Linagliptin Tablets
cbdbd4b2-c07b-00e1-e053-2995a90a5fc9
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Linagliptin is a dipeptidyl peptidase-4 (DPP-4) inhibitor indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus ( 1 ) Limitations of Use Should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis ( 1 ) Has not been studied in patients with a history of pancreatitis ( 1 )
Dosage and Administration
The recommended dose of linagliptin is 5 mg once daily (2.1) Linagliptin can be taken with or without food (2.1)
Contraindications
Linagliptin is contraindicated in patients with a history of a hypersensitivity reaction to linagliptin, such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial Linagliptin is contraindicated in patients with hypersensitivity to linagliptin or any of the excipients in linagliptin tablets, reactions such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial hyperreactivity have occurred [see Warnings and Precautions (5.4) and Adverse Reactions (6) ] .
Warnings and Precautions
Pancreatitis: There have been reports of acute pancreatitis, including fatal pancreatitis. If pancreatitis is suspected, promptly discontinue linagliptin. (5.1) Heart failure: Heart failure has been observed with two other members of the DPP-4 inhibitor class. Consider risks and benefits of linagliptin in patients who have known risk factors for heart failure. Monitor for signs and symptoms. (5.2) Hypoglycemia: When used with an insulin secretagogue (e.g., sulfonylurea (SU)) or insulin, consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemia (5.3) Hypersensitivity reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema, and exfoliative skin conditions) have occurred with linagliptin. If hypersensitivity reactions occur, discontinue linagliptin, treat promptly, and monitor until signs and symptoms resolve. (5.4) Arthralgia: Severe and disabling arthralgia has been reported in patients taking DPP-4 inhibitors. Consider as a possible cause for severe joint pain and discontinue drug if appropriate. (5.5) Bullous pemphigoid: There have been reports of bullous pemphigoid requiring hospitalization. Tell patients to report development of blisters or erosions. If bullous pemphigoid is suspected, discontinue linagliptin (5.6) .
Adverse Reactions
The following serious adverse reactions are described below or elsewhere in the prescribing information: Pancreatitis [see Warnings and Precautions (5.1) ] Heart Failure [see Warnings and Precautions (5.2) ] Use with Medications Known to Cause Hypoglycemia [see Warnings and Precautions (5.3) ] Hypersensitivity Reactions [see Warnings and Precautions (5.4) ] Severe and Disabling Arthralgia [see Warnings and Precautions (5.5) ] Bullous Pemphigoid [see Warnings and Precautions (5.6) ]
Drug Interactions
Strong P-glycoprotein/CYP3A4 inducer: The efficacy of linagliptin may be reduced when administered in combination (e.g., with rifampin). Use of alternative treatments is strongly recommended. (7.1)
How Supplied
Linagliptin tablets are available as white or off-white, round, biconvex, film-coated tablets containing 5 mg of linagliptin. Linagliptin tablets are debossed with “S75” on one side and blank on the other side. They are supplied as follows: Bottles of 30 (NDC 48792-7865-1) If repackaging is required, dispense in a tight container as defined in USP.
Storage and Handling
Linagliptin tablets are available as white or off-white, round, biconvex, film-coated tablets containing 5 mg of linagliptin. Linagliptin tablets are debossed with “S75” on one side and blank on the other side. They are supplied as follows: Bottles of 30 (NDC 48792-7865-1) If repackaging is required, dispense in a tight container as defined in USP.
Description
Warnings and Precautions Pancreatitis ( 5.1 ) 7/2019 Bullous Pemphigoid ( 5.6 ) 7/2019 Macrovascular Outcomes- Removed 7/2019
Medication Information
Warnings and Precautions
Pancreatitis: There have been reports of acute pancreatitis, including fatal pancreatitis. If pancreatitis is suspected, promptly discontinue linagliptin. (5.1) Heart failure: Heart failure has been observed with two other members of the DPP-4 inhibitor class. Consider risks and benefits of linagliptin in patients who have known risk factors for heart failure. Monitor for signs and symptoms. (5.2) Hypoglycemia: When used with an insulin secretagogue (e.g., sulfonylurea (SU)) or insulin, consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemia (5.3) Hypersensitivity reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema, and exfoliative skin conditions) have occurred with linagliptin. If hypersensitivity reactions occur, discontinue linagliptin, treat promptly, and monitor until signs and symptoms resolve. (5.4) Arthralgia: Severe and disabling arthralgia has been reported in patients taking DPP-4 inhibitors. Consider as a possible cause for severe joint pain and discontinue drug if appropriate. (5.5) Bullous pemphigoid: There have been reports of bullous pemphigoid requiring hospitalization. Tell patients to report development of blisters or erosions. If bullous pemphigoid is suspected, discontinue linagliptin (5.6) .
Indications and Usage
Linagliptin is a dipeptidyl peptidase-4 (DPP-4) inhibitor indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus ( 1 ) Limitations of Use Should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis ( 1 ) Has not been studied in patients with a history of pancreatitis ( 1 )
Dosage and Administration
The recommended dose of linagliptin is 5 mg once daily (2.1) Linagliptin can be taken with or without food (2.1)
Contraindications
Linagliptin is contraindicated in patients with a history of a hypersensitivity reaction to linagliptin, such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial Linagliptin is contraindicated in patients with hypersensitivity to linagliptin or any of the excipients in linagliptin tablets, reactions such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial hyperreactivity have occurred [see Warnings and Precautions (5.4) and Adverse Reactions (6) ] .
Adverse Reactions
The following serious adverse reactions are described below or elsewhere in the prescribing information: Pancreatitis [see Warnings and Precautions (5.1) ] Heart Failure [see Warnings and Precautions (5.2) ] Use with Medications Known to Cause Hypoglycemia [see Warnings and Precautions (5.3) ] Hypersensitivity Reactions [see Warnings and Precautions (5.4) ] Severe and Disabling Arthralgia [see Warnings and Precautions (5.5) ] Bullous Pemphigoid [see Warnings and Precautions (5.6) ]
Drug Interactions
Strong P-glycoprotein/CYP3A4 inducer: The efficacy of linagliptin may be reduced when administered in combination (e.g., with rifampin). Use of alternative treatments is strongly recommended. (7.1)
Storage and Handling
Linagliptin tablets are available as white or off-white, round, biconvex, film-coated tablets containing 5 mg of linagliptin. Linagliptin tablets are debossed with “S75” on one side and blank on the other side. They are supplied as follows: Bottles of 30 (NDC 48792-7865-1) If repackaging is required, dispense in a tight container as defined in USP.
How Supplied
Linagliptin tablets are available as white or off-white, round, biconvex, film-coated tablets containing 5 mg of linagliptin. Linagliptin tablets are debossed with “S75” on one side and blank on the other side. They are supplied as follows: Bottles of 30 (NDC 48792-7865-1) If repackaging is required, dispense in a tight container as defined in USP.
Description
Warnings and Precautions Pancreatitis ( 5.1 ) 7/2019 Bullous Pemphigoid ( 5.6 ) 7/2019 Macrovascular Outcomes- Removed 7/2019
Race
No dose adjustment is necessary based on race. Race had no clinically meaningful effect on the pharmacokinetics of linagliptin based on available pharmacokinetic data, including subjects of White, Hispanic, Black, and Asian racial groups.
Gender
No dose adjustment is necessary based on gender. Gender had no clinically meaningful effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis.
Section 42229-5
Linagliptin tablet is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus [see Clinical Studies (14.1)] .
Section 42231-1
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: 6/2020 | |||
|
MEDICATION GUIDE
Linagliptin (LIN-a-GLIP-tin) Tablets for oral use |
||||
| Read this Medication Guide carefully before you start taking linagliptin tablets and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or your treatment. If you have any questions about linagliptin tablets, ask your doctor or pharmacist. | ||||
|
What is the most important information I should know about linagliptin tablets?
Linagliptin can cause serious side effects, including :
|
||||
|
|
|||
|
||||
What is linagliptin tablet?
|
||||
|
Who should not take linagliptin tablets?
Do not take linagliptin tablets if you:
|
||||
|
What should I tell my doctor before taking linagliptin tablets?
Before taking linagliptin tablets, tell your doctor about all of your medical conditions, including if you:
linagliptin tablets may affect the way other medicines work, and other medicines may affect how linagliptin tablets work. Especially tell your doctor if you take:
|
||||
How should I take linagliptin tablets?
|
||||
|
What are the possible side effects of linagliptin tablets?
linagliptin tablets may cause serious side effects, including:
|
||||
|
|
|
|
|
|
||||
|
|
|||
Tell your doctor if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of linagliptin tablets. For more information, ask your doctor or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
||||
How should I store linagliptin tablets?
|
||||
|
General information about the safe and effective use of linagliptin tablets.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use linagliptin tablets for a condition for which it was not prescribed. Do not give linagliptin tablets to other people, even if they have the same symptoms you have. It may harm them. You can ask your pharmacist or doctor for information about linagliptin tablets that is written for health professionals. |
||||
|
What are the ingredients in linagliptin tablets?
Active Ingredient: linagliptin Inactive Ingredients: mannitol, pregelatinized starch, copovidone, and magnesium stearate. The film coating contains the following inactive ingredients: hypromellose, titanium dioxide, and polyethylene glycol. |
||||
|
Manufactured by:
Sunshine Lake Pharma Co., Ltd. Northern Industry Road 1#, Song Shan Lake, DongGuan, GuangDong Province, 523808, P.R. China Manufactured for: HEC Pharm USA Inc. 13200 Townsend Road, Philadelphia, PA 19154 The brands listed are trademarks of their respective owners and are not trademarks of HEC Pharm Co., Ltd. The makers of these brands are not affiliated with and do not endorse HEC Pharm Co., Ltd., or its products. |
Section 43683-2
Section 51945-4
Linagliptin tablets
5 mg
30 tablets
NDC 48792-7865-1
In Vivo
Strong inducers of CYP3A4 or P-gp (e.g., rifampin) decrease exposure to linagliptin to subtherapeutic and likely ineffective concentrations [see Drug Interactions (7)] . In vivo studies indicated evidence of a low propensity for causing drug interactions with substrates of CYP3A4, CYP2C9, CYP2C8, P-gp and organic cationic transporter (OCT).
In Vitro
Linagliptin is a weak to moderate inhibitor of CYP isozyme CYP3A4, but does not inhibit other CYP isozymes and is not an inducer of CYP isozymes, including CYP1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, and 4A11.
Linagliptin is a P-glycoprotein (P-gp) substrate, and inhibits P-gp mediated transport of digoxin at high concentrations. Based on these results and in vivo drug interaction studies, linagliptin is considered unlikely to cause interactions with other P-gp substrates at therapeutic concentrations.
Geriatric
Age did not have a clinically meaningful impact on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis.
Pediatric
Studies characterizing the pharmacokinetics of linagliptin in pediatric patients have not yet been performed.
Absorption
The absolute bioavailability of linagliptin is approximately 30%. A high-fat meal reduced C max by 15% and increased AUC by 4%; this effect is not clinically relevant. Linagliptin may be administered with or without food.
Distribution
The mean apparent volume of distribution at steady state following a single intravenous dose of linagliptin 5 mg to healthy subjects is approximately 1110 L, indicating that linagliptin extensively distributes to the tissues. Plasma protein binding of linagliptin is concentration-dependent, decreasing from about 99% at 1 nmol/L to 75%-89% at ≥30 nmol/L, reflecting saturation of binding to DPP-4 with increasing concentration of linagliptin. At high concentrations, where DPP-4 is fully saturated, 70% to 80% of linagliptin remains bound to plasma proteins and 20% to 30% is unbound in plasma. Plasma binding is not altered in patients with renal or hepatic impairment.
Laboratory Tests
Changes in laboratory findings were similar in patients treated with linagliptin 5 mg compared to patients treated with placebo.
Increase in Uric Acid: Changes in laboratory values that occurred more frequently in the linagliptin group and >1% more than in the placebo group were increases in uric acid (1.3% in the placebo group, 2.7% in the linagliptin group).
Increase in Lipase: In a placebo-controlled clinical trial with linagliptin in type 2 diabetes mellitus patients with micro- or macroalbuminuria, a mean increase of 30% in lipase concentrations from baseline to 24 weeks was observed in the linagliptin arm compared to a mean decrease of 2% in the placebo arm. Lipase levels above 3 times upper limit of normal were seen in 8.2% compared to 1.7% patients in the linagliptin and placebo arms, respectively.
The clinical significance of elevations in lipase with linagliptin is unknown in the absence of potential signs and symptoms of pancreatitis [see Warnings and Precautions (5.1)].
Vital
Signs
No clinically meaningful changes in vital signs were
observed in patients treated with linagliptin.
Renal Impairment
An open-label pharmacokinetic study evaluated the pharmacokinetics of linagliptin 5 mg in male and female patients with varying degrees of chronic renal impairment. The study included 6 healthy subjects with normal renal function (creatinine clearance [CrCl] ≥80 mL/min), 6 patients with mild renal impairment (CrCl 50 to <80 mL/min), 6 patients with moderate renal impairment (CrCl 30 to <50 mL/min), 10 patients with type 2 diabetes mellitus and severe renal impairment (CrCl <30 mL/min), and 11 patients with type 2 diabetes mellitus and normal renal function. Creatinine clearance was measured by 24-hour urinary creatinine clearance measurements or estimated from serum creatinine based on the Cockcroft-Gault formula.
Under steady-state conditions, linagliptin exposure in patients with mild renal impairment was comparable to healthy subjects.
In patients with moderate renal impairment under steady-state conditions, mean exposure of linagliptin increased (AUC τ,ss by 71% and C max by 46%) compared with healthy subjects. This increase was not associated with a prolonged accumulation half-life, terminal half-life, or an increased accumulation factor. Renal excretion of linagliptin was below 5% of the administered dose and was not affected by decreased renal function.
Patients with type 2 diabetes mellitus and severe renal impairment showed steady-state exposure approximately 40% higher than that of patients with type 2 diabetes mellitus and normal renal function (increase in AUC τ,ss by 42% and C max by 35%). For both type 2 diabetes mellitus groups, renal excretion was below 7% of the administered dose.
These findings were further supported by the results of population pharmacokinetic analyses.
10 overdosage
In the event of an overdose with linagliptin, contact the Poison Control Center. Removal of linagliptin by hemodialysis or peritoneal dialysis is unlikely.
Hepatic Impairment
In patients with mild hepatic impairment (Child-Pugh class A), steady-state exposure (AUC τ,ss) of linagliptin was approximately 25% lower and C max,ss was approximately 36% lower than in healthy subjects. In patients with moderate hepatic impairment (Child-Pugh class B), AUC ss of linagliptin was about 14% lower and C max,ss was approximately 8% lower than in healthy subjects. Patients with severe hepatic impairment (Child-Pugh class C) had comparable exposure of linagliptin in terms of AUC 0-24 and approximately 23% lower C max compared with healthy subjects. Reductions in the pharmacokinetic parameters seen in patients with hepatic impairment did not result in reductions in DPP-4 inhibition.
11 description
Linagliptin tablets contain, as the active ingredient, an orally-active inhibitor of the dipeptidyl peptidase-4 (DPP-4) enzyme.
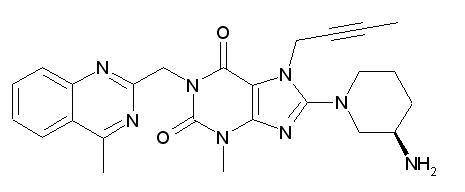
Linagliptin is described chemically as 1H-Purine-2,6-dione, 8-[(3R)-3-amino-1-piperidinyl]-7-(2-butyn-1-yl)-3,7-dihydro-3-methyl-1-[(4-methyl-2-quinazolinyl)methyl]-
The empirical formula is C 25H 28N 8O 2 and the molecular weight is 472.54 g/mol. The structural formula is:
Linagliptin is a white to yellowish, not or only slightly hygroscopic solid substance. It is very slightly soluble in water (0.9 mg/mL). Linagliptin is soluble in methanol (ca. 60 mg/mL), sparingly soluble in ethanol (ca. 10 mg/mL), very slightly soluble in isopropanol (<1 mg/mL), and very slightly soluble in acetone (ca. 1 mg/mL).
Each film-coated tablet of linagliptin contains 5 mg of linagliptin free base and the following inactive ingredients: mannitol, pregelatinized starch, copovidone, and magnesium stearate. In addition, the film coating contains the following inactive ingredients: hypromellose, titanium dioxide and polyethylene glycol.
5.1 pancreatitis
Acute pancreatitis, including fatal pancreatitis, has been reported in patients treated with linagliptin.
Take careful notice of potential signs and symptoms of pancreatitis. If pancreatitis is suspected, promptly discontinue linagliptin and initiate appropriate management. It is unknown whether patients with a history of pancreatitis are at increased risk for the development of pancreatitis while using linagliptin.
5.2 heart Failure
An association between DPP-4 inhibitor treatment and heart failure has been observed in cardiovascular outcomes trials for two other members of the DPP-4 inhibitor class. These trials evaluated patients with type 2 diabetes mellitus and atherosclerotic cardiovascular disease.
Consider the risks and benefits of linagliptin prior to initiating treