Gazyva
df12ceb2-5b4b-4ab5-a317-2a36bf2a3cda
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
GAZYVA is a CD20-directed cytolytic antibody indicated: in combination with chlorambucil, for the treatment of patients with previously untreated chronic lymphocytic leukemia (CLL). ( 1.1 , 14 ) in combination with bendamustine followed by GAZYVA monotherapy, for the treatment of patients with follicular lymphoma (FL)who relapsed after, or are refractory to, a rituximab-containing regimen. ( 1.2 , 14 ) in combination with chemotherapy followed by GAZYVA monotherapy in patients achieving at least a partial remission, for the treatment of adult patients with previously untreated stage II bulky, III or IV follicular lymphoma. ( 1.2 , 14 ) for the treatment of adult patients with active lupus nephritis (LN) who are receiving standard therapy ( 1.3 , 14 )
Dosage and Administration
Premedicate for infusion-related reactions and tumor lysis syndrome. ( 2.1 , 5.3 , 5.4 ) Administer only as intravenous infusion. Do not administer as an intravenous push or bolus. ( 2.1 ) The recommended dosage for chronic lymphocytic leukemia is 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2–6. ( 2.2 ) The recommended dosage for follicular lymphoma is 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years. ( 2.3 ) The recommended dosage for active lupus nephritis is 1,000 mg at the initial infusion, on Week 2, 24, 26, and every 6 months thereafter. ( 2.4 )
Contraindications
GAZYVA is contraindicated in patients with known hypersensitivity reactions (e.g., anaphylaxis) to obinutuzumab or to any of the excipients, or serum sickness with prior obinutuzumab use [see Warnings and Precautions (5.4) ].
Warnings and Precautions
Infusion-Related Reactions : Premedicate patients with glucocorticoid, acetaminophen, and anti-histamine. Monitor patients closely during infusions. Interrupt, reduce rate, or discontinue for infusion-related reactions based on severity. ( 2.1 , 5.3 ) Hypersensitivity Reactions Including Serum Sickness : Discontinue GAZYVA permanently. ( 5.4 ) Tumor Lysis Syndrome : In CLL and FL, premedicate with anti-hyperuricemics and adequate hydration, especially for patients with high tumor burden, high circulating lymphocyte count or renal impairment. Correct electrolyte abnormalities, provide supportive care, and monitor renal function and fluid balance. ( 5.5 ) Serious, Including Fatal, Infections : Do not administer GAZYVA to patients with an active infection. Patients with a history of recurring or chronic infections may be at increased risk of infection. ( 5.6 ) Neutropenia : In patients with Grade 3 to 4 neutropenia, monitor laboratory tests until resolution and for infection. Consider dose delays and infection prophylaxis, as appropriate. ( 5.7 ) Thrombocytopenia : Monitor for decreased platelet counts and bleeding. Transfusion may be necessary. ( 5.8 ) Disseminated Intravascular Coagulation : Evaluate cause and monitor for bleeding, thrombosis, and need for supportive care. ( 5.9 ) Immunization : Avoid administration of live virus vaccines during GAZYVA treatment and until B-cell recovery. ( 5.10 ) Embryo-Fetal Toxicity : Can cause fetal harm. Advise females of reproductive potential of the potential risk to a fetus and use effective contraception. ( 5.11 )
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: Hepatitis B virus reactivation [see Warnings and Precautions (5.1) ] Progressive multifocal leukoencephalopathy [see Warnings and Precautions (5.2) ] Infusion-related reactions [see Warnings and Precautions (5.3) ] Hypersensitivity reactions including serum sickness [see Warnings and Precautions (5.4) ] Tumor lysis syndrome [see Warnings and Precautions (5.5) ] Infections [see Warnings and Precautions (5.6) ] Neutropenia [see Warnings and Precautions (5.7) ] Thrombocytopenia [see Warnings and Precautions (5.8) ] Disseminated intravascular coagulation [see Warnings and Precautions (5.9) ]
How Supplied
GAZYVA (obinutuzumab) injection is a clear, colorless to slightly brown, preservative-free solution for intravenous use supplied as 1,000 mg/40 mL (25 mg/mL) in single-dose vials (NDC 50242-070-01).
Storage and Handling
GAZYVA (obinutuzumab) injection is a clear, colorless to slightly brown, preservative-free solution for intravenous use supplied as 1,000 mg/40 mL (25 mg/mL) in single-dose vials (NDC 50242-070-01).
Description
Hepatitis B Virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients receiving CD20-directed cytolytic antibodies, including GAZYVA. Screen all patients for HBV infection before treatment initiation. Monitor HBV-positive patients during and after treatment with GAZYVA. Discontinue GAZYVA and concomitant medications in the event of HBV reactivation [see Warnings and Precautions (5.1) ] . Progressive Multifocal Leukoencephalopathy (PML) including fatal PML, can occur in patients receiving GAZYVA [see Warnings and Precautions (5.2) ] .
Medication Information
Warnings and Precautions
Infusion-Related Reactions : Premedicate patients with glucocorticoid, acetaminophen, and anti-histamine. Monitor patients closely during infusions. Interrupt, reduce rate, or discontinue for infusion-related reactions based on severity. ( 2.1 , 5.3 ) Hypersensitivity Reactions Including Serum Sickness : Discontinue GAZYVA permanently. ( 5.4 ) Tumor Lysis Syndrome : In CLL and FL, premedicate with anti-hyperuricemics and adequate hydration, especially for patients with high tumor burden, high circulating lymphocyte count or renal impairment. Correct electrolyte abnormalities, provide supportive care, and monitor renal function and fluid balance. ( 5.5 ) Serious, Including Fatal, Infections : Do not administer GAZYVA to patients with an active infection. Patients with a history of recurring or chronic infections may be at increased risk of infection. ( 5.6 ) Neutropenia : In patients with Grade 3 to 4 neutropenia, monitor laboratory tests until resolution and for infection. Consider dose delays and infection prophylaxis, as appropriate. ( 5.7 ) Thrombocytopenia : Monitor for decreased platelet counts and bleeding. Transfusion may be necessary. ( 5.8 ) Disseminated Intravascular Coagulation : Evaluate cause and monitor for bleeding, thrombosis, and need for supportive care. ( 5.9 ) Immunization : Avoid administration of live virus vaccines during GAZYVA treatment and until B-cell recovery. ( 5.10 ) Embryo-Fetal Toxicity : Can cause fetal harm. Advise females of reproductive potential of the potential risk to a fetus and use effective contraception. ( 5.11 )
Indications and Usage
GAZYVA is a CD20-directed cytolytic antibody indicated: in combination with chlorambucil, for the treatment of patients with previously untreated chronic lymphocytic leukemia (CLL). ( 1.1 , 14 ) in combination with bendamustine followed by GAZYVA monotherapy, for the treatment of patients with follicular lymphoma (FL)who relapsed after, or are refractory to, a rituximab-containing regimen. ( 1.2 , 14 ) in combination with chemotherapy followed by GAZYVA monotherapy in patients achieving at least a partial remission, for the treatment of adult patients with previously untreated stage II bulky, III or IV follicular lymphoma. ( 1.2 , 14 ) for the treatment of adult patients with active lupus nephritis (LN) who are receiving standard therapy ( 1.3 , 14 )
Dosage and Administration
Premedicate for infusion-related reactions and tumor lysis syndrome. ( 2.1 , 5.3 , 5.4 ) Administer only as intravenous infusion. Do not administer as an intravenous push or bolus. ( 2.1 ) The recommended dosage for chronic lymphocytic leukemia is 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2–6. ( 2.2 ) The recommended dosage for follicular lymphoma is 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years. ( 2.3 ) The recommended dosage for active lupus nephritis is 1,000 mg at the initial infusion, on Week 2, 24, 26, and every 6 months thereafter. ( 2.4 )
Contraindications
GAZYVA is contraindicated in patients with known hypersensitivity reactions (e.g., anaphylaxis) to obinutuzumab or to any of the excipients, or serum sickness with prior obinutuzumab use [see Warnings and Precautions (5.4) ].
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: Hepatitis B virus reactivation [see Warnings and Precautions (5.1) ] Progressive multifocal leukoencephalopathy [see Warnings and Precautions (5.2) ] Infusion-related reactions [see Warnings and Precautions (5.3) ] Hypersensitivity reactions including serum sickness [see Warnings and Precautions (5.4) ] Tumor lysis syndrome [see Warnings and Precautions (5.5) ] Infections [see Warnings and Precautions (5.6) ] Neutropenia [see Warnings and Precautions (5.7) ] Thrombocytopenia [see Warnings and Precautions (5.8) ] Disseminated intravascular coagulation [see Warnings and Precautions (5.9) ]
Storage and Handling
GAZYVA (obinutuzumab) injection is a clear, colorless to slightly brown, preservative-free solution for intravenous use supplied as 1,000 mg/40 mL (25 mg/mL) in single-dose vials (NDC 50242-070-01).
How Supplied
GAZYVA (obinutuzumab) injection is a clear, colorless to slightly brown, preservative-free solution for intravenous use supplied as 1,000 mg/40 mL (25 mg/mL) in single-dose vials (NDC 50242-070-01).
Description
Hepatitis B Virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients receiving CD20-directed cytolytic antibodies, including GAZYVA. Screen all patients for HBV infection before treatment initiation. Monitor HBV-positive patients during and after treatment with GAZYVA. Discontinue GAZYVA and concomitant medications in the event of HBV reactivation [see Warnings and Precautions (5.1) ] . Progressive Multifocal Leukoencephalopathy (PML) including fatal PML, can occur in patients receiving GAZYVA [see Warnings and Precautions (5.2) ] .
Section 42229-5
Infusion-Related Reactions
Premedication to reduce the risk of IRRs is outlined in Table 6 [see Warnings and Precautions (5.3)].
Hypotension may occur during GAZYVA intravenous infusions. Consider withholding antihypertensive treatments for 12 hours prior to and throughout each GAZYVA infusion and for the first hour after administration [see Warnings and Precautions (5.3)].
| Indication/Cycle/Day of Treatment | Patients requiring premedication | Premedication | Administration |
|---|---|---|---|
| Premedication applies to both standard and approximately 90-minute infusions. | |||
|
CLL Cycle 1 Days 1 and 2 FL Cycle 1 Day 1 |
All patients | Intravenous glucocorticoid: 20 mg dexamethasone or 80 mg methylprednisolone Hydrocortisone is not recommended as it has not been effective in reducing the rate of IRRs.
