Irbesartan And Hydrochlorothiazide Tablets
e6d11cd6-7204-4031-a6c5-8f6a33568ab4
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Irbesartan and hydrochlorothiazide tablets USP are indicated for the treatment of hypertension. Irbesartan and hydrochlorothiazide tablets USP may be used in patients whose blood pressure is not adequately controlled on monotherapy. Irbesartan and hydrochlorothiazide tablets USP may also be used as initial therapy in patients who are likely to need multiple drugs to achieve their blood pressure goals. The choice of irbesartan and hydrochlorothiazide tablets USP as initial therapy for hypertension should be based on an assessment of potential benefits and risks. Patients with stage 2 (moderate or severe) hypertension are at relatively high risk for cardiovascular events (such as strokes, heart attacks, and heart failure), kidney failure, and vision problems, so prompt treatment is clinically relevant. The decision to use a combination as initial therapy should be individualized and may be shaped by considerations such as the baseline blood pressure, the target goal, and the incremental likelihood of achieving goal with a combination compared with monotherapy. Data from Studies V and VI [see Clinical Studies (14.2) ] provide estimates of the probability of reaching a blood pressure goal with irbesartan and hydrochlorothiazide tablets USP compared to irbesartan or HCTZ monotherapy. The relationship between baseline blood pressure and achievement of a SeSBP <140 or <130 mmHg or SeDBP <90 or <80 mmHg in patients treated with irbesartan and hydrochlorothiazide tablets USP compared to patients treated with irbesartan or HCTZ monotherapy are shown in Figures 1a through 2b. Figure 1a: Probability of Achieving SBP <140 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) For all probability curves, patients without blood pressure measurements at Week 7 (Study VI) and Week 8 (Study V) were counted as not reaching goal (intent-to-treat analysis). Figure 1b: Probability of Achieving SBP <130 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) Figure 2a: Probability of Achieving DBP <90 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) Figure 2b: Probability of Achieving DBP <80 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) The above graphs provide a rough approximation of the likelihood of reaching a targeted blood pressure goal (e.g., Week 8 sitting systolic blood pressure ≤140 mmHg) for the treatment groups. The curve of each treatment group in each study was estimated by logistic regression modeling from all available data of that treatment group. The estimated likelihood at the right tail of each curve is less reliable due to small numbers of subjects with high baseline blood pressures. For example, a patient with a blood pressure of 180/105 mmHg has about a 25% likelihood of achieving a goal of <140 mmHg (systolic) and 50% likelihood of achieving <90 mmHg (diastolic) on irbesartan alone (and lower still likelihoods on HCTZ alone). The likelihood of achieving these goals on irbesartan and hydrochlorothiazide tablets USP rises to about 40% (systolic) or 70% (diastolic).
Dosage and Administration
General Considerations Maximum effects within 2 to 4 weeks after dose change. ( 2.1 ) Renal impairment: Not recommended for patients with severe renal impairment (creatinine clearance <30 mL/min). ( 2.1 , 5.7 ) Hypertension Initiate with 150/12.5 mg. Titrate to 300/12.5 mg then 300/25 mg if needed. ( 2.2 ) Replacement therapy: May be substituted for titrated components. ( 2.3 )
Contraindications
Irbesartan and hydrochlorothiazide tablets are contraindicated in patients who are hypersensitive to any component of this product. Because of the hydrochlorothiazide component, this product is contraindicated in patients with anuria or hypersensitivity to other sulfonamide-derived drugs. Do not coadminister aliskiren with irbesartan and hydrochlorothiazide tablets in patients with diabetes [see Drug Interactions (7) ].
Warnings and Precautions
Hypotension: Correct volume-depletion prior to administration. ( 5.2 ) Impaired renal function. ( 5.7 ) Thiazide diuretics may cause an exacerbation or activation of systemic lupus erythematosus. ( 5.4 ) Secondary acute angle-closure glaucoma and/or acute myopia. ( 5.8 )
Adverse Reactions
Most common adverse events (≥5% on irbesartan and hydrochlorothiazide and more often than on placebo) are dizziness, fatigue, and musculoskeletal pain. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Hisun Pharmaceuticals USA, Inc. at 1-855-554-4786 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
NSAIDs and selective COX-2 inhibitors: Can reduce diuretic, natriuretic of diuretic, may lead to increased risk of renal impairment and reduced antihypertensive effect. Monitor renal function periodically. (7) Dual blockade of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7) Antidiabetic drugs: Dosage adjustment of antidiabetic may be required (7) Cholestyramine and colestipol: Reduced absorption of thiazides (7) Lithium: Increases in serum lithium concentrations and lithium toxicity (7) Carbamazepine: Increased risk of hyponatremia. (7)
How Supplied
Irbesartan and hydrochlorothiazide tablets, USP have markings on both sides and are available in the strengths and packages listed in the following table: Tablet Strength (irbesartan and hydrochlorothiazide) Film-Coated Tablet Color/Shape Tablet Markings Package Size NDC Code 150 mg/12.5 mg peach, biconvex, oval-shaped debossed with “HU” on one side and “150/12.5” on the other side Bottles of 30 Bottles of 90 Bottles of 500 42658-141-01 42658-141-04 42658-141-07 300 mg/12.5 mg peach, biconvex, oval-shaped debossed with “HU” on one side and “300/12.5” on the other side Bottles of 30 Bottles of 90 Bottles of 500 42658-142-01 42658-142-04 42658-142-07
Description
When pregnancy is detected, discontinue irbesartan and hydrochlorothiazide as soon as possible. [See Warnings and Precautions (5.1) .] Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. [See Warnings and Precautions (5.1) .]
Medication Information
Warnings and Precautions
Hypotension: Correct volume-depletion prior to administration. ( 5.2 ) Impaired renal function. ( 5.7 ) Thiazide diuretics may cause an exacerbation or activation of systemic lupus erythematosus. ( 5.4 ) Secondary acute angle-closure glaucoma and/or acute myopia. ( 5.8 )
Indications and Usage
Irbesartan and hydrochlorothiazide tablets USP are indicated for the treatment of hypertension. Irbesartan and hydrochlorothiazide tablets USP may be used in patients whose blood pressure is not adequately controlled on monotherapy. Irbesartan and hydrochlorothiazide tablets USP may also be used as initial therapy in patients who are likely to need multiple drugs to achieve their blood pressure goals. The choice of irbesartan and hydrochlorothiazide tablets USP as initial therapy for hypertension should be based on an assessment of potential benefits and risks. Patients with stage 2 (moderate or severe) hypertension are at relatively high risk for cardiovascular events (such as strokes, heart attacks, and heart failure), kidney failure, and vision problems, so prompt treatment is clinically relevant. The decision to use a combination as initial therapy should be individualized and may be shaped by considerations such as the baseline blood pressure, the target goal, and the incremental likelihood of achieving goal with a combination compared with monotherapy. Data from Studies V and VI [see Clinical Studies (14.2) ] provide estimates of the probability of reaching a blood pressure goal with irbesartan and hydrochlorothiazide tablets USP compared to irbesartan or HCTZ monotherapy. The relationship between baseline blood pressure and achievement of a SeSBP <140 or <130 mmHg or SeDBP <90 or <80 mmHg in patients treated with irbesartan and hydrochlorothiazide tablets USP compared to patients treated with irbesartan or HCTZ monotherapy are shown in Figures 1a through 2b. Figure 1a: Probability of Achieving SBP <140 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) For all probability curves, patients without blood pressure measurements at Week 7 (Study VI) and Week 8 (Study V) were counted as not reaching goal (intent-to-treat analysis). Figure 1b: Probability of Achieving SBP <130 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) Figure 2a: Probability of Achieving DBP <90 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) Figure 2b: Probability of Achieving DBP <80 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) The above graphs provide a rough approximation of the likelihood of reaching a targeted blood pressure goal (e.g., Week 8 sitting systolic blood pressure ≤140 mmHg) for the treatment groups. The curve of each treatment group in each study was estimated by logistic regression modeling from all available data of that treatment group. The estimated likelihood at the right tail of each curve is less reliable due to small numbers of subjects with high baseline blood pressures. For example, a patient with a blood pressure of 180/105 mmHg has about a 25% likelihood of achieving a goal of <140 mmHg (systolic) and 50% likelihood of achieving <90 mmHg (diastolic) on irbesartan alone (and lower still likelihoods on HCTZ alone). The likelihood of achieving these goals on irbesartan and hydrochlorothiazide tablets USP rises to about 40% (systolic) or 70% (diastolic).
Dosage and Administration
General Considerations Maximum effects within 2 to 4 weeks after dose change. ( 2.1 ) Renal impairment: Not recommended for patients with severe renal impairment (creatinine clearance <30 mL/min). ( 2.1 , 5.7 ) Hypertension Initiate with 150/12.5 mg. Titrate to 300/12.5 mg then 300/25 mg if needed. ( 2.2 ) Replacement therapy: May be substituted for titrated components. ( 2.3 )
Contraindications
Irbesartan and hydrochlorothiazide tablets are contraindicated in patients who are hypersensitive to any component of this product. Because of the hydrochlorothiazide component, this product is contraindicated in patients with anuria or hypersensitivity to other sulfonamide-derived drugs. Do not coadminister aliskiren with irbesartan and hydrochlorothiazide tablets in patients with diabetes [see Drug Interactions (7) ].
Adverse Reactions
Most common adverse events (≥5% on irbesartan and hydrochlorothiazide and more often than on placebo) are dizziness, fatigue, and musculoskeletal pain. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Hisun Pharmaceuticals USA, Inc. at 1-855-554-4786 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
NSAIDs and selective COX-2 inhibitors: Can reduce diuretic, natriuretic of diuretic, may lead to increased risk of renal impairment and reduced antihypertensive effect. Monitor renal function periodically. (7) Dual blockade of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7) Antidiabetic drugs: Dosage adjustment of antidiabetic may be required (7) Cholestyramine and colestipol: Reduced absorption of thiazides (7) Lithium: Increases in serum lithium concentrations and lithium toxicity (7) Carbamazepine: Increased risk of hyponatremia. (7)
How Supplied
Irbesartan and hydrochlorothiazide tablets, USP have markings on both sides and are available in the strengths and packages listed in the following table: Tablet Strength (irbesartan and hydrochlorothiazide) Film-Coated Tablet Color/Shape Tablet Markings Package Size NDC Code 150 mg/12.5 mg peach, biconvex, oval-shaped debossed with “HU” on one side and “150/12.5” on the other side Bottles of 30 Bottles of 90 Bottles of 500 42658-141-01 42658-141-04 42658-141-07 300 mg/12.5 mg peach, biconvex, oval-shaped debossed with “HU” on one side and “300/12.5” on the other side Bottles of 30 Bottles of 90 Bottles of 500 42658-142-01 42658-142-04 42658-142-07
Description
When pregnancy is detected, discontinue irbesartan and hydrochlorothiazide as soon as possible. [See Warnings and Precautions (5.1) .] Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. [See Warnings and Precautions (5.1) .]
Section 34077-8
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue irbesartan and hydrochlorothiazide as soon as possible [see Use in Specific Populations (8.1) ].
Thiazides cross the placenta, and use of thiazides during pregnancy is associated with a risk of fetal or neonatal jaundice, thrombocytopenia, and possibly other adverse reactions that have occurred in adults.
Section 42229-5
Hydrochlorothiazide
Hypersensitivity reactions to hydrochlorothiazide may occur in patients with or without a history of allergy or bronchial asthma, but are more likely in patients with such a history.
Section 51945-4
PRINCIPAL DISPLAY PANEL - 150/12.5 mg Tablet Bottle Label
NDC 42658-141-01
Irbesartan and Hydrochlorothiazide Tablets USP
150 mg/12.5 mg
Rx only 30 Tablets
Pregnancy
Tell female patients of childbearing age about the consequences of exposure to irbesartan and hydrochlorothiazide during pregnancy. Discuss treatment options with women planning to become pregnant. Ask patients to report pregnancies to their physician as soon as possible.
7.6 Lithium
Increases in serum lithium concentrations and lithium toxicity have been reported with concomitant use of irbesartan or thiazide diuretics. Monitor lithium levels in patients receiving irbesartan and hydrochlorothiazide and lithium.
16.2 Storage
Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
11 Description
Irbesartan and hydrochlorothiazide tablets USP are a combination of an angiotensin II receptor antagonist (AT 1 subtype), irbesartan, and a thiazide diuretic, hydrochlorothiazide (HCTZ).
Irbesartan is a non-peptide compound, chemically described as a 2-butyl-3-[ p-( o-1 H-tetrazol-5-ylphenyl)benzyl]-1,3-diazaspiro[4.4]non-1-en-4-one. Its molecular formula is C 25H 28N 6O, and its structural formula is:
Irbesartan, USP is a white to off-white crystalline powder with a molecular weight of 428.5. It is a nonpolar compound with a partition coefficient (octanol/water) of 10.1 at pH of 7.4. Irbesartan is slightly soluble in alcohol and methylene chloride and practically insoluble in water.
Hydrochlorothiazide is 6-chloro-3,4-dihydro-2H-1,2,4-benzothiadiazine-7-sulfonamide1,1 dioxide. Its molecular formula is C7H8ClN3O4S2 and its structural formula is:
Hydrochlorothiazide, USP is a white, or practically white, crystalline powder with a molecular weight of 297.7. Hydrochlorothiazide is slightly soluble in water and freely soluble in sodium hydroxide solution.
Irbesartan and hydrochlorothiazide tablets, USP are available for oral administration in film-coated tablets containing either 150 mg or 300 mg of irbesartan, USP combined with 12.5 mg of hydrochlorothiazide, USP. All dosage strengths contain the following inactive ingredients: lactose monohydrate, microcrystalline cellulose, croscarmellose sodium, hypromellose, magnesium stearate, colloidal silicon dioxide, ferric oxide red, ferric oxide yellow, polyethylene glycol, titanium dioxide.
16.1 How Supplied
Irbesartan and hydrochlorothiazide tablets, USP have markings on both sides and are available in the strengths and packages listed in the following table:
| Tablet Strength
(irbesartan and hydrochlorothiazide) |
Film-Coated Tablet
Color/Shape |
Tablet
Markings |
Package Size | NDC Code |
|---|---|---|---|---|
| 150 mg/12.5 mg | peach, biconvex, oval-shaped | debossed with “HU” on one side and “150/12.5” on the other side | Bottles of 30
Bottles of 90 Bottles of 500 |
42658-141-01
42658-141-04 42658-141-07 |
| 300 mg/12.5 mg | peach, biconvex, oval-shaped | debossed with “HU” on one side and “300/12.5” on the other side | Bottles of 30
Bottles of 90 Bottles of 500 |
42658-142-01
42658-142-04 42658-142-07 |
7.7 Carbamazepine
Concomitant use of carbamazepine and hydrochlorothiazide has been associated with the risk of symptomatic hyponatremia. Monitor electrolytes during concomitant use.
8.5 Geriatric Use
Of 1694 patients receiving irbesartan and hydrochlorothiazide in controlled clinical studies of hypertension, 264 (15.6%) were 65 years and over, while 45 (2.7%) were 75 years and over. No overall differences in safety or effectiveness were observed between these patients and younger patients, but greater sensitivity of some older individuals cannot be ruled out. [See Clinical Pharmacology (12.3) and Clinical Studies (14) .]
2.2 Add On Therapy
In patients not controlled on monotherapy with irbesartan or hydrochlorothiazide, the recommended doses of irbesartan and hydrochlorothiazide tablets, in order of increasing mean effect, are (irbesartan-hydrochlorothiazide) 150/12.5 mg, 300/12.5 mg, and 300/25 mg. The largest incremental effect will likely be in the transition from monotherapy to 150/12.5 mg. [See Clinical Studies (14.2) .]
2.4 Initial Therapy
The usual starting dose is irbesartan and hydrochlorothiazide tablets 150/12.5 mg once daily. The dosage can be increased after 1 to 2 weeks of therapy to a maximum of 300/25 mg once daily as needed to control blood pressure [see Clinical Studies (14.2) ]. Irbesartan and hydrochlorothiazide tablets are not recommended as initial therapy in patients with intravascular volume depletion [see Warnings and Precautions (5.2) ].
4 Contraindications
- Irbesartan and hydrochlorothiazide tablets are contraindicated in patients who are hypersensitive to any component of this product.
- Because of the hydrochlorothiazide component, this product is contraindicated in patients with anuria or hypersensitivity to other sulfonamide-derived drugs.
- Do not coadminister aliskiren with irbesartan and hydrochlorothiazide tablets in patients with diabetes [see Drug Interactions (7) ].
6 Adverse Reactions
Most common adverse events (≥5% on irbesartan and hydrochlorothiazide and more often than on placebo) are dizziness, fatigue, and musculoskeletal pain. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Hisun Pharmaceuticals USA, Inc. at 1-855-554-4786 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions
- NSAIDs and selective COX-2 inhibitors: Can reduce diuretic, natriuretic of diuretic, may lead to increased risk of renal impairment and reduced antihypertensive effect. Monitor renal function periodically. (7)
- Dual blockade of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7)
- Antidiabetic drugs: Dosage adjustment of antidiabetic may be required (7)
- Cholestyramine and colestipol: Reduced absorption of thiazides (7)
- Lithium: Increases in serum lithium concentrations and lithium toxicity (7)
- Carbamazepine: Increased risk of hyponatremia. (7)
8.3 Nursing Mothers
It is not known whether irbesartan is excreted in human milk, but irbesartan or some metabolite of irbesartan is secreted at low concentration in the milk of lactating rats.
Thiazides appear in human milk. Because of the potential for adverse effects on the nursing infant, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Potassium Supplements
Advise patients not to use potassium supplements or salt substitutes containing potassium without consulting their healthcare provider [see Drug Interactions ( 7.3)].
1 Indications and Usage
Irbesartan and hydrochlorothiazide tablets USP are indicated for the treatment of hypertension.
Irbesartan and hydrochlorothiazide tablets USP may be used in patients whose blood pressure is not adequately controlled on monotherapy.
Irbesartan and hydrochlorothiazide tablets USP may also be used as initial therapy in patients who are likely to need multiple drugs to achieve their blood pressure goals.
The choice of irbesartan and hydrochlorothiazide tablets USP as initial therapy for hypertension should be based on an assessment of potential benefits and risks.
Patients with stage 2 (moderate or severe) hypertension are at relatively high risk for cardiovascular events (such as strokes, heart attacks, and heart failure), kidney failure, and vision problems, so prompt treatment is clinically relevant. The decision to use a combination as initial therapy should be individualized and may be shaped by considerations such as the baseline blood pressure, the target goal, and the incremental likelihood of achieving goal with a combination compared with monotherapy.
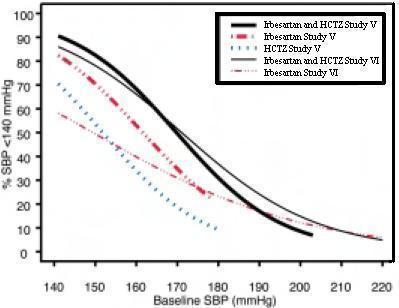
Data from Studies V and VI [see Clinical Studies (14.2) ] provide estimates of the probability of reaching a blood pressure goal with irbesartan and hydrochlorothiazide tablets USP compared to irbesartan or HCTZ monotherapy. The relationship between baseline blood pressure and achievement of a SeSBP <140 or <130 mmHg or SeDBP <90 or <80 mmHg in patients treated with irbesartan and hydrochlorothiazide tablets USP compared to patients treated with irbesartan or HCTZ monotherapy are shown in Figures 1a through 2b.
| Figure 1a: Probability of Achieving SBP <140 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7)
For all probability curves, patients without blood pressure measurements at Week 7 (Study VI) and Week 8 (Study V) were counted as not reaching goal (intent-to-treat analysis).
|
Figure 1b: Probability of Achieving SBP <130 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) |
| Figure 2a: Probability of Achieving DBP <90 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) | Figure 2b: Probability of Achieving DBP <80 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) |
The above graphs provide a rough approximation of the likelihood of reaching a targeted blood pressure goal (e.g., Week 8 sitting systolic blood pressure ≤140 mmHg) for the treatment groups. The curve of each treatment group in each study was estimated by logistic regression modeling from all available data of that treatment group. The estimated likelihood at the right tail of each curve is less reliable due to small numbers of subjects with high baseline blood pressures.
For example, a patient with a blood pressure of 180/105 mmHg has about a 25% likelihood of achieving a goal of <140 mmHg (systolic) and 50% likelihood of achieving <90 mmHg (diastolic) on irbesartan alone (and lower still likelihoods on HCTZ alone).
The likelihood of achieving these goals on irbesartan and hydrochlorothiazide tablets USP rises to about 40% (systolic) or 70% (diastolic).
2.3 Replacement Therapy
Irbesartan and hydrochlorothiazide tablets may be substituted for the titrated components.
Symptomatic Hypotension
Tell patients using irbesartan and hydrochlorothiazide that they may feel lightheaded, especially during the first days of use. Tell patients to inform their physician if they feel lightheaded or faint. Tell the patient, if fainting occurs, stop using irbesartan and hydrochlorothiazide and contact the prescribing doctor.
Tell patients using irbesartan and hydrochlorothiazide that getting dehydrated can lower their blood pressure too much and lead to lightheadedness and possible fainting. Dehydration may occur with excessive sweating, diarrhea, or vomiting and with not drinking enough liquids.
Warning: Fetal Toxicity
- When pregnancy is detected, discontinue irbesartan and hydrochlorothiazide as soon as possible. [See Warnings and Precautions (5.1) .]
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. [See Warnings and Precautions (5.1) .]
2.1 General Considerations
The side effects of irbesartan are generally rare and apparently independent of dose; those of hydrochlorothiazide are a mixture of dose-dependent (primarily hypokalemia) and dose-independent phenomena (e.g., pancreatitis), the former much more common than the latter. [See Adverse Reactions (6) .]
Maximum antihypertensive effects are attained within 2 to 4 weeks after a change in dose.
Irbesartan and hydrochlorothiazide tablets may be administered with or without food.
Irbesartan and hydrochlorothiazide tablets may be administered with other antihypertensive agents.
Renal Impairment. The usual regimens of therapy with irbesartan and hydrochlorothiazide tablets may be followed as long as the patient's creatinine clearance is >30 mL/min. In patients with more severe renal impairment, loop diuretics are preferred to thiazides, so irbesartan and hydrochlorothiazide tablets are not recommended.
Hepatic Impairment. No dosage adjustment is necessary in patients with hepatic impairment.
5 Warnings and Precautions
14.1 Irbesartan Monotherapy
The antihypertensive effects of irbesartan were examined in 7 major placebo-controlled, 8- to 12-week trials in patients with baseline diastolic blood pressures of 95 to 110 mmHg. Doses of 1 to 900 mg were included in these trials in order to fully explore the dose-range of irbesartan. These studies allowed a comparison of once- or twice-daily regimens at 150 mg/day, comparisons of peak and trough effects, and comparisons of response by gender, age, and race. Two of the 7 placebo-controlled trials identified above and 2 additional placebo-controlled studies examined the antihypertensive effects of irbesartan and hydrochlorothiazide in combination.
The 7 studies of irbesartan monotherapy included a total of 1915 patients randomized to irbesartan (1 to 900 mg) and 611 patients randomized to placebo. Once-daily doses of 150 to 300 mg provided statistically and clinically significant decreases in systolic and diastolic blood pressure with trough (24-hour post-dose) effects after 6 to 12 weeks of treatment compared to placebo, of about 8 to 10/5 to 6 mmHg and 8 to 12/5 to 8 mmHg, respectively. No further increase in effect was seen at dosages greater than 300 mg. The dose-response relationships for effects on systolic and diastolic pressure are shown in Figures 3 and 4.
Once-daily administration of therapeutic doses of irbesartan gave peak effects at around 3 to 6 hours and, in one continuous ambulatory blood pressure monitoring study, again around 14 hours. This was seen with both once-daily and twice-daily dosing. Trough-to-peak ratios for systolic and diastolic response were generally between 60% and 70%. In a continuous ambulatory blood pressure monitoring study, once-daily dosing with 150 mg gave trough and mean 24-hour responses similar to those observed in patients receiving twice-daily dosing at the same total daily dose.
Analysis of age, gender, and race subgroups of patients showed that men and women, and patients over and under 65 years of age, had generally similar responses. Irbesartan was effective in reducing blood pressure regardless of race, although the effect was somewhat less in blacks (usually a low-renin population). Black patients typically show an improved response with the addition of a low dose diuretic (e.g., 12.5 mg hydrochlorothiazide).
The effect of irbesartan is apparent after the first dose and is close to the full observed effect at 2 weeks. At the end of the 8-week exposure, about 2/3 of the antihypertensive effect was still present 1 week after the last dose. Rebound hypertension was not observed. There was essentially no change in average heart rate in irbesartan-treated patients in controlled trials.
2 Dosage and Administration
5.7 Impaired Renal Function
As a consequence of inhibiting the renin-angiotensin-aldosterone system, changes in renal function may be anticipated in susceptible individuals [see Drug Interactions (7) ]. In patients whose renal function may depend on the activity of the renin-angiotensin-aldosterone system (e.g., patients with severe congestive heart failure), treatment with ACE inhibitors has been associated with oliguria and/or progressive azotemia and (rarely) with acute renal failure and/or death. Irbesartan would be expected to behave similarly. In studies of ACE inhibitors in patients with unilateral or bilateral renal artery stenosis, increases in serum creatinine or BUN have been reported. There has been no known use of irbesartan in patients with unilateral or bilateral renal artery stenosis, but a similar effect should be anticipated.
Thiazides should be used with caution in severe renal disease. In patients with renal disease, thiazides may precipitate azotemia. Cumulative effects of the drug may develop in patients with impaired renal function.
3 Dosage Forms and Strengths
Irbesartan and hydrochlorothiazide tablets USP, 150 mg/12.5 mg are peach color, oval biconvex, film-coated tablets, debossed with "HU" on one side and “150/12.5” on the other side. Irbesartan and hydrochlorothiazide tablets USP, 300 mg/12.5 mg are peach color, oval biconvex, film-coated tablets, debossed with "HU" on one side and “300/12.5” on the other side.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of irbesartan and hydrochlorothiazide. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Decisions to include these reactions in labeling are typically based on one or more of the following factors: (1) seriousness of the reaction, (2) frequency of reporting, or (3) strength of causal connection to irbesartan and hydrochlorothiazide.
The following have been very rarely reported with irbesartan and hydrochlorothiazide monotherapies: urticaria, jaundice, hepatitis, thrombocytopenia, and impaired renal function including renal failure.
The following have been reported with irbesartan monotherapy: tinnitus, hyperkalemia, angioedema (involving swelling of the face, lips, pharynx, and/or tongue), anaphylactic reaction including anaphylactic shock, and increased CPK.
The following have been reported with hydrochlorothiazide monotherapy: secondary acute angle-closure glaucoma and/or acute myopia.
6.3 Laboratory Abnormalities
In controlled clinical trials, clinically important changes in standard laboratory parameters were rarely associated with administration of irbesartan and hydrochlorothiazide.
Creatinine, Blood Urea Nitrogen: Minor increases in blood urea nitrogen (BUN) or serum creatinine were observed in 2.3% and 1.1%, respectively, of patients with essential hypertension treated with irbesartan and hydrochlorothiazide alone. No patient discontinued taking irbesartan and hydrochlorothiazide due to increased BUN. One patient discontinued taking irbesartan and hydrochlorothiazide due to a minor increase in serum creatinine.
Liver Function Tests: Occasional elevations of liver enzymes and/or serum bilirubin have occurred. In patients with essential hypertension treated with irbesartan and hydrochlorothiazide alone, one patient was discontinued due to elevated liver enzymes.
Serum Electrolytes: [See Warnings and Precautions (5.2, 5.5) .]
8 Use in Specific Populations
- Nursing Mothers: Potential for adverse effects in infant. ( 8.3)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The adverse reaction information from clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
14.2 Irbesartan Hydrochlorothiazide
The antihypertensive effects of irbesartan and hydrochlorothiazide tablets were examined in 4 placebo-controlled studies in patients with mild-moderate hypertension (mean seated diastolic blood pressure [SeDBP] between 90 and 110 mmHg), one study in patients with moderate hypertension (mean seated systolic blood pressure [SeSBP] 160 to 179 mmHg or SeDBP 100 to 109 mmHg), and one study in patients with severe hypertension (mean SeDBP ≥110 mmHg) of 8 to 12 weeks. These trials included 3149 patients randomized to fixed doses of irbesartan (37.5 to 300 mg) and concomitant hydrochlorothiazide (6.25 to 25 mg).
Study I was a factorial study that compared all combinations of irbesartan (37.5 mg, 100 mg, and 300 mg or placebo) and hydrochlorothiazide (6.25 mg, 12.5 mg, and 25 mg or placebo).
Study II compared the irbesartan-hydrochlorothiazide combinations of 75/12.5 mg and 150/12.5 mg to their individual components and placebo.
Study III investigated the ambulatory blood pressure responses to irbesartan-hydrochlorothiazide (75/12.5 mg and 150/12.5 mg) and placebo after 8 weeks of dosing.
Study IV investigated the effects of the addition of irbesartan (75 or 150 mg) in patients not controlled (SeDBP 93–120 mmHg) on hydrochlorothiazide (25 mg) alone. In Studies I–III, the addition of irbesartan 150 to 300 mg to hydrochlorothiazide doses of 6.25, 12.5, or 25 mg produced further dose-related reductions in blood pressure at trough of 8 to 10 mmHg/3 to 6 mmHg, similar to those achieved with the same monotherapy dose of irbesartan. The addition of hydrochlorothiazide to irbesartan produced further dose-related reductions in blood pressure at trough (24 hours post-dose) of 5 to 6/2 to 3 mmHg (12.5 mg) and 7 to 11/4 to 5 mmHg (25 mg), also similar to effects achieved with hydrochlorothiazide alone. Once-daily dosing with 150 mg irbesartan and 12.5 mg hydrochlorothiazide, 300 mg irbesartan and 12.5 mg hydrochlorothiazide, or 300 mg irbesartan and 25 mg hydrochlorothiazide produced mean placebo-adjusted blood pressure reductions at trough (24 hours post-dosing) of about 13 to 15/7 to 9 mmHg, 14/9 to 12 mmHg, and 19 to 21/11 to 12 mmHg, respectively. Peak effects occurred at 3 to 6 hours, with the trough-to-peak ratios >65%.
In Study IV, the addition of irbesartan (75–150 mg) gave an additive effect (systolic/diastolic) at trough (24 hours post-dosing) of 11/7 mmHg.
7.3 Agents Increasing Serum Potassium
Coadministration of irbesartan and hydrochlorothiazide with other drugs that raise serum potassium levels may result in hyperkalemia, sometimes severe. Monitor serum potassium in such patients.
7.5 Cholestyramine and Colestipol Resins
Absorption of hydrochlorothiazide is impaired in the presence of anionic exchange resins. Stagger the dosage of hydrochlorothiazide and the resin such that irbesartan and hydrochlorothiazide is administered at least 4 hours before or 4 to 6 hours after the administration of the resin.
7.4 Antidiabetic Drugs (oral Agents and Insulin)
Dosage adjustment of the antidiabetic drug may be required when coadministered with hydrochlorothiazide.
Acute Myopia and Secondary Angle Closure Glaucoma
Advise patients to discontinue irbesartan and hydrochlorothiazide and seek immediate medical attention if they experience symptoms of Acute Myopia or Secondary Angle-Closure Glaucoma [see Warnings and Precautions ( 5.8)].
5.2 Hypotension in Volume Or Salt Depleted Patients
Excessive reduction of blood pressure was rarely seen in patients with uncomplicated hypertension treated with irbesartan alone (<0.1%) or with irbesartan-hydrochlorothiazide (approximately 1%). Initiation of antihypertensive therapy may cause symptomatic hypotension in patients with intravascular volume- or sodium-depletion, e.g., in patients treated vigorously with diuretics or in patients on dialysis. Such volume depletion should be corrected prior to administration of antihypertensive therapy.
If hypotension occurs, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. A transient hypotensive response is not a contraindication to further treatment, which usually can be continued without difficulty once the blood pressure has stabilized.
7.2 Dual Blockade of the Renin Angiotensin System (ras)
Dual blockade of the RAS with angiotensin-receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Closely monitor blood pressure, renal function, and electrolytes in patients on irbesartan and hydrochlorothiazide and other agents that affect the RAS.
In most patients no benefit has been associated with using two RAS inhibitors concomitantly. In general, avoid combined use of RAS inhibitors.
Do not coadminister aliskiren with irbesartan and hydrochlorothiazide in patients with diabetes. Avoid use of aliskiren with irbesartan and hydrochlorothiazide in patients with renal impairment (GFR <60 mL/min).
5.8 Secondary Acute Angle Closure Glaucoma And/or Acute Myopia
Hydrochlorothiazide
Sulfonamide or sulfonamide derivative drugs, such as hydrochlorothiazide, can cause an idiosyncratic reaction, resulting in transient myopia and/or acute angle-closure glaucoma. Cases of acute angle-closure glaucoma have been reported with hydrochlorothiazide. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue drug intake as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy.
7.1 Non Steroidal Anti Inflammatory Agents Including Selective Cyclooxygenase 2 Inhibitors (cox 2 Inhibitors)
Irbesartan
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, coadministration of NSAIDs, including selective COX-2 inhibitors, with angiotensin II receptor antagonists, including irbesartan, may result in deterioration of renal function, including possible acute renal failure. These effects are usually reversible. Therefore, monitor renal function and blood pressure periodically in patients receiving irbesartan and NSAID therapy.
Hydrochlorothiazide
Administration of a non-steroidal anti-inflammatory agent, including a selective COX-2 inhibitor can reduce the diuretic, natriuretic, and antihypertensive effects of loop, potassium-sparing, and thiazide diuretics. Therefore, when irbesartan and hydrochlorothiazide tablets and non-steroidal anti-inflammatory agents are used concomitantly, the patient should be observed closely to determine if the desired effect of the diuretic is obtained.
Structured Label Content
Section 34077-8 (34077-8)
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue irbesartan and hydrochlorothiazide as soon as possible [see Use in Specific Populations (8.1) ].
Thiazides cross the placenta, and use of thiazides during pregnancy is associated with a risk of fetal or neonatal jaundice, thrombocytopenia, and possibly other adverse reactions that have occurred in adults.
Section 42229-5 (42229-5)
Hydrochlorothiazide
Hypersensitivity reactions to hydrochlorothiazide may occur in patients with or without a history of allergy or bronchial asthma, but are more likely in patients with such a history.
Section 51945-4 (51945-4)
PRINCIPAL DISPLAY PANEL - 150/12.5 mg Tablet Bottle Label
NDC 42658-141-01
Irbesartan and Hydrochlorothiazide Tablets USP
150 mg/12.5 mg
Rx only 30 Tablets
Pregnancy
Tell female patients of childbearing age about the consequences of exposure to irbesartan and hydrochlorothiazide during pregnancy. Discuss treatment options with women planning to become pregnant. Ask patients to report pregnancies to their physician as soon as possible.
7.6 Lithium
Increases in serum lithium concentrations and lithium toxicity have been reported with concomitant use of irbesartan or thiazide diuretics. Monitor lithium levels in patients receiving irbesartan and hydrochlorothiazide and lithium.
16.2 Storage
Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
11 Description (11 DESCRIPTION)
Irbesartan and hydrochlorothiazide tablets USP are a combination of an angiotensin II receptor antagonist (AT 1 subtype), irbesartan, and a thiazide diuretic, hydrochlorothiazide (HCTZ).
Irbesartan is a non-peptide compound, chemically described as a 2-butyl-3-[ p-( o-1 H-tetrazol-5-ylphenyl)benzyl]-1,3-diazaspiro[4.4]non-1-en-4-one. Its molecular formula is C 25H 28N 6O, and its structural formula is:
Irbesartan, USP is a white to off-white crystalline powder with a molecular weight of 428.5. It is a nonpolar compound with a partition coefficient (octanol/water) of 10.1 at pH of 7.4. Irbesartan is slightly soluble in alcohol and methylene chloride and practically insoluble in water.
Hydrochlorothiazide is 6-chloro-3,4-dihydro-2H-1,2,4-benzothiadiazine-7-sulfonamide1,1 dioxide. Its molecular formula is C7H8ClN3O4S2 and its structural formula is:
Hydrochlorothiazide, USP is a white, or practically white, crystalline powder with a molecular weight of 297.7. Hydrochlorothiazide is slightly soluble in water and freely soluble in sodium hydroxide solution.
Irbesartan and hydrochlorothiazide tablets, USP are available for oral administration in film-coated tablets containing either 150 mg or 300 mg of irbesartan, USP combined with 12.5 mg of hydrochlorothiazide, USP. All dosage strengths contain the following inactive ingredients: lactose monohydrate, microcrystalline cellulose, croscarmellose sodium, hypromellose, magnesium stearate, colloidal silicon dioxide, ferric oxide red, ferric oxide yellow, polyethylene glycol, titanium dioxide.
16.1 How Supplied
Irbesartan and hydrochlorothiazide tablets, USP have markings on both sides and are available in the strengths and packages listed in the following table:
| Tablet Strength
(irbesartan and hydrochlorothiazide) |
Film-Coated Tablet
Color/Shape |
Tablet
Markings |
Package Size | NDC Code |
|---|---|---|---|---|
| 150 mg/12.5 mg | peach, biconvex, oval-shaped | debossed with “HU” on one side and “150/12.5” on the other side | Bottles of 30
Bottles of 90 Bottles of 500 |
42658-141-01
42658-141-04 42658-141-07 |
| 300 mg/12.5 mg | peach, biconvex, oval-shaped | debossed with “HU” on one side and “300/12.5” on the other side | Bottles of 30
Bottles of 90 Bottles of 500 |
42658-142-01
42658-142-04 42658-142-07 |
7.7 Carbamazepine
Concomitant use of carbamazepine and hydrochlorothiazide has been associated with the risk of symptomatic hyponatremia. Monitor electrolytes during concomitant use.
8.5 Geriatric Use
Of 1694 patients receiving irbesartan and hydrochlorothiazide in controlled clinical studies of hypertension, 264 (15.6%) were 65 years and over, while 45 (2.7%) were 75 years and over. No overall differences in safety or effectiveness were observed between these patients and younger patients, but greater sensitivity of some older individuals cannot be ruled out. [See Clinical Pharmacology (12.3) and Clinical Studies (14) .]
2.2 Add On Therapy (2.2 Add-On Therapy)
In patients not controlled on monotherapy with irbesartan or hydrochlorothiazide, the recommended doses of irbesartan and hydrochlorothiazide tablets, in order of increasing mean effect, are (irbesartan-hydrochlorothiazide) 150/12.5 mg, 300/12.5 mg, and 300/25 mg. The largest incremental effect will likely be in the transition from monotherapy to 150/12.5 mg. [See Clinical Studies (14.2) .]
2.4 Initial Therapy
The usual starting dose is irbesartan and hydrochlorothiazide tablets 150/12.5 mg once daily. The dosage can be increased after 1 to 2 weeks of therapy to a maximum of 300/25 mg once daily as needed to control blood pressure [see Clinical Studies (14.2) ]. Irbesartan and hydrochlorothiazide tablets are not recommended as initial therapy in patients with intravascular volume depletion [see Warnings and Precautions (5.2) ].
4 Contraindications (4 CONTRAINDICATIONS)
- Irbesartan and hydrochlorothiazide tablets are contraindicated in patients who are hypersensitive to any component of this product.
- Because of the hydrochlorothiazide component, this product is contraindicated in patients with anuria or hypersensitivity to other sulfonamide-derived drugs.
- Do not coadminister aliskiren with irbesartan and hydrochlorothiazide tablets in patients with diabetes [see Drug Interactions (7) ].
6 Adverse Reactions (6 ADVERSE REACTIONS)
Most common adverse events (≥5% on irbesartan and hydrochlorothiazide and more often than on placebo) are dizziness, fatigue, and musculoskeletal pain. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Hisun Pharmaceuticals USA, Inc. at 1-855-554-4786 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions (7 DRUG INTERACTIONS)
- NSAIDs and selective COX-2 inhibitors: Can reduce diuretic, natriuretic of diuretic, may lead to increased risk of renal impairment and reduced antihypertensive effect. Monitor renal function periodically. (7)
- Dual blockade of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7)
- Antidiabetic drugs: Dosage adjustment of antidiabetic may be required (7)
- Cholestyramine and colestipol: Reduced absorption of thiazides (7)
- Lithium: Increases in serum lithium concentrations and lithium toxicity (7)
- Carbamazepine: Increased risk of hyponatremia. (7)
8.3 Nursing Mothers
It is not known whether irbesartan is excreted in human milk, but irbesartan or some metabolite of irbesartan is secreted at low concentration in the milk of lactating rats.
Thiazides appear in human milk. Because of the potential for adverse effects on the nursing infant, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
Potassium Supplements
Advise patients not to use potassium supplements or salt substitutes containing potassium without consulting their healthcare provider [see Drug Interactions ( 7.3)].
1 Indications and Usage (1 INDICATIONS AND USAGE)
Irbesartan and hydrochlorothiazide tablets USP are indicated for the treatment of hypertension.
Irbesartan and hydrochlorothiazide tablets USP may be used in patients whose blood pressure is not adequately controlled on monotherapy.
Irbesartan and hydrochlorothiazide tablets USP may also be used as initial therapy in patients who are likely to need multiple drugs to achieve their blood pressure goals.
The choice of irbesartan and hydrochlorothiazide tablets USP as initial therapy for hypertension should be based on an assessment of potential benefits and risks.
Patients with stage 2 (moderate or severe) hypertension are at relatively high risk for cardiovascular events (such as strokes, heart attacks, and heart failure), kidney failure, and vision problems, so prompt treatment is clinically relevant. The decision to use a combination as initial therapy should be individualized and may be shaped by considerations such as the baseline blood pressure, the target goal, and the incremental likelihood of achieving goal with a combination compared with monotherapy.
Data from Studies V and VI [see Clinical Studies (14.2) ] provide estimates of the probability of reaching a blood pressure goal with irbesartan and hydrochlorothiazide tablets USP compared to irbesartan or HCTZ monotherapy. The relationship between baseline blood pressure and achievement of a SeSBP <140 or <130 mmHg or SeDBP <90 or <80 mmHg in patients treated with irbesartan and hydrochlorothiazide tablets USP compared to patients treated with irbesartan or HCTZ monotherapy are shown in Figures 1a through 2b.
| Figure 1a: Probability of Achieving SBP <140 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7)
For all probability curves, patients without blood pressure measurements at Week 7 (Study VI) and Week 8 (Study V) were counted as not reaching goal (intent-to-treat analysis).
|
Figure 1b: Probability of Achieving SBP <130 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) |
| Figure 2a: Probability of Achieving DBP <90 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) | Figure 2b: Probability of Achieving DBP <80 mmHg in Patients from Initial Therapy Studies V (Week 8) and VI (Week 7) |
The above graphs provide a rough approximation of the likelihood of reaching a targeted blood pressure goal (e.g., Week 8 sitting systolic blood pressure ≤140 mmHg) for the treatment groups. The curve of each treatment group in each study was estimated by logistic regression modeling from all available data of that treatment group. The estimated likelihood at the right tail of each curve is less reliable due to small numbers of subjects with high baseline blood pressures.
For example, a patient with a blood pressure of 180/105 mmHg has about a 25% likelihood of achieving a goal of <140 mmHg (systolic) and 50% likelihood of achieving <90 mmHg (diastolic) on irbesartan alone (and lower still likelihoods on HCTZ alone).
The likelihood of achieving these goals on irbesartan and hydrochlorothiazide tablets USP rises to about 40% (systolic) or 70% (diastolic).
2.3 Replacement Therapy
Irbesartan and hydrochlorothiazide tablets may be substituted for the titrated components.
Symptomatic Hypotension
Tell patients using irbesartan and hydrochlorothiazide that they may feel lightheaded, especially during the first days of use. Tell patients to inform their physician if they feel lightheaded or faint. Tell the patient, if fainting occurs, stop using irbesartan and hydrochlorothiazide and contact the prescribing doctor.
Tell patients using irbesartan and hydrochlorothiazide that getting dehydrated can lower their blood pressure too much and lead to lightheadedness and possible fainting. Dehydration may occur with excessive sweating, diarrhea, or vomiting and with not drinking enough liquids.
Warning: Fetal Toxicity (WARNING: FETAL TOXICITY)
- When pregnancy is detected, discontinue irbesartan and hydrochlorothiazide as soon as possible. [See Warnings and Precautions (5.1) .]
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. [See Warnings and Precautions (5.1) .]
2.1 General Considerations
The side effects of irbesartan are generally rare and apparently independent of dose; those of hydrochlorothiazide are a mixture of dose-dependent (primarily hypokalemia) and dose-independent phenomena (e.g., pancreatitis), the former much more common than the latter. [See Adverse Reactions (6) .]
Maximum antihypertensive effects are attained within 2 to 4 weeks after a change in dose.
Irbesartan and hydrochlorothiazide tablets may be administered with or without food.
Irbesartan and hydrochlorothiazide tablets may be administered with other antihypertensive agents.
Renal Impairment. The usual regimens of therapy with irbesartan and hydrochlorothiazide tablets may be followed as long as the patient's creatinine clearance is >30 mL/min. In patients with more severe renal impairment, loop diuretics are preferred to thiazides, so irbesartan and hydrochlorothiazide tablets are not recommended.
Hepatic Impairment. No dosage adjustment is necessary in patients with hepatic impairment.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
14.1 Irbesartan Monotherapy
The antihypertensive effects of irbesartan were examined in 7 major placebo-controlled, 8- to 12-week trials in patients with baseline diastolic blood pressures of 95 to 110 mmHg. Doses of 1 to 900 mg were included in these trials in order to fully explore the dose-range of irbesartan. These studies allowed a comparison of once- or twice-daily regimens at 150 mg/day, comparisons of peak and trough effects, and comparisons of response by gender, age, and race. Two of the 7 placebo-controlled trials identified above and 2 additional placebo-controlled studies examined the antihypertensive effects of irbesartan and hydrochlorothiazide in combination.
The 7 studies of irbesartan monotherapy included a total of 1915 patients randomized to irbesartan (1 to 900 mg) and 611 patients randomized to placebo. Once-daily doses of 150 to 300 mg provided statistically and clinically significant decreases in systolic and diastolic blood pressure with trough (24-hour post-dose) effects after 6 to 12 weeks of treatment compared to placebo, of about 8 to 10/5 to 6 mmHg and 8 to 12/5 to 8 mmHg, respectively. No further increase in effect was seen at dosages greater than 300 mg. The dose-response relationships for effects on systolic and diastolic pressure are shown in Figures 3 and 4.
Once-daily administration of therapeutic doses of irbesartan gave peak effects at around 3 to 6 hours and, in one continuous ambulatory blood pressure monitoring study, again around 14 hours. This was seen with both once-daily and twice-daily dosing. Trough-to-peak ratios for systolic and diastolic response were generally between 60% and 70%. In a continuous ambulatory blood pressure monitoring study, once-daily dosing with 150 mg gave trough and mean 24-hour responses similar to those observed in patients receiving twice-daily dosing at the same total daily dose.
Analysis of age, gender, and race subgroups of patients showed that men and women, and patients over and under 65 years of age, had generally similar responses. Irbesartan was effective in reducing blood pressure regardless of race, although the effect was somewhat less in blacks (usually a low-renin population). Black patients typically show an improved response with the addition of a low dose diuretic (e.g., 12.5 mg hydrochlorothiazide).
The effect of irbesartan is apparent after the first dose and is close to the full observed effect at 2 weeks. At the end of the 8-week exposure, about 2/3 of the antihypertensive effect was still present 1 week after the last dose. Rebound hypertension was not observed. There was essentially no change in average heart rate in irbesartan-treated patients in controlled trials.
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
5.7 Impaired Renal Function
As a consequence of inhibiting the renin-angiotensin-aldosterone system, changes in renal function may be anticipated in susceptible individuals [see Drug Interactions (7) ]. In patients whose renal function may depend on the activity of the renin-angiotensin-aldosterone system (e.g., patients with severe congestive heart failure), treatment with ACE inhibitors has been associated with oliguria and/or progressive azotemia and (rarely) with acute renal failure and/or death. Irbesartan would be expected to behave similarly. In studies of ACE inhibitors in patients with unilateral or bilateral renal artery stenosis, increases in serum creatinine or BUN have been reported. There has been no known use of irbesartan in patients with unilateral or bilateral renal artery stenosis, but a similar effect should be anticipated.
Thiazides should be used with caution in severe renal disease. In patients with renal disease, thiazides may precipitate azotemia. Cumulative effects of the drug may develop in patients with impaired renal function.
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Irbesartan and hydrochlorothiazide tablets USP, 150 mg/12.5 mg are peach color, oval biconvex, film-coated tablets, debossed with "HU" on one side and “150/12.5” on the other side. Irbesartan and hydrochlorothiazide tablets USP, 300 mg/12.5 mg are peach color, oval biconvex, film-coated tablets, debossed with "HU" on one side and “300/12.5” on the other side.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of irbesartan and hydrochlorothiazide. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Decisions to include these reactions in labeling are typically based on one or more of the following factors: (1) seriousness of the reaction, (2) frequency of reporting, or (3) strength of causal connection to irbesartan and hydrochlorothiazide.
The following have been very rarely reported with irbesartan and hydrochlorothiazide monotherapies: urticaria, jaundice, hepatitis, thrombocytopenia, and impaired renal function including renal failure.
The following have been reported with irbesartan monotherapy: tinnitus, hyperkalemia, angioedema (involving swelling of the face, lips, pharynx, and/or tongue), anaphylactic reaction including anaphylactic shock, and increased CPK.
The following have been reported with hydrochlorothiazide monotherapy: secondary acute angle-closure glaucoma and/or acute myopia.
6.3 Laboratory Abnormalities
In controlled clinical trials, clinically important changes in standard laboratory parameters were rarely associated with administration of irbesartan and hydrochlorothiazide.
Creatinine, Blood Urea Nitrogen: Minor increases in blood urea nitrogen (BUN) or serum creatinine were observed in 2.3% and 1.1%, respectively, of patients with essential hypertension treated with irbesartan and hydrochlorothiazide alone. No patient discontinued taking irbesartan and hydrochlorothiazide due to increased BUN. One patient discontinued taking irbesartan and hydrochlorothiazide due to a minor increase in serum creatinine.
Liver Function Tests: Occasional elevations of liver enzymes and/or serum bilirubin have occurred. In patients with essential hypertension treated with irbesartan and hydrochlorothiazide alone, one patient was discontinued due to elevated liver enzymes.
Serum Electrolytes: [See Warnings and Precautions (5.2, 5.5) .]
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Nursing Mothers: Potential for adverse effects in infant. ( 8.3)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The adverse reaction information from clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
14.2 Irbesartan Hydrochlorothiazide (14.2 Irbesartan-Hydrochlorothiazide)
The antihypertensive effects of irbesartan and hydrochlorothiazide tablets were examined in 4 placebo-controlled studies in patients with mild-moderate hypertension (mean seated diastolic blood pressure [SeDBP] between 90 and 110 mmHg), one study in patients with moderate hypertension (mean seated systolic blood pressure [SeSBP] 160 to 179 mmHg or SeDBP 100 to 109 mmHg), and one study in patients with severe hypertension (mean SeDBP ≥110 mmHg) of 8 to 12 weeks. These trials included 3149 patients randomized to fixed doses of irbesartan (37.5 to 300 mg) and concomitant hydrochlorothiazide (6.25 to 25 mg).
Study I was a factorial study that compared all combinations of irbesartan (37.5 mg, 100 mg, and 300 mg or placebo) and hydrochlorothiazide (6.25 mg, 12.5 mg, and 25 mg or placebo).
Study II compared the irbesartan-hydrochlorothiazide combinations of 75/12.5 mg and 150/12.5 mg to their individual components and placebo.
Study III investigated the ambulatory blood pressure responses to irbesartan-hydrochlorothiazide (75/12.5 mg and 150/12.5 mg) and placebo after 8 weeks of dosing.
Study IV investigated the effects of the addition of irbesartan (75 or 150 mg) in patients not controlled (SeDBP 93–120 mmHg) on hydrochlorothiazide (25 mg) alone. In Studies I–III, the addition of irbesartan 150 to 300 mg to hydrochlorothiazide doses of 6.25, 12.5, or 25 mg produced further dose-related reductions in blood pressure at trough of 8 to 10 mmHg/3 to 6 mmHg, similar to those achieved with the same monotherapy dose of irbesartan. The addition of hydrochlorothiazide to irbesartan produced further dose-related reductions in blood pressure at trough (24 hours post-dose) of 5 to 6/2 to 3 mmHg (12.5 mg) and 7 to 11/4 to 5 mmHg (25 mg), also similar to effects achieved with hydrochlorothiazide alone. Once-daily dosing with 150 mg irbesartan and 12.5 mg hydrochlorothiazide, 300 mg irbesartan and 12.5 mg hydrochlorothiazide, or 300 mg irbesartan and 25 mg hydrochlorothiazide produced mean placebo-adjusted blood pressure reductions at trough (24 hours post-dosing) of about 13 to 15/7 to 9 mmHg, 14/9 to 12 mmHg, and 19 to 21/11 to 12 mmHg, respectively. Peak effects occurred at 3 to 6 hours, with the trough-to-peak ratios >65%.
In Study IV, the addition of irbesartan (75–150 mg) gave an additive effect (systolic/diastolic) at trough (24 hours post-dosing) of 11/7 mmHg.
7.3 Agents Increasing Serum Potassium
Coadministration of irbesartan and hydrochlorothiazide with other drugs that raise serum potassium levels may result in hyperkalemia, sometimes severe. Monitor serum potassium in such patients.
7.5 Cholestyramine and Colestipol Resins
Absorption of hydrochlorothiazide is impaired in the presence of anionic exchange resins. Stagger the dosage of hydrochlorothiazide and the resin such that irbesartan and hydrochlorothiazide is administered at least 4 hours before or 4 to 6 hours after the administration of the resin.
7.4 Antidiabetic Drugs (oral Agents and Insulin) (7.4 Antidiabetic Drugs (oral agents and insulin))
Dosage adjustment of the antidiabetic drug may be required when coadministered with hydrochlorothiazide.
Acute Myopia and Secondary Angle Closure Glaucoma (Acute Myopia and Secondary Angle-Closure Glaucoma)
Advise patients to discontinue irbesartan and hydrochlorothiazide and seek immediate medical attention if they experience symptoms of Acute Myopia or Secondary Angle-Closure Glaucoma [see Warnings and Precautions ( 5.8)].
5.2 Hypotension in Volume Or Salt Depleted Patients (5.2 Hypotension in Volume- or Salt-Depleted Patients)
Excessive reduction of blood pressure was rarely seen in patients with uncomplicated hypertension treated with irbesartan alone (<0.1%) or with irbesartan-hydrochlorothiazide (approximately 1%). Initiation of antihypertensive therapy may cause symptomatic hypotension in patients with intravascular volume- or sodium-depletion, e.g., in patients treated vigorously with diuretics or in patients on dialysis. Such volume depletion should be corrected prior to administration of antihypertensive therapy.
If hypotension occurs, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. A transient hypotensive response is not a contraindication to further treatment, which usually can be continued without difficulty once the blood pressure has stabilized.
7.2 Dual Blockade of the Renin Angiotensin System (ras) (7.2 Dual Blockade of the Renin-Angiotensin System (RAS))
Dual blockade of the RAS with angiotensin-receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Closely monitor blood pressure, renal function, and electrolytes in patients on irbesartan and hydrochlorothiazide and other agents that affect the RAS.
In most patients no benefit has been associated with using two RAS inhibitors concomitantly. In general, avoid combined use of RAS inhibitors.
Do not coadminister aliskiren with irbesartan and hydrochlorothiazide in patients with diabetes. Avoid use of aliskiren with irbesartan and hydrochlorothiazide in patients with renal impairment (GFR <60 mL/min).
5.8 Secondary Acute Angle Closure Glaucoma And/or Acute Myopia (5.8 Secondary Acute Angle-Closure Glaucoma and/or Acute Myopia)
Hydrochlorothiazide
Sulfonamide or sulfonamide derivative drugs, such as hydrochlorothiazide, can cause an idiosyncratic reaction, resulting in transient myopia and/or acute angle-closure glaucoma. Cases of acute angle-closure glaucoma have been reported with hydrochlorothiazide. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue drug intake as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy.
7.1 Non Steroidal Anti Inflammatory Agents Including Selective Cyclooxygenase 2 Inhibitors (cox 2 Inhibitors) (7.1 Non-Steroidal Anti-Inflammatory Agents Including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors))
Irbesartan
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, coadministration of NSAIDs, including selective COX-2 inhibitors, with angiotensin II receptor antagonists, including irbesartan, may result in deterioration of renal function, including possible acute renal failure. These effects are usually reversible. Therefore, monitor renal function and blood pressure periodically in patients receiving irbesartan and NSAID therapy.
Hydrochlorothiazide
Administration of a non-steroidal anti-inflammatory agent, including a selective COX-2 inhibitor can reduce the diuretic, natriuretic, and antihypertensive effects of loop, potassium-sparing, and thiazide diuretics. Therefore, when irbesartan and hydrochlorothiazide tablets and non-steroidal anti-inflammatory agents are used concomitantly, the patient should be observed closely to determine if the desired effect of the diuretic is obtained.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:45:18.810900 · Updated: 2026-03-14T22:22:13.322156