
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:51:25.158460 · Updated: 2026-03-14T22:40:22.461215