,
If a glucocorticoid-containing chemotherapy regimen is administered on the same day as GAZYVA, the glucocorticoid can be administered as an oral medication if given at least 1 hour prior to GAZYVA, in which case additional intravenous glucocorticoid as premedication is not required.
|
Completed at least 1 hour prior to GAZYVA infusion. |
| 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. | ||
| anti-histamine (e.g., 50 mg diphenhydramine) | |||
|
CLL or FL All subsequent infusions |
All patients | 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. |
| Patients with an IRR (Grade 1-2) with the previous infusion | 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. | |
| anti-histamine (e.g., 50 mg diphenhydramine) | |||
| Patients with a Grade 3 IRR with the previous infusion OR with a lymphocyte count > 25 × 109/L prior to next treatment | Intravenous glucocorticoid: 20 mg dexamethasone or 80 mg methylprednisolone |
Completed at least 1 hour prior to GAZYVA infusion. | |
| 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. | ||
| anti-histamine (e.g., 50 mg diphenhydramine) | |||
| LN | All patients | Intravenous glucocorticoid (80 mg methylprednisolone) | Completed between 30 and 60 minutes prior to GAZYVA infusion Starting from Dose 6, intravenous corticosteroid should only be administered to patients who have experienced an IRR in the prior infusion |
| 650–1,000 mg acetaminophen | |||
| anti-histamine (e.g., 50 mg diphenhydramine) |
Section 43683-2
Section 44425-7
Store at 2°C to 8°C (36°F to 46°F). Do not use beyond expiration date stamped on carton. Protect from light. DO NOT FREEZE. DO NOT SHAKE.
10 Overdosage
There has been no experience with overdose in human clinical trials. For patients who experience overdose, treatment should consist of immediate interruption or reduction of GAZYVA and supportive therapy.
11 Description
Obinutuzumab is a humanized anti-CD20 monoclonal antibody of the IgG1 subclass. It recognizes a specific epitope of the CD20 molecule found on B cells. The molecular mass of the antibody is approximately 150 kDa.
GAZYVA (obinutuzumab) injection is produced by mammalian cell (CHO) suspension culture. GAZYVA was engineered to have reduced fucose content as compared to a typical IgG1 produced in CHO cells. GAZYVA is a sterile, clear, colorless to slightly brown, preservative-free liquid concentrate for intravenous use. GAZYVA is supplied at a concentration of 25 mg/mL in 1,000 mg single-dose vials. Each vial contains in 40 mL: 1,000 mg obinutuzumab, L-histidine (57.6 mg), L-histidine hydrochloride monohydrate (89.6 mg), trehalose dihydrate (3632 mg), and poloxamer 188 (8 mg). The pH is 6.0.
5.7 Neutropenia
Severe and life-threatening neutropenia, including febrile neutropenia, has been reported during treatment with GAZYVA. Monitor patients with Grade 3 to 4 neutropenia frequently with regular laboratory tests until resolution. Anticipate, evaluate, and treat any symptoms or signs of developing infection. Consider dose delays for Grade 3 or 4 neutropenia. Consider administration of granulocyte colony-stimulating factors (GCSF) in patients with Grade 3 or 4 neutropenia.
Neutropenia can also be of late onset (occurring more than 28 days after completion of treatment) and/or prolonged (lasting longer than 28 days). Patients with severe and long lasting (> 1 week) neutropenia are strongly recommended to receive antimicrobial prophylaxis until resolution of neutropenia to Grade 1 or 2. Consider antiviral and antifungal prophylaxis.
5.10 Immunization
The safety and efficacy of immunization with live or attenuated viral vaccines during or following GAZYVA therapy have not been studied. Immunization with live virus vaccines is not recommended during treatment with GAZYVA and until B-cell recovery.
8.4 Pediatric Use
The safety and effectiveness of GAZYVA in pediatric patients have not been established.
12.6 Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of anti-drug antibody (ADA) (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies or to other products may be misleading.
Seven percent (18/271) of patients with CLL tested positive for anti-GAZYVA antibodies at one or more time points in CLL11. No patients developed anti-GAZYVA antibodies during or following GAZYVA treatment in GADOLIN, while 1 patient (1/564, 0.2%) developed anti-GAZYVA antibodies in GALLIUM. Neutralizing activity of anti-GAZYVA antibodies was not assessed.
In GAZYVA-treated patients in the LN studies, a total of 12 out of 200 (6%) had at least one ADA-positive sample recorded at any time during the studies. Six (3%) subjects had ADA-positive samples recorded at baseline in which two patients remained ADA-positive throughout the studies, one patient had a single post-baseline sample that was ADA-positive, and three patients had post-baseline samples that were all ADA-negative. Six (3%) patients with ADA-negative samples at baseline had a positive ADA titer post-baseline (treatment-induced ADA). None of the 12 patients with positive ADA titers at any time during the treatment period experienced an IRR or hypersensitivity reaction during the studies. Neutralizing activity of anti-GAZYVA antibodies was not assessed.
Because of the low occurrence of anti-drug antibodies, the effect of these antibodies on the pharmacokinetics, pharmacodynamics, safety and/or effectiveness of GAZYVA is unknown.
4 Contraindications
GAZYVA is contraindicated in patients with known hypersensitivity reactions (e.g., anaphylaxis) to obinutuzumab or to any of the excipients, or serum sickness with prior obinutuzumab use [see Warnings and Precautions (5.4)].
6 Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hepatitis B virus reactivation [see Warnings and Precautions (5.1)]
- Progressive multifocal leukoencephalopathy [see Warnings and Precautions (5.2)]
- Infusion-related reactions [see Warnings and Precautions (5.3)]
- Hypersensitivity reactions including serum sickness [see Warnings and Precautions (5.4)]
- Tumor lysis syndrome [see Warnings and Precautions (5.5)]
- Infections [see Warnings and Precautions (5.6)]
- Neutropenia [see Warnings and Precautions (5.7)]
- Thrombocytopenia [see Warnings and Precautions (5.8)]
- Disseminated intravascular coagulation [see Warnings and Precautions (5.9) ]
5.8 Thrombocytopenia
Severe and life-threatening thrombocytopenia has been reported during treatment with GAZYVA in combination with chemotherapy. Fatal hemorrhagic events have been reported in patients with NHL and CLL treated with GAZYVA in combination with chemotherapy, including during Cycle 1.
Monitor patients frequently for thrombocytopenia and hemorrhagic events, especially during the first cycle and if clinically indicated, evaluate laboratory coagulation parameters [see Warnings and Precautions (5.9)]. In patients with Grade 3 or 4 thrombocytopenia, monitor platelet counts more frequently until resolution and consider dose delays of GAZYVA and chemotherapy or dose reductions of chemotherapy. Transfusion of blood products (i.e., platelet transfusion) may be necessary. Consider withholding concomitant medications that may increase bleeding risk (platelet inhibitors, anticoagulants), especially during the first cycle.
12.2 Pharmacodynamics
In patients with CLL, GAZYVA caused CD19 B-cell depletion (defined as CD19 B cell counts < 0.07 × 109/L). Initial CD19 B cell recovery was observed in some patients approximately 9 months after the last GAZYVA dose. At 18 months of follow-up, some patients remain B cell depleted.
Although the depletion of B cells in the peripheral blood is a measurable pharmacodynamic effect, it is not directly correlated with the depletion of B-cells in solid organs or in malignant deposits. B cell depletion has not been shown to be directly correlated to clinical response.
In patients with LN (REGENCY study), total peripheral CD19+ B cell levels below the defined threshold of 10 cells/µl were achieved in 99% of patients treated with GAZYVA by Week 4 after treatment initiation and remained below this threshold in 95% of patients at Week 76.
Reductions in circulating naive B, memory B, and plasmablasts/plasma cells were observed by Week 4 and remained low through Week 76 after treatment initiation.
Treatment with GAZYVA led to improvements in complement (C3 and C4) and anti-double-stranded DNA antibodies (anti-dsDNA) by Week 4 and Week 12, respectively. These changes were sustained through Week 76.
In patients with low C3 at baseline, normalization of C3 levels occurred in 49% (by Week 12) and in 62% (by Week 76) of patients receiving GAZYVA compared to 33% and 29%, respectively, in the placebo group. In patients with low C4 at baseline, normalization of C4 levels occurred in 75% (by Week 12) and in 88% (by Week 76) of patients receiving GAZYVA compared to 55% and 55%, respectively, in the placebo group. Among patients with positive anti-dsDNA at baseline, 32% and 56% of patients treated with GAZYVA seroconverted by Week 4 and Week 76, respectively, compared with 16% and 16% of patients receiving placebo.
The clinical relevance of the above mentioned pharmacodynamic biomarkers has not been established.
12.3 Pharmacokinetics
The pharmacokinetic parameters of obinutuzumab after 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2-6 for CLL; after 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years for NHL; 1,000 mg on day 1, week 2, 24, 26 and every 6 months for up to 76 Weeks for LN are provided in Table 14. The dosing regimen is within the linear pharmacokinetic behavior of obinutuzumab.
| PK Measure | CLL Induction Cycle 6 of a 28-day cycle;
|
Relapsed or refractory FL | First line FL in combination with chemotherapy | LN Steady state values
|
|
|---|---|---|---|---|---|
| GAZYVA + Bendamustine | GAZYVA + CHOP or CVP Induction Cycle 8 of a 21-day cycle.
|
||||
| Results are presented as geometric mean (% Coefficient of Variation). | |||||
| Cmax, µg/mL | 466.3 (35) | 553.5 (32) | 513.4 (28) | 676.4 (30) | 463 (18) |
| Ctrough, µg/mL | 192.5 (78) | 295 (56) | 255 (46) | 395 (44) | 0.91 (752) |
| AUC, µg/mL*day | 8701 (51) | 11362 (41) | 10088 (35) | 10723 (37) | 8770 (38) |
1 Indications and Usage
GAZYVA is a CD20-directed cytolytic antibody indicated:
- in combination with chlorambucil, for the treatment of patients with previously untreated chronic lymphocytic leukemia (CLL). (1.1, 14)
- in combination with bendamustine followed by GAZYVA monotherapy, for the treatment of patients with follicular lymphoma (FL)who relapsed after, or are refractory to, a rituximab-containing regimen. (1.2, 14)
- in combination with chemotherapy followed by GAZYVA monotherapy in patients achieving at least a partial remission, for the treatment of adult patients with previously untreated stage II bulky, III or IV follicular lymphoma. (1.2, 14)
- for the treatment of adult patients with active lupus nephritis (LN) who are receiving standard therapy (1.3, 14)
1.3 Lupus Nephritis (ln)
GAZYVA is indicated for the treatment of adult patients with active lupus nephritis who are receiving standard therapy.
12.1 Mechanism of Action
Obinutuzumab is a monoclonal antibody that targets the CD20 antigen expressed on the surface of pre-B and mature B lymphocytes. Upon binding to CD20, obinutuzumab mediates B-cell lysis through (1) engagement of immune effector cells, (2) by directly activating intracellular death signaling pathways (direct cell death), and/or (3) activation of the complement cascade. The immune effector cell mechanisms include antibody-dependent cellular cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis.
As an antibody with reduced fucose content, obinutuzumab induces greater ADCC activity than rituximab in vitro using human cancer cell lines. Obinutuzumab also demonstrated an increased ability to induce direct cell death when compared to rituximab. Obinutuzumab binds to FcγRIII using purified proteins with a higher affinity than rituximab. Obinutuzumab and rituximab bind with similar affinity to overlapping epitopes on CD20.
5.5 Tumor Lysis Syndrome
Tumor lysis syndrome (TLS), including fatal cases, has been reported in patients with CLL and NHL receiving GAZYVA. Patients with high tumor burden, high circulating lymphocyte count (> 25 × 109/L) or renal impairment are at greater risk for TLS.
In patients with CLL and NHL at risk for TLS, administer appropriate tumor lysis prophylaxis with anti-hyperuricemics (e.g., allopurinol or rasburicase) and hydration prior to the infusion of GAZYVA [see Dosage and Administration (2.4)]. During the initial days of GAZYVA treatment, monitor the laboratory parameters of patients considered at risk for TLS. For treatment of TLS, correct electrolyte abnormalities, monitor renal function and fluid balance, and administer supportive care, including dialysis as indicated. TLS is not identified as a risk in LN.
5 Warnings and Precautions
- Infusion-Related Reactions: Premedicate patients with glucocorticoid, acetaminophen, and anti-histamine. Monitor patients closely during infusions. Interrupt, reduce rate, or discontinue for infusion-related reactions based on severity. (2.1, 5.3)
- Hypersensitivity Reactions Including Serum Sickness: Discontinue GAZYVA permanently. (5.4)
- Tumor Lysis Syndrome: In CLL and FL, premedicate with anti-hyperuricemics and adequate hydration, especially for patients with high tumor burden, high circulating lymphocyte count or renal impairment. Correct electrolyte abnormalities, provide supportive care, and monitor renal function and fluid balance. (5.5)
- Serious, Including Fatal, Infections: Do not administer GAZYVA to patients with an active infection. Patients with a history of recurring or chronic infections may be at increased risk of infection. (5.6)
- Neutropenia: In patients with Grade 3 to 4 neutropenia, monitor laboratory tests until resolution and for infection. Consider dose delays and infection prophylaxis, as appropriate. (5.7)
- Thrombocytopenia: Monitor for decreased platelet counts and bleeding. Transfusion may be necessary. (5.8)
- Disseminated Intravascular Coagulation: Evaluate cause and monitor for bleeding, thrombosis, and need for supportive care. (5.9)
- Immunization: Avoid administration of live virus vaccines during GAZYVA treatment and until B-cell recovery. (5.10)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of reproductive potential of the potential risk to a fetus and use effective contraception. (5.11)
5.11 Embryo Fetal Toxicity
Based on its mechanism of action and findings in animals, GAZYVA can cause B-cell depletion in infants exposed to obinutuzumab in-utero. Advise pregnant women of the potential risk to the fetus. Advise females of reproductive potential to use effective contraception while taking GAZYVA and for 6 months after the last dose [see Use in Specific Populations (8.1, 8.3)].
2 Dosage and Administration
- Premedicate for infusion-related reactions and tumor lysis syndrome. (2.1, 5.3, 5.4)
- Administer only as intravenous infusion. Do not administer as an intravenous push or bolus. (2.1)
- The recommended dosage for chronic lymphocytic leukemia is 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2–6. (2.2)
- The recommended dosage for follicular lymphoma is 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years. (2.3)
- The recommended dosage for active lupus nephritis is 1,000 mg at the initial infusion, on Week 2, 24, 26, and every 6 months thereafter. (2.4)
1.2 Follicular Lymphoma (fl)
GAZYVA, in combination with bendamustine followed by GAZYVA monotherapy, is indicated for the treatment of patients with follicular lymphoma who relapsed after, or are refractory to, a rituximab-containing regimen.
GAZYVA, in combination with chemotherapy followed by GAZYVA monotherapy in patients achieving at least a partial remission, is indicated for the treatment of adult patients with previously untreated stage II bulky, III or IV follicular lymphoma.
3 Dosage Forms and Strengths
Injection: 1,000 mg/40 mL (25 mg/mL) clear, colorless to slightly brown solution in a single-dose vial.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of GAZYVA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Immune/Autoimmune Events: Serum sickness
8 Use in Specific Populations
- Lactation: Advise not to breastfeed. (8.1)
5.3 Infusion Related Reactions
GAZYVA can cause severe and life-threatening infusion-related reactions (IRRs). Sixty-five percent of patients with CLL experienced a reaction to the first 1,000 mg of GAZYVA infused. Thirty-seven percent of patients with relapsed or refractory NHL and 60% of patients with previously untreated NHL experienced a reaction on Day 1 of GAZYVA infusion. In patients with CLL and NHL , IRRs have occurred within 24 hours of receiving GAZYVA. IRRs can also occur with subsequent infusions. Symptoms may include hypotension, tachycardia, dyspnea, and respiratory symptoms (e.g., bronchospasm, larynx and throat irritation, wheezing, laryngeal edema). The most frequently reported IRR symptoms in patients with CLL and NHL include nausea, fatigue, chest discomfort, dyspnea, dizziness, vomiting, diarrhea, rash, hypertension, hypotension, flushing, headache, pyrexia, and chills [see Adverse Reactions (6.1)].
In patients with LN, IRRs occurred predominantly during infusion of the first 1,000 mg. IRRs were generally mild to moderate and could be managed by the slowing or temporarily halting the infusion [see Dosage and Administration (2.6)]. Severe and life-threatening IRRs requiring symptomatic treatment were also reported. The most common IRR signs or symptoms reported in the REGENCY study included headache, nausea and vomiting. In the NOBILITY study, the most common IRR symptoms were pyrexia and tachycardia [see Adverse Reactions (6.2)].
Premedicate patients with acetaminophen, anti-histamine, and a glucocorticoid [see Dosage and Administration (2.4)]. Closely monitor patients during the entire infusion. Reduce infusion rate, interrupt infusion or permanently discontinue GAZYVA for IRRs based on severity [see Dosage and Administration (2.5)]. Institute medical management (e.g., glucocorticoids, epinephrine, bronchodilators, and/or oxygen) for IRRs as needed.
For patients with preexisting cardiac or pulmonary conditions, monitor more frequently throughout the infusion and the post-infusion period since they may be at greater risk of experiencing more severe reactions. Hypotension may occur as part of the IRR to GAZYVA. Consider withholding antihypertensive treatments for 12 hours prior to, during each GAZYVA infusion, and for the first hour after administration until blood pressure is stable. For patients at increased risk of hypertensive crisis, consider the benefits versus the risks of withholding their antihypertensive medication as is suggested here.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
2.1 Important Dosing Information
- Premedicate before each infusion [see Dosage and Administration (2.4)].
- Provide prophylactic hydration and anti-hyperuricemics to patients at high risk of tumor lysis syndrome [see Dosage and Administration (2.4) and Warnings and Precautions (5.4)].
- Administer only as an intravenous infusion through a dedicated line [see Dosage and Administration (2.6)].
- Do not administer as an intravenous push or bolus.
- Monitor blood counts at regular intervals.
- GAZYVA should only be administered by a healthcare professional with appropriate medical support to manage severe infusion-related reactions that can be fatal if they occur [see Warnings and Precautions (5.3)].
14.1 Chronic Lymphocytic Leukemia
The efficacy of GAZYVA was evaluated in a three-arm, open-label, active-controlled, randomized, multicenter trial (CLL11; NCT01010061) in 781 patients with previously untreated CD20+ CLL requiring treatment who had coexisting medical conditions or reduced renal function as measured by creatinine clearance (CLcr) < 70 mL/min. Patients with CLcr < 30 mL/min, active infections, positive hepatitis B (HBsAg or anti-HBc positive; patients positive for anti-HBc could be included if hepatitis B viral DNA was not detectable) and hepatitis C serology, or immunization with live virus vaccine within 28 days prior to randomization were excluded from the trial. Patients were treated with chlorambucil control (Arm 1), GAZYVA in combination with chlorambucil (Arm 2), or rituximab product in combination with chlorambucil (Arm 3). The safety and efficacy of GAZYVA was evaluated in a Stage 1 comparison of Arm 1 vs. Arm 2 in 356 patients and a Stage 2 comparison of Arm 2 vs. Arm 3 in 663 patients.
The majority of patients received 1,000 mg of GAZYVA on days 1, 8 and 15 of the first cycle, followed by treatment on the first day of 5 subsequent cycles (total of 6 cycles, 28 days each). The first dose of GAZYVA was divided between day 1 (100 mg) and day 2 (900 mg) [see Dosage and Administration (2.2)], which was implemented in 140 patients. Chlorambucil was given orally at 0.5 mg/kg on day 1 and day 15 of all treatment cycles (1 to 6).
In CLL11, the median age was 73 years, 62% were male, and 95% were White. Sixty-five percent had a CLcr < 70 mL/min and 76% had multiple coexisting medical conditions. Twenty-two percent of patients were Binet stage A, 42% were stage B, and 36% were stage C. The median estimated CLcr was 62 mL/min. Eighty-one percent of patients treated with GAZYVA in combination with chlorambucil received all 6 cycles compared to 89% of patients in the rituximab product treated arm and 67% in the chlorambucil alone arm.
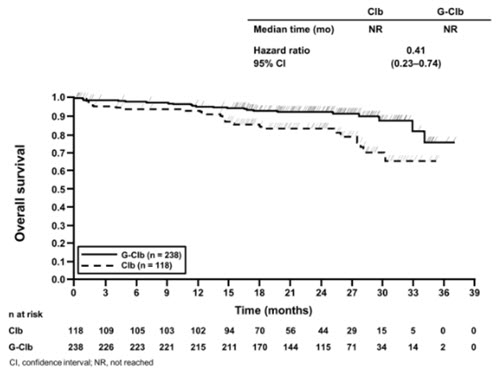
In the Stage 1 analysis of CLL11, the median progression-free survival (PFS) in the GAZYVA in combination with chlorambucil arm was 27.2 months and 11.2 months in the chlorambucil alone arm (median observation time 22.8 months) as assessed by independent review and is consistent with investigator-assessed PFS. The median overall survival (OS) was not yet reached with a total of 46 deaths: 22 (9%) in the GAZYVA in combination with chlorambucil arm and 24 (20%) in the chlorambucil arm. The hazard ratio for OS was 0.41 (95% CI: 0.23-0.74).
In the Stage 2 analysis of CLL11, the median PFS was 26.7 months in the GAZYVA arm and 14.9 months in the rituximab product arm with a median observation time of 18.7 months (HR: 0.42, 95% CI: 0.33-0.54, p-value < 0.0001). These results were assessed by independent review and are consistent with investigator-assessed PFS. Minimal residual disease (MRD) was evaluated using allele-specific oligonucleotide polymerase chain reaction (ASO-PCR). The cutoff for a negative status was one CLL cell per 104 leukocytes in the sample (i.e., an MRD value of < 10-4 was considered negative). Among patients who achieved complete response (CR) and complete response with incomplete marrow recovery (CRi; 94 patients in the GAZYVA arm and 34 patients in the rituximab product arm), 18 patients (19%) had negative MRD in the bone marrow in the GAZYVA arm compared to 2 patients (6%) in the rituximab product arm. Out of the patients who achieved CR and CRi, 39 patients (41%) in the GAZYVA arm, and 4 patients (12%) in the rituximab product arm were MRD negative in peripheral blood samples collected at least 3 months after the end of treatment.
Efficacy results are shown in Table 16 and Figures 1 and 2.
| Endpoint | Stage 1 of CLL11 | Stage 2 of CLL11 | ||
|---|---|---|---|---|
| GAZYVA + Chlorambucil All Stage 1 GClb patients (n = 238) were included in the Stage 2 GClb population (n = 333).
|
Chlorambucil | GAZYVA + Chlorambucil | Rituximab product + Chlorambucil | |
| n = 238 | n = 118 | n = 333 | n = 330 | |
| Median Progression-Free Survival As defined by independent review. Investigator-assessed PFS was consistent with data from independent review.
|
27.2 months | 11.2 months | 26.7 months | 14.9 months |
| (HR 0.19 [0.14; 0.27], p-value < 0.0001 stratified log-rank test) | (HR 0.42 [0.33; 0.54], p-value < 0.0001 stratified log-rank test) | |||
| Overall Response Rate Defined as best overall response rate (ORR = CR + CRi + PR + nPR).
|
78.2% | 33.1% | 79.6% | 66.3% |
| Complete Response | 28.2% | 0 | 26.1% | 8.8% |
| Complete Response with Incomplete Marrow Recovery | 2.5% | 1.7% | 2.1% | 1.5% |
| Partial Response | 45.0% | 30.5% | 48.6% | 54.1% |
| Nodular Partial Response | 2.5% | 0.8% | 2.7% | 1.8% |
| Median Duration of Response | 22.4 months | 4.7 months | 19.6 months | 9.7 months |
| Overall Survival | HR 0.41 [0.23; 0.74] | Not Yet Mature |
|
Figure 1 Kaplan-Meier Curve of Overall Survival in Patients with CLL in CLL11 (Stage 1) |
|
Figure 2 Kaplan-Meier Curve of Progression-Free Survival in Patients with CLL in CLL11 (Stage 2) |
5.1 Hepatitis B Virus Reactivation
GAZYVA can cause Hepatitis B virus (HBV) reactivation. Hepatitis B virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients treated with anti-CD20 antibodies such as GAZYVA. HBV reactivation has been reported in patients who are hepatitis B surface antigen (HBsAg) positive and also in patients who are HBsAg negative but are hepatitis B core antibody (anti-HBc) positive. Reactivation has also occurred in patients who appear to have resolved hepatitis B infection (i.e., HBsAg negative, anti-HBc positive, and hepatitis B surface antibody [anti-HBs] positive).
HBV reactivation is defined as an abrupt increase in HBV replication manifesting as a rapid increase in serum HBV DNA level or detection of HBsAg in a person who was previously HBsAg negative and anti-HBc positive. Reactivation of HBV replication is often followed by hepatitis, i.e., increase in transaminase levels and, in severe cases, increase in bilirubin levels, liver failure, and death.
Screen all patients for HBV infection by measuring HBsAg and anti-HBc before initiating treatment with GAZYVA. For patients who show evidence of hepatitis B infection (HBsAg positive [regardless of antibody status] or HBsAg negative but anti-HBc positive), consult healthcare providers with expertise in managing hepatitis B regarding monitoring and consideration for HBV antiviral therapy.
Monitor patients with evidence of current or prior HBV infection for clinical and laboratory signs of hepatitis or HBV reactivation during and for several months following treatment with GAZYVA. HBV reactivation has been reported for other CD20-directed cytolytic antibodies following completion of therapy.
In patients who develop reactivation of HBV while receiving GAZYVA, immediately discontinue GAZYVA and any concomitant chemotherapy and institute appropriate treatment. Resumption of GAZYVA in patients whose HBV reactivation resolves should be discussed with healthcare providers with expertise in managing hepatitis B. Insufficient data exist regarding the safety of resuming GAZYVA in patients who develop HBV reactivation.
16 How Supplied/storage and Handling
GAZYVA (obinutuzumab) injection is a clear, colorless to slightly brown, preservative-free solution for intravenous use supplied as 1,000 mg/40 mL (25 mg/mL) in single-dose vials (NDC 50242-070-01).
1.1 Chronic Lymphocytic Leukemia (cll)
GAZYVA, in combination with chlorambucil, is indicated for the treatment of patients with previously untreated chronic lymphocytic leukemia.
5.6 Serious, Including Fatal, Infections
Fatal and serious bacterial, fungal, and new or reactivated viral infections can occur during and following GAZYVA therapy. When GAZYVA is administered with chemotherapy followed by GAZYVA monotherapy as in the GALLIUM study, Grade 3 to 5 infections have been reported in up to 8% of patients during combination therapy, up to 13% of patients during monotherapy, and up to 8% of patients after treatment [see Adverse Reactions (6.1)].
Principal Display Panel 40 Ml Vial Carton
NDC 50242-070-01
Gazyva®
(obinutuzumab)
Injection
1000 mg/40 mL
(25 mg/mL)
For Intravenous Infusion After Dilution.
Single-Dose Vial. Discard Unused Portion.
No preservative.
1 vial
Rx only
Genentech
10240530
2.3 Recommended Dosage for Follicular Lymphoma
Each dose of GAZYVA is 1,000 mg administered intravenously according to Table 2.
For patients with relapsed or refractory FL, administer GAZYVA in combination with bendamustine in six 28-day cycles. Patients who achieve stable disease, complete response, or partial response to the initial 6 cycles should continue on GAZYVA 1,000 mg as monotherapy for up to two years.
For patients with previously untreated FL, administer GAZYVA with one of the following chemotherapy regimens:
- Six 28-day cycles in combination with bendamustine
- Six 21-day cycles in combination with CHOP, followed by 2 additional 21-day cycles of GAZYVA alone
- Eight 21-day cycles in combination with CVP
Patients with previously untreated FL who achieve a complete response or partial response to the initial 6 or 8 cycles should continue on GAZYVA 1,000 mg as monotherapy for up to two years.
GAZYVA should be administered at the standard infusion rate in Cycle 1 (see Table 2). In patients with FL who do not experience a Grade 3 or higher IRR during Cycle 1, GAZYVA may be administered as a shorter, approximately 90-minute infusion from Cycle 2 onwards (see Table 3) with continued premedication.
| Day of treatment cycle | Dose of GAZYVA | Rate of infusion | |
|---|---|---|---|
|
Cycle 1 (loading doses) |
Day 1 | 1,000 mg | Administer at 50 mg/hr. The rate of the infusion can be escalated in 50 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. |
| Day 8 | 1,000 mg | If no infusion-related reaction or an infusion-related reaction of Grade 1 occurred during the previous infusion and the final infusion rate was 100 mg/hr or faster, infusions can be started at a rate of 100 mg/hr and increased by 100 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. If an infusion-related reaction of Grade 2 or higher occurred during the previous infusion, administer at 50 mg/hr. The rate of infusion can be escalated in increments of 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. |
|
| Day 15 | 1,000 mg | ||
| Cycles 2–6 or 2–8 | Day 1 | 1,000 mg | |
| Monotherapy | Every two months for up to two years | 1,000 mg |
| Day of treatment cycle | Dose of GAZYVA | Rate of infusion | |
|---|---|---|---|
| Cycle 1 | Days 1, 8, 15 | 1,000 mg | See Table 2 |
|
Cycles 2–6 Consider an approximately 90-minute infusion in patients with FL who do not experience a Grade 3 or higher infusion-related reaction to GAZYVA in Cycle 1 and subsequent cycles. or 2-8
|
Day 1 | 1,000 mg | If no Grade 3 or higher IRR occurred during Cycle 1: 100 mg/hr for 30 minutes, then 900 mg/hr for approximately 60 minutes. If an IRR of Grade 1-2 with ongoing symptoms or a Grade 3 or higher IRR occurred during the previous approximately 90-minute infusion, administer all subsequent GAZYVA infusions at the standard infusion rate (see Table 2). |
| Monotherapy | Every two months for up to two years | 1,000 mg |
If a planned dose of GAZYVA is missed, administer the missed dose as soon as possible. During GAZYVA and chemotherapy treatment, adjust the dosing schedule accordingly to maintain the time interval between chemotherapy cycles. During monotherapy, maintain the original dosing schedule for subsequent doses. Initiate monotherapy approximately two months after the last dose of GAZYVA administered during the induction phase.
5.2 Progressive Multifocal Leukoencephalopathy
John Cunningham (JC) virus infection resulting in progressive multifocal leukoencephalopathy (PML), which can be fatal, occurred in patients treated with GAZYVA for CLL and NHL. Consider the diagnosis of PML in any patient presenting with new onset or changes to preexisting neurologic manifestations. Evaluation of PML includes, but is not limited to, consultation with a neurologist, brain MRI, and lumbar puncture. Discontinue GAZYVA therapy and consider discontinuation or reduction of any concomitant chemotherapy or immunosuppressive therapy in patients who develop PML.
5.9 Disseminated Intravascular Coagulation (dic)
Fatal and severe DIC has been reported in patients receiving GAZYVA for treatment of CLL and NHL. The majority of DIC cases have involved changes in platelets and laboratory coagulation parameters following the first infusion, with spontaneous resolution usually occurring by Day 8. In some cases, DIC was associated with IRRs, TLS, or both [see Adverse Reactions (6.1)].
In patients with suspected DIC, evaluate potential causes, and monitor coagulation parameters, platelet counts, and for signs and symptoms of bleeding or thrombosis. Manage according to standard guidelines for DIC. Supportive care, including transfusion of blood products and other medical management, may be necessary.
2.4 Recommended Dosage for Active Lupus Nephritis
Each recommended dose of GAZYVA is 1,000 mg administered intravenously according to Table 4.
| Dose number | Timing of treatment | Dose of GAZYVA | Rate of infusion |
|---|---|---|---|
| 1 | Initial infusion | 1,000 mg | Administer at a rate of 50 mg/hr. The rate of infusion can be escalated in 50 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. For management of IRRs that occur during infusion, see Dosage Modifications for Adverse Reactions (2.6) . |
| 2 | Week 2 (two weeks after Dose 1) |
1,000 mg | Administer at a rate of 100 mg/hr. The rate of infusion can be escalated at a rate of 100 mg/hr every 30 minutes to a maximum of 400 mg/hr. |
| 3 | Week 24 | 1,000 mg | |
| 4 | Week 26 (two weeks after Dose 3) |
1,000 mg | |
|
5
Dose 5 should be administered six months after Dose 4 and thereafter
|
Every 6 months | 1,000 mg |
Patients who do not experience Grade ≥ 3 infusion related reactions during the previous infusion may receive GAZYVA over approximately 90 minutes from Dose 2 onwards (see Table 5), with continued premedication.
| Dose number | Rate of infusion |
|---|---|
| 1 | See Table 4 |
|
2 and thereafter (if no Grade 3 or higher IRR during previous infusion) |
100 mg/hr for 30 minutes, then 900 mg/hr for approximately 60 minutes. If an IRR of Grade 1-2 with ongoing symptoms or a Grade 3 or higher IRR occurs during the previous approximately 90-minute infusion, administer GAZYVA at the standard infusion rate (see Table 4). |
If a planned dose of GAZYVA is missed, it should be administered as soon as possible – do not wait until the next planned dose. The schedule of administration should be adjusted to maintain the appropriate interval between doses.
2.2 Recommended Dosage for Chronic Lymphocytic Leukemia
Each dose of GAZYVA is 1,000 mg administered intravenously with the exception of the first infusions in Cycle 1, which are administered on day 1 (100 mg) and day 2 (900 mg) according to Table 1.
| Day of treatment cycle | Dose of GAZYVA | Rate of infusion | |
|---|---|---|---|
|
Cycle 1 (loading doses) |
Day 1 | 100 mg | Administer at 25 mg/hr over 4 hours. Do not increase the infusion rate. |
| Day 2 | 900 mg | If no infusion-related reaction (IRR) occurred during the previous infusion, administer at 50 mg/hr. The rate of the infusion can be escalated in increments of 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. If an IRR occurred during the previous infusion, administer at 25 mg/hr. The rate of infusion can be escalated in increments of up to 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. |
|
| Day 8 | 1,000 mg | If no IRR occurred during the previous infusion and the final infusion rate was 100 mg/hr or faster, infusions can be started at a rate of 100 mg/hr and increased by 100 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. If an infusion-related reaction occurred during the previous infusion, administer at 50 mg/hr. The rate of infusion can be escalated in increments of 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. |
|
| Day 15 | 1,000 mg | ||
| Cycles 2–6 | Day 1 | 1,000 mg |
If a planned dose of GAZYVA is missed, administer the missed dose as soon as possible and adjust dosing schedule to maintain the time interval between doses. If appropriate, patients who do not complete the Day 1 Cycle 1 dose may proceed to the Day 2 Cycle 1 dose.
5.4 Hypersensitivity Reactions Including Serum Sickness
Hypersensitivity reactions have been reported in patients treated with GAZYVA. Signs of immediate-onset hypersensitivity included dyspnea, bronchospasm, hypotension, urticaria and tachycardia. Late-onset hypersensitivity diagnosed as serum sickness has also been reported, with symptoms that include chest pain, diffuse arthralgia and fever. Hypersensitivity reactions may be difficult to clinically distinguish from IRRs. However, hypersensitivity very rarely occurs with the first infusion and, when observed, often occurs after previous exposure.
If a hypersensitivity reaction is suspected during or after an infusion, stop the infusion and permanently discontinue treatment. GAZYVA is contraindicated in patients with known hypersensitivity reactions to GAZYVA, including serum sickness with prior GAZYVA use [see Contraindications (4)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity or genotoxicity studies have been conducted with obinutuzumab.
No specific studies have been conducted to evaluate potential effects on fertility; however, no adverse effects on male or female reproductive organs were observed in the 26-week repeat-dose toxicity study in cynomolgus monkeys.
Warning: Hepatitis B Virus Reactivation and Progressive Multifocal Leukoencephalopathy
- Hepatitis B Virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients receiving CD20-directed cytolytic antibodies, including GAZYVA. Screen all patients for HBV infection before treatment initiation. Monitor HBV-positive patients during and after treatment with GAZYVA. Discontinue GAZYVA and concomitant medications in the event of HBV reactivation [see Warnings and Precautions (5.1)].
- Progressive Multifocal Leukoencephalopathy (PML) including fatal PML, can occur in patients receiving GAZYVA [see Warnings and Precautions (5.2)].
Structured Label Content
Section 42229-5 (42229-5)
Infusion-Related Reactions
Premedication to reduce the risk of IRRs is outlined in Table 6 [see Warnings and Precautions (5.3)].
Hypotension may occur during GAZYVA intravenous infusions. Consider withholding antihypertensive treatments for 12 hours prior to and throughout each GAZYVA infusion and for the first hour after administration [see Warnings and Precautions (5.3)].
| Indication/Cycle/Day of Treatment | Patients requiring premedication | Premedication | Administration |
|---|---|---|---|
| Premedication applies to both standard and approximately 90-minute infusions. | |||
|
CLL Cycle 1 Days 1 and 2 FL Cycle 1 Day 1 |
All patients | Intravenous glucocorticoid: 20 mg dexamethasone or 80 mg methylprednisolone Hydrocortisone is not recommended as it has not been effective in reducing the rate of IRRs.
,
If a glucocorticoid-containing chemotherapy regimen is administered on the same day as GAZYVA, the glucocorticoid can be administered as an oral medication if given at least 1 hour prior to GAZYVA, in which case additional intravenous glucocorticoid as premedication is not required.
|
Completed at least 1 hour prior to GAZYVA infusion. |
| 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. | ||
| anti-histamine (e.g., 50 mg diphenhydramine) | |||
|
CLL or FL All subsequent infusions |
All patients | 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. |
| Patients with an IRR (Grade 1-2) with the previous infusion | 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. | |
| anti-histamine (e.g., 50 mg diphenhydramine) | |||
| Patients with a Grade 3 IRR with the previous infusion OR with a lymphocyte count > 25 × 109/L prior to next treatment | Intravenous glucocorticoid: 20 mg dexamethasone or 80 mg methylprednisolone |
Completed at least 1 hour prior to GAZYVA infusion. | |
| 650–1,000 mg acetaminophen | At least 30 minutes before GAZYVA infusion. | ||
| anti-histamine (e.g., 50 mg diphenhydramine) | |||
| LN | All patients | Intravenous glucocorticoid (80 mg methylprednisolone) | Completed between 30 and 60 minutes prior to GAZYVA infusion Starting from Dose 6, intravenous corticosteroid should only be administered to patients who have experienced an IRR in the prior infusion |
| 650–1,000 mg acetaminophen | |||
| anti-histamine (e.g., 50 mg diphenhydramine) |
Section 43683-2 (43683-2)
Section 44425-7 (44425-7)
Store at 2°C to 8°C (36°F to 46°F). Do not use beyond expiration date stamped on carton. Protect from light. DO NOT FREEZE. DO NOT SHAKE.
10 Overdosage (10 OVERDOSAGE)
There has been no experience with overdose in human clinical trials. For patients who experience overdose, treatment should consist of immediate interruption or reduction of GAZYVA and supportive therapy.
11 Description (11 DESCRIPTION)
Obinutuzumab is a humanized anti-CD20 monoclonal antibody of the IgG1 subclass. It recognizes a specific epitope of the CD20 molecule found on B cells. The molecular mass of the antibody is approximately 150 kDa.
GAZYVA (obinutuzumab) injection is produced by mammalian cell (CHO) suspension culture. GAZYVA was engineered to have reduced fucose content as compared to a typical IgG1 produced in CHO cells. GAZYVA is a sterile, clear, colorless to slightly brown, preservative-free liquid concentrate for intravenous use. GAZYVA is supplied at a concentration of 25 mg/mL in 1,000 mg single-dose vials. Each vial contains in 40 mL: 1,000 mg obinutuzumab, L-histidine (57.6 mg), L-histidine hydrochloride monohydrate (89.6 mg), trehalose dihydrate (3632 mg), and poloxamer 188 (8 mg). The pH is 6.0.
5.7 Neutropenia
Severe and life-threatening neutropenia, including febrile neutropenia, has been reported during treatment with GAZYVA. Monitor patients with Grade 3 to 4 neutropenia frequently with regular laboratory tests until resolution. Anticipate, evaluate, and treat any symptoms or signs of developing infection. Consider dose delays for Grade 3 or 4 neutropenia. Consider administration of granulocyte colony-stimulating factors (GCSF) in patients with Grade 3 or 4 neutropenia.
Neutropenia can also be of late onset (occurring more than 28 days after completion of treatment) and/or prolonged (lasting longer than 28 days). Patients with severe and long lasting (> 1 week) neutropenia are strongly recommended to receive antimicrobial prophylaxis until resolution of neutropenia to Grade 1 or 2. Consider antiviral and antifungal prophylaxis.
5.10 Immunization
The safety and efficacy of immunization with live or attenuated viral vaccines during or following GAZYVA therapy have not been studied. Immunization with live virus vaccines is not recommended during treatment with GAZYVA and until B-cell recovery.
8.4 Pediatric Use
The safety and effectiveness of GAZYVA in pediatric patients have not been established.
12.6 Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of anti-drug antibody (ADA) (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies or to other products may be misleading.
Seven percent (18/271) of patients with CLL tested positive for anti-GAZYVA antibodies at one or more time points in CLL11. No patients developed anti-GAZYVA antibodies during or following GAZYVA treatment in GADOLIN, while 1 patient (1/564, 0.2%) developed anti-GAZYVA antibodies in GALLIUM. Neutralizing activity of anti-GAZYVA antibodies was not assessed.
In GAZYVA-treated patients in the LN studies, a total of 12 out of 200 (6%) had at least one ADA-positive sample recorded at any time during the studies. Six (3%) subjects had ADA-positive samples recorded at baseline in which two patients remained ADA-positive throughout the studies, one patient had a single post-baseline sample that was ADA-positive, and three patients had post-baseline samples that were all ADA-negative. Six (3%) patients with ADA-negative samples at baseline had a positive ADA titer post-baseline (treatment-induced ADA). None of the 12 patients with positive ADA titers at any time during the treatment period experienced an IRR or hypersensitivity reaction during the studies. Neutralizing activity of anti-GAZYVA antibodies was not assessed.
Because of the low occurrence of anti-drug antibodies, the effect of these antibodies on the pharmacokinetics, pharmacodynamics, safety and/or effectiveness of GAZYVA is unknown.
4 Contraindications (4 CONTRAINDICATIONS)
GAZYVA is contraindicated in patients with known hypersensitivity reactions (e.g., anaphylaxis) to obinutuzumab or to any of the excipients, or serum sickness with prior obinutuzumab use [see Warnings and Precautions (5.4)].
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hepatitis B virus reactivation [see Warnings and Precautions (5.1)]
- Progressive multifocal leukoencephalopathy [see Warnings and Precautions (5.2)]
- Infusion-related reactions [see Warnings and Precautions (5.3)]
- Hypersensitivity reactions including serum sickness [see Warnings and Precautions (5.4)]
- Tumor lysis syndrome [see Warnings and Precautions (5.5)]
- Infections [see Warnings and Precautions (5.6)]
- Neutropenia [see Warnings and Precautions (5.7)]
- Thrombocytopenia [see Warnings and Precautions (5.8)]
- Disseminated intravascular coagulation [see Warnings and Precautions (5.9) ]
5.8 Thrombocytopenia
Severe and life-threatening thrombocytopenia has been reported during treatment with GAZYVA in combination with chemotherapy. Fatal hemorrhagic events have been reported in patients with NHL and CLL treated with GAZYVA in combination with chemotherapy, including during Cycle 1.
Monitor patients frequently for thrombocytopenia and hemorrhagic events, especially during the first cycle and if clinically indicated, evaluate laboratory coagulation parameters [see Warnings and Precautions (5.9)]. In patients with Grade 3 or 4 thrombocytopenia, monitor platelet counts more frequently until resolution and consider dose delays of GAZYVA and chemotherapy or dose reductions of chemotherapy. Transfusion of blood products (i.e., platelet transfusion) may be necessary. Consider withholding concomitant medications that may increase bleeding risk (platelet inhibitors, anticoagulants), especially during the first cycle.
12.2 Pharmacodynamics
In patients with CLL, GAZYVA caused CD19 B-cell depletion (defined as CD19 B cell counts < 0.07 × 109/L). Initial CD19 B cell recovery was observed in some patients approximately 9 months after the last GAZYVA dose. At 18 months of follow-up, some patients remain B cell depleted.
Although the depletion of B cells in the peripheral blood is a measurable pharmacodynamic effect, it is not directly correlated with the depletion of B-cells in solid organs or in malignant deposits. B cell depletion has not been shown to be directly correlated to clinical response.
In patients with LN (REGENCY study), total peripheral CD19+ B cell levels below the defined threshold of 10 cells/µl were achieved in 99% of patients treated with GAZYVA by Week 4 after treatment initiation and remained below this threshold in 95% of patients at Week 76.
Reductions in circulating naive B, memory B, and plasmablasts/plasma cells were observed by Week 4 and remained low through Week 76 after treatment initiation.
Treatment with GAZYVA led to improvements in complement (C3 and C4) and anti-double-stranded DNA antibodies (anti-dsDNA) by Week 4 and Week 12, respectively. These changes were sustained through Week 76.
In patients with low C3 at baseline, normalization of C3 levels occurred in 49% (by Week 12) and in 62% (by Week 76) of patients receiving GAZYVA compared to 33% and 29%, respectively, in the placebo group. In patients with low C4 at baseline, normalization of C4 levels occurred in 75% (by Week 12) and in 88% (by Week 76) of patients receiving GAZYVA compared to 55% and 55%, respectively, in the placebo group. Among patients with positive anti-dsDNA at baseline, 32% and 56% of patients treated with GAZYVA seroconverted by Week 4 and Week 76, respectively, compared with 16% and 16% of patients receiving placebo.
The clinical relevance of the above mentioned pharmacodynamic biomarkers has not been established.
12.3 Pharmacokinetics
The pharmacokinetic parameters of obinutuzumab after 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2-6 for CLL; after 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years for NHL; 1,000 mg on day 1, week 2, 24, 26 and every 6 months for up to 76 Weeks for LN are provided in Table 14. The dosing regimen is within the linear pharmacokinetic behavior of obinutuzumab.
| PK Measure | CLL Induction Cycle 6 of a 28-day cycle;
|
Relapsed or refractory FL | First line FL in combination with chemotherapy | LN Steady state values
|
|
|---|---|---|---|---|---|
| GAZYVA + Bendamustine | GAZYVA + CHOP or CVP Induction Cycle 8 of a 21-day cycle.
|
||||
| Results are presented as geometric mean (% Coefficient of Variation). | |||||
| Cmax, µg/mL | 466.3 (35) | 553.5 (32) | 513.4 (28) | 676.4 (30) | 463 (18) |
| Ctrough, µg/mL | 192.5 (78) | 295 (56) | 255 (46) | 395 (44) | 0.91 (752) |
| AUC, µg/mL*day | 8701 (51) | 11362 (41) | 10088 (35) | 10723 (37) | 8770 (38) |
1 Indications and Usage (1 INDICATIONS AND USAGE)
GAZYVA is a CD20-directed cytolytic antibody indicated:
- in combination with chlorambucil, for the treatment of patients with previously untreated chronic lymphocytic leukemia (CLL). (1.1, 14)
- in combination with bendamustine followed by GAZYVA monotherapy, for the treatment of patients with follicular lymphoma (FL)who relapsed after, or are refractory to, a rituximab-containing regimen. (1.2, 14)
- in combination with chemotherapy followed by GAZYVA monotherapy in patients achieving at least a partial remission, for the treatment of adult patients with previously untreated stage II bulky, III or IV follicular lymphoma. (1.2, 14)
- for the treatment of adult patients with active lupus nephritis (LN) who are receiving standard therapy (1.3, 14)
1.3 Lupus Nephritis (ln) (1.3 Lupus Nephritis (LN))
GAZYVA is indicated for the treatment of adult patients with active lupus nephritis who are receiving standard therapy.
12.1 Mechanism of Action
Obinutuzumab is a monoclonal antibody that targets the CD20 antigen expressed on the surface of pre-B and mature B lymphocytes. Upon binding to CD20, obinutuzumab mediates B-cell lysis through (1) engagement of immune effector cells, (2) by directly activating intracellular death signaling pathways (direct cell death), and/or (3) activation of the complement cascade. The immune effector cell mechanisms include antibody-dependent cellular cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis.
As an antibody with reduced fucose content, obinutuzumab induces greater ADCC activity than rituximab in vitro using human cancer cell lines. Obinutuzumab also demonstrated an increased ability to induce direct cell death when compared to rituximab. Obinutuzumab binds to FcγRIII using purified proteins with a higher affinity than rituximab. Obinutuzumab and rituximab bind with similar affinity to overlapping epitopes on CD20.
5.5 Tumor Lysis Syndrome
Tumor lysis syndrome (TLS), including fatal cases, has been reported in patients with CLL and NHL receiving GAZYVA. Patients with high tumor burden, high circulating lymphocyte count (> 25 × 109/L) or renal impairment are at greater risk for TLS.
In patients with CLL and NHL at risk for TLS, administer appropriate tumor lysis prophylaxis with anti-hyperuricemics (e.g., allopurinol or rasburicase) and hydration prior to the infusion of GAZYVA [see Dosage and Administration (2.4)]. During the initial days of GAZYVA treatment, monitor the laboratory parameters of patients considered at risk for TLS. For treatment of TLS, correct electrolyte abnormalities, monitor renal function and fluid balance, and administer supportive care, including dialysis as indicated. TLS is not identified as a risk in LN.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Infusion-Related Reactions: Premedicate patients with glucocorticoid, acetaminophen, and anti-histamine. Monitor patients closely during infusions. Interrupt, reduce rate, or discontinue for infusion-related reactions based on severity. (2.1, 5.3)
- Hypersensitivity Reactions Including Serum Sickness: Discontinue GAZYVA permanently. (5.4)
- Tumor Lysis Syndrome: In CLL and FL, premedicate with anti-hyperuricemics and adequate hydration, especially for patients with high tumor burden, high circulating lymphocyte count or renal impairment. Correct electrolyte abnormalities, provide supportive care, and monitor renal function and fluid balance. (5.5)
- Serious, Including Fatal, Infections: Do not administer GAZYVA to patients with an active infection. Patients with a history of recurring or chronic infections may be at increased risk of infection. (5.6)
- Neutropenia: In patients with Grade 3 to 4 neutropenia, monitor laboratory tests until resolution and for infection. Consider dose delays and infection prophylaxis, as appropriate. (5.7)
- Thrombocytopenia: Monitor for decreased platelet counts and bleeding. Transfusion may be necessary. (5.8)
- Disseminated Intravascular Coagulation: Evaluate cause and monitor for bleeding, thrombosis, and need for supportive care. (5.9)
- Immunization: Avoid administration of live virus vaccines during GAZYVA treatment and until B-cell recovery. (5.10)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise females of reproductive potential of the potential risk to a fetus and use effective contraception. (5.11)
5.11 Embryo Fetal Toxicity (5.11 Embryo-Fetal Toxicity)
Based on its mechanism of action and findings in animals, GAZYVA can cause B-cell depletion in infants exposed to obinutuzumab in-utero. Advise pregnant women of the potential risk to the fetus. Advise females of reproductive potential to use effective contraception while taking GAZYVA and for 6 months after the last dose [see Use in Specific Populations (8.1, 8.3)].
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
- Premedicate for infusion-related reactions and tumor lysis syndrome. (2.1, 5.3, 5.4)
- Administer only as intravenous infusion. Do not administer as an intravenous push or bolus. (2.1)
- The recommended dosage for chronic lymphocytic leukemia is 100 mg on day 1 and 900 mg on day 2 of Cycle 1, 1,000 mg on day 8 and 15 of Cycle 1, and 1,000 mg on day 1 of Cycles 2–6. (2.2)
- The recommended dosage for follicular lymphoma is 1,000 mg on day 1, 8 and 15 of Cycle 1, 1,000 mg on day 1 of Cycles 2-6 or Cycles 2-8, and then 1,000 mg every 2 months for up to 2 years. (2.3)
- The recommended dosage for active lupus nephritis is 1,000 mg at the initial infusion, on Week 2, 24, 26, and every 6 months thereafter. (2.4)
1.2 Follicular Lymphoma (fl) (1.2 Follicular Lymphoma (FL))
GAZYVA, in combination with bendamustine followed by GAZYVA monotherapy, is indicated for the treatment of patients with follicular lymphoma who relapsed after, or are refractory to, a rituximab-containing regimen.
GAZYVA, in combination with chemotherapy followed by GAZYVA monotherapy in patients achieving at least a partial remission, is indicated for the treatment of adult patients with previously untreated stage II bulky, III or IV follicular lymphoma.
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Injection: 1,000 mg/40 mL (25 mg/mL) clear, colorless to slightly brown solution in a single-dose vial.
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of GAZYVA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Immune/Autoimmune Events: Serum sickness
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Lactation: Advise not to breastfeed. (8.1)
5.3 Infusion Related Reactions (5.3 Infusion-Related Reactions)
GAZYVA can cause severe and life-threatening infusion-related reactions (IRRs). Sixty-five percent of patients with CLL experienced a reaction to the first 1,000 mg of GAZYVA infused. Thirty-seven percent of patients with relapsed or refractory NHL and 60% of patients with previously untreated NHL experienced a reaction on Day 1 of GAZYVA infusion. In patients with CLL and NHL , IRRs have occurred within 24 hours of receiving GAZYVA. IRRs can also occur with subsequent infusions. Symptoms may include hypotension, tachycardia, dyspnea, and respiratory symptoms (e.g., bronchospasm, larynx and throat irritation, wheezing, laryngeal edema). The most frequently reported IRR symptoms in patients with CLL and NHL include nausea, fatigue, chest discomfort, dyspnea, dizziness, vomiting, diarrhea, rash, hypertension, hypotension, flushing, headache, pyrexia, and chills [see Adverse Reactions (6.1)].
In patients with LN, IRRs occurred predominantly during infusion of the first 1,000 mg. IRRs were generally mild to moderate and could be managed by the slowing or temporarily halting the infusion [see Dosage and Administration (2.6)]. Severe and life-threatening IRRs requiring symptomatic treatment were also reported. The most common IRR signs or symptoms reported in the REGENCY study included headache, nausea and vomiting. In the NOBILITY study, the most common IRR symptoms were pyrexia and tachycardia [see Adverse Reactions (6.2)].
Premedicate patients with acetaminophen, anti-histamine, and a glucocorticoid [see Dosage and Administration (2.4)]. Closely monitor patients during the entire infusion. Reduce infusion rate, interrupt infusion or permanently discontinue GAZYVA for IRRs based on severity [see Dosage and Administration (2.5)]. Institute medical management (e.g., glucocorticoids, epinephrine, bronchodilators, and/or oxygen) for IRRs as needed.
For patients with preexisting cardiac or pulmonary conditions, monitor more frequently throughout the infusion and the post-infusion period since they may be at greater risk of experiencing more severe reactions. Hypotension may occur as part of the IRR to GAZYVA. Consider withholding antihypertensive treatments for 12 hours prior to, during each GAZYVA infusion, and for the first hour after administration until blood pressure is stable. For patients at increased risk of hypertensive crisis, consider the benefits versus the risks of withholding their antihypertensive medication as is suggested here.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
2.1 Important Dosing Information
- Premedicate before each infusion [see Dosage and Administration (2.4)].
- Provide prophylactic hydration and anti-hyperuricemics to patients at high risk of tumor lysis syndrome [see Dosage and Administration (2.4) and Warnings and Precautions (5.4)].
- Administer only as an intravenous infusion through a dedicated line [see Dosage and Administration (2.6)].
- Do not administer as an intravenous push or bolus.
- Monitor blood counts at regular intervals.
- GAZYVA should only be administered by a healthcare professional with appropriate medical support to manage severe infusion-related reactions that can be fatal if they occur [see Warnings and Precautions (5.3)].
14.1 Chronic Lymphocytic Leukemia
The efficacy of GAZYVA was evaluated in a three-arm, open-label, active-controlled, randomized, multicenter trial (CLL11; NCT01010061) in 781 patients with previously untreated CD20+ CLL requiring treatment who had coexisting medical conditions or reduced renal function as measured by creatinine clearance (CLcr) < 70 mL/min. Patients with CLcr < 30 mL/min, active infections, positive hepatitis B (HBsAg or anti-HBc positive; patients positive for anti-HBc could be included if hepatitis B viral DNA was not detectable) and hepatitis C serology, or immunization with live virus vaccine within 28 days prior to randomization were excluded from the trial. Patients were treated with chlorambucil control (Arm 1), GAZYVA in combination with chlorambucil (Arm 2), or rituximab product in combination with chlorambucil (Arm 3). The safety and efficacy of GAZYVA was evaluated in a Stage 1 comparison of Arm 1 vs. Arm 2 in 356 patients and a Stage 2 comparison of Arm 2 vs. Arm 3 in 663 patients.
The majority of patients received 1,000 mg of GAZYVA on days 1, 8 and 15 of the first cycle, followed by treatment on the first day of 5 subsequent cycles (total of 6 cycles, 28 days each). The first dose of GAZYVA was divided between day 1 (100 mg) and day 2 (900 mg) [see Dosage and Administration (2.2)], which was implemented in 140 patients. Chlorambucil was given orally at 0.5 mg/kg on day 1 and day 15 of all treatment cycles (1 to 6).
In CLL11, the median age was 73 years, 62% were male, and 95% were White. Sixty-five percent had a CLcr < 70 mL/min and 76% had multiple coexisting medical conditions. Twenty-two percent of patients were Binet stage A, 42% were stage B, and 36% were stage C. The median estimated CLcr was 62 mL/min. Eighty-one percent of patients treated with GAZYVA in combination with chlorambucil received all 6 cycles compared to 89% of patients in the rituximab product treated arm and 67% in the chlorambucil alone arm.
In the Stage 1 analysis of CLL11, the median progression-free survival (PFS) in the GAZYVA in combination with chlorambucil arm was 27.2 months and 11.2 months in the chlorambucil alone arm (median observation time 22.8 months) as assessed by independent review and is consistent with investigator-assessed PFS. The median overall survival (OS) was not yet reached with a total of 46 deaths: 22 (9%) in the GAZYVA in combination with chlorambucil arm and 24 (20%) in the chlorambucil arm. The hazard ratio for OS was 0.41 (95% CI: 0.23-0.74).
In the Stage 2 analysis of CLL11, the median PFS was 26.7 months in the GAZYVA arm and 14.9 months in the rituximab product arm with a median observation time of 18.7 months (HR: 0.42, 95% CI: 0.33-0.54, p-value < 0.0001). These results were assessed by independent review and are consistent with investigator-assessed PFS. Minimal residual disease (MRD) was evaluated using allele-specific oligonucleotide polymerase chain reaction (ASO-PCR). The cutoff for a negative status was one CLL cell per 104 leukocytes in the sample (i.e., an MRD value of < 10-4 was considered negative). Among patients who achieved complete response (CR) and complete response with incomplete marrow recovery (CRi; 94 patients in the GAZYVA arm and 34 patients in the rituximab product arm), 18 patients (19%) had negative MRD in the bone marrow in the GAZYVA arm compared to 2 patients (6%) in the rituximab product arm. Out of the patients who achieved CR and CRi, 39 patients (41%) in the GAZYVA arm, and 4 patients (12%) in the rituximab product arm were MRD negative in peripheral blood samples collected at least 3 months after the end of treatment.
Efficacy results are shown in Table 16 and Figures 1 and 2.
| Endpoint | Stage 1 of CLL11 | Stage 2 of CLL11 | ||
|---|---|---|---|---|
| GAZYVA + Chlorambucil All Stage 1 GClb patients (n = 238) were included in the Stage 2 GClb population (n = 333).
|
Chlorambucil | GAZYVA + Chlorambucil | Rituximab product + Chlorambucil | |
| n = 238 | n = 118 | n = 333 | n = 330 | |
| Median Progression-Free Survival As defined by independent review. Investigator-assessed PFS was consistent with data from independent review.
|
27.2 months | 11.2 months | 26.7 months | 14.9 months |
| (HR 0.19 [0.14; 0.27], p-value < 0.0001 stratified log-rank test) | (HR 0.42 [0.33; 0.54], p-value < 0.0001 stratified log-rank test) | |||
| Overall Response Rate Defined as best overall response rate (ORR = CR + CRi + PR + nPR).
|
78.2% | 33.1% | 79.6% | 66.3% |
| Complete Response | 28.2% | 0 | 26.1% | 8.8% |
| Complete Response with Incomplete Marrow Recovery | 2.5% | 1.7% | 2.1% | 1.5% |
| Partial Response | 45.0% | 30.5% | 48.6% | 54.1% |
| Nodular Partial Response | 2.5% | 0.8% | 2.7% | 1.8% |
| Median Duration of Response | 22.4 months | 4.7 months | 19.6 months | 9.7 months |
| Overall Survival | HR 0.41 [0.23; 0.74] | Not Yet Mature |
|
Figure 1 Kaplan-Meier Curve of Overall Survival in Patients with CLL in CLL11 (Stage 1) |
|
Figure 2 Kaplan-Meier Curve of Progression-Free Survival in Patients with CLL in CLL11 (Stage 2) |
5.1 Hepatitis B Virus Reactivation
GAZYVA can cause Hepatitis B virus (HBV) reactivation. Hepatitis B virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients treated with anti-CD20 antibodies such as GAZYVA. HBV reactivation has been reported in patients who are hepatitis B surface antigen (HBsAg) positive and also in patients who are HBsAg negative but are hepatitis B core antibody (anti-HBc) positive. Reactivation has also occurred in patients who appear to have resolved hepatitis B infection (i.e., HBsAg negative, anti-HBc positive, and hepatitis B surface antibody [anti-HBs] positive).
HBV reactivation is defined as an abrupt increase in HBV replication manifesting as a rapid increase in serum HBV DNA level or detection of HBsAg in a person who was previously HBsAg negative and anti-HBc positive. Reactivation of HBV replication is often followed by hepatitis, i.e., increase in transaminase levels and, in severe cases, increase in bilirubin levels, liver failure, and death.
Screen all patients for HBV infection by measuring HBsAg and anti-HBc before initiating treatment with GAZYVA. For patients who show evidence of hepatitis B infection (HBsAg positive [regardless of antibody status] or HBsAg negative but anti-HBc positive), consult healthcare providers with expertise in managing hepatitis B regarding monitoring and consideration for HBV antiviral therapy.
Monitor patients with evidence of current or prior HBV infection for clinical and laboratory signs of hepatitis or HBV reactivation during and for several months following treatment with GAZYVA. HBV reactivation has been reported for other CD20-directed cytolytic antibodies following completion of therapy.
In patients who develop reactivation of HBV while receiving GAZYVA, immediately discontinue GAZYVA and any concomitant chemotherapy and institute appropriate treatment. Resumption of GAZYVA in patients whose HBV reactivation resolves should be discussed with healthcare providers with expertise in managing hepatitis B. Insufficient data exist regarding the safety of resuming GAZYVA in patients who develop HBV reactivation.
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
GAZYVA (obinutuzumab) injection is a clear, colorless to slightly brown, preservative-free solution for intravenous use supplied as 1,000 mg/40 mL (25 mg/mL) in single-dose vials (NDC 50242-070-01).
1.1 Chronic Lymphocytic Leukemia (cll) (1.1 Chronic Lymphocytic Leukemia (CLL))
GAZYVA, in combination with chlorambucil, is indicated for the treatment of patients with previously untreated chronic lymphocytic leukemia.
5.6 Serious, Including Fatal, Infections
Fatal and serious bacterial, fungal, and new or reactivated viral infections can occur during and following GAZYVA therapy. When GAZYVA is administered with chemotherapy followed by GAZYVA monotherapy as in the GALLIUM study, Grade 3 to 5 infections have been reported in up to 8% of patients during combination therapy, up to 13% of patients during monotherapy, and up to 8% of patients after treatment [see Adverse Reactions (6.1)].
Principal Display Panel 40 Ml Vial Carton (PRINCIPAL DISPLAY PANEL - 40 mL Vial Carton)
NDC 50242-070-01
Gazyva®
(obinutuzumab)
Injection
1000 mg/40 mL
(25 mg/mL)
For Intravenous Infusion After Dilution.
Single-Dose Vial. Discard Unused Portion.
No preservative.
1 vial
Rx only
Genentech
10240530
2.3 Recommended Dosage for Follicular Lymphoma
Each dose of GAZYVA is 1,000 mg administered intravenously according to Table 2.
For patients with relapsed or refractory FL, administer GAZYVA in combination with bendamustine in six 28-day cycles. Patients who achieve stable disease, complete response, or partial response to the initial 6 cycles should continue on GAZYVA 1,000 mg as monotherapy for up to two years.
For patients with previously untreated FL, administer GAZYVA with one of the following chemotherapy regimens:
- Six 28-day cycles in combination with bendamustine
- Six 21-day cycles in combination with CHOP, followed by 2 additional 21-day cycles of GAZYVA alone
- Eight 21-day cycles in combination with CVP
Patients with previously untreated FL who achieve a complete response or partial response to the initial 6 or 8 cycles should continue on GAZYVA 1,000 mg as monotherapy for up to two years.
GAZYVA should be administered at the standard infusion rate in Cycle 1 (see Table 2). In patients with FL who do not experience a Grade 3 or higher IRR during Cycle 1, GAZYVA may be administered as a shorter, approximately 90-minute infusion from Cycle 2 onwards (see Table 3) with continued premedication.
| Day of treatment cycle | Dose of GAZYVA | Rate of infusion | |
|---|---|---|---|
|
Cycle 1 (loading doses) |
Day 1 | 1,000 mg | Administer at 50 mg/hr. The rate of the infusion can be escalated in 50 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. |
| Day 8 | 1,000 mg | If no infusion-related reaction or an infusion-related reaction of Grade 1 occurred during the previous infusion and the final infusion rate was 100 mg/hr or faster, infusions can be started at a rate of 100 mg/hr and increased by 100 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. If an infusion-related reaction of Grade 2 or higher occurred during the previous infusion, administer at 50 mg/hr. The rate of infusion can be escalated in increments of 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. |
|
| Day 15 | 1,000 mg | ||
| Cycles 2–6 or 2–8 | Day 1 | 1,000 mg | |
| Monotherapy | Every two months for up to two years | 1,000 mg |
| Day of treatment cycle | Dose of GAZYVA | Rate of infusion | |
|---|---|---|---|
| Cycle 1 | Days 1, 8, 15 | 1,000 mg | See Table 2 |
|
Cycles 2–6 Consider an approximately 90-minute infusion in patients with FL who do not experience a Grade 3 or higher infusion-related reaction to GAZYVA in Cycle 1 and subsequent cycles. or 2-8
|
Day 1 | 1,000 mg | If no Grade 3 or higher IRR occurred during Cycle 1: 100 mg/hr for 30 minutes, then 900 mg/hr for approximately 60 minutes. If an IRR of Grade 1-2 with ongoing symptoms or a Grade 3 or higher IRR occurred during the previous approximately 90-minute infusion, administer all subsequent GAZYVA infusions at the standard infusion rate (see Table 2). |
| Monotherapy | Every two months for up to two years | 1,000 mg |
If a planned dose of GAZYVA is missed, administer the missed dose as soon as possible. During GAZYVA and chemotherapy treatment, adjust the dosing schedule accordingly to maintain the time interval between chemotherapy cycles. During monotherapy, maintain the original dosing schedule for subsequent doses. Initiate monotherapy approximately two months after the last dose of GAZYVA administered during the induction phase.
5.2 Progressive Multifocal Leukoencephalopathy
John Cunningham (JC) virus infection resulting in progressive multifocal leukoencephalopathy (PML), which can be fatal, occurred in patients treated with GAZYVA for CLL and NHL. Consider the diagnosis of PML in any patient presenting with new onset or changes to preexisting neurologic manifestations. Evaluation of PML includes, but is not limited to, consultation with a neurologist, brain MRI, and lumbar puncture. Discontinue GAZYVA therapy and consider discontinuation or reduction of any concomitant chemotherapy or immunosuppressive therapy in patients who develop PML.
5.9 Disseminated Intravascular Coagulation (dic) (5.9 Disseminated Intravascular Coagulation (DIC))
Fatal and severe DIC has been reported in patients receiving GAZYVA for treatment of CLL and NHL. The majority of DIC cases have involved changes in platelets and laboratory coagulation parameters following the first infusion, with spontaneous resolution usually occurring by Day 8. In some cases, DIC was associated with IRRs, TLS, or both [see Adverse Reactions (6.1)].
In patients with suspected DIC, evaluate potential causes, and monitor coagulation parameters, platelet counts, and for signs and symptoms of bleeding or thrombosis. Manage according to standard guidelines for DIC. Supportive care, including transfusion of blood products and other medical management, may be necessary.
2.4 Recommended Dosage for Active Lupus Nephritis
Each recommended dose of GAZYVA is 1,000 mg administered intravenously according to Table 4.
| Dose number | Timing of treatment | Dose of GAZYVA | Rate of infusion |
|---|---|---|---|
| 1 | Initial infusion | 1,000 mg | Administer at a rate of 50 mg/hr. The rate of infusion can be escalated in 50 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. For management of IRRs that occur during infusion, see Dosage Modifications for Adverse Reactions (2.6) . |
| 2 | Week 2 (two weeks after Dose 1) |
1,000 mg | Administer at a rate of 100 mg/hr. The rate of infusion can be escalated at a rate of 100 mg/hr every 30 minutes to a maximum of 400 mg/hr. |
| 3 | Week 24 | 1,000 mg | |
| 4 | Week 26 (two weeks after Dose 3) |
1,000 mg | |
|
5
Dose 5 should be administered six months after Dose 4 and thereafter
|
Every 6 months | 1,000 mg |
Patients who do not experience Grade ≥ 3 infusion related reactions during the previous infusion may receive GAZYVA over approximately 90 minutes from Dose 2 onwards (see Table 5), with continued premedication.
| Dose number | Rate of infusion |
|---|---|
| 1 | See Table 4 |
|
2 and thereafter (if no Grade 3 or higher IRR during previous infusion) |
100 mg/hr for 30 minutes, then 900 mg/hr for approximately 60 minutes. If an IRR of Grade 1-2 with ongoing symptoms or a Grade 3 or higher IRR occurs during the previous approximately 90-minute infusion, administer GAZYVA at the standard infusion rate (see Table 4). |
If a planned dose of GAZYVA is missed, it should be administered as soon as possible – do not wait until the next planned dose. The schedule of administration should be adjusted to maintain the appropriate interval between doses.
2.2 Recommended Dosage for Chronic Lymphocytic Leukemia
Each dose of GAZYVA is 1,000 mg administered intravenously with the exception of the first infusions in Cycle 1, which are administered on day 1 (100 mg) and day 2 (900 mg) according to Table 1.
| Day of treatment cycle | Dose of GAZYVA | Rate of infusion | |
|---|---|---|---|
|
Cycle 1 (loading doses) |
Day 1 | 100 mg | Administer at 25 mg/hr over 4 hours. Do not increase the infusion rate. |
| Day 2 | 900 mg | If no infusion-related reaction (IRR) occurred during the previous infusion, administer at 50 mg/hr. The rate of the infusion can be escalated in increments of 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. If an IRR occurred during the previous infusion, administer at 25 mg/hr. The rate of infusion can be escalated in increments of up to 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. |
|
| Day 8 | 1,000 mg | If no IRR occurred during the previous infusion and the final infusion rate was 100 mg/hr or faster, infusions can be started at a rate of 100 mg/hr and increased by 100 mg/hr increments every 30 minutes to a maximum of 400 mg/hr. If an infusion-related reaction occurred during the previous infusion, administer at 50 mg/hr. The rate of infusion can be escalated in increments of 50 mg/hr every 30 minutes to a maximum rate of 400 mg/hr. |
|
| Day 15 | 1,000 mg | ||
| Cycles 2–6 | Day 1 | 1,000 mg |
If a planned dose of GAZYVA is missed, administer the missed dose as soon as possible and adjust dosing schedule to maintain the time interval between doses. If appropriate, patients who do not complete the Day 1 Cycle 1 dose may proceed to the Day 2 Cycle 1 dose.
5.4 Hypersensitivity Reactions Including Serum Sickness
Hypersensitivity reactions have been reported in patients treated with GAZYVA. Signs of immediate-onset hypersensitivity included dyspnea, bronchospasm, hypotension, urticaria and tachycardia. Late-onset hypersensitivity diagnosed as serum sickness has also been reported, with symptoms that include chest pain, diffuse arthralgia and fever. Hypersensitivity reactions may be difficult to clinically distinguish from IRRs. However, hypersensitivity very rarely occurs with the first infusion and, when observed, often occurs after previous exposure.
If a hypersensitivity reaction is suspected during or after an infusion, stop the infusion and permanently discontinue treatment. GAZYVA is contraindicated in patients with known hypersensitivity reactions to GAZYVA, including serum sickness with prior GAZYVA use [see Contraindications (4)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity or genotoxicity studies have been conducted with obinutuzumab.
No specific studies have been conducted to evaluate potential effects on fertility; however, no adverse effects on male or female reproductive organs were observed in the 26-week repeat-dose toxicity study in cynomolgus monkeys.
Warning: Hepatitis B Virus Reactivation and Progressive Multifocal Leukoencephalopathy (WARNING: HEPATITIS B VIRUS REACTIVATION and PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY)
- Hepatitis B Virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, can occur in patients receiving CD20-directed cytolytic antibodies, including GAZYVA. Screen all patients for HBV infection before treatment initiation. Monitor HBV-positive patients during and after treatment with GAZYVA. Discontinue GAZYVA and concomitant medications in the event of HBV reactivation [see Warnings and Precautions (5.1)].
- Progressive Multifocal Leukoencephalopathy (PML) including fatal PML, can occur in patients receiving GAZYVA [see Warnings and Precautions (5.2)].
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:38:49.419185 · Updated: 2026-03-14T22:40:41.023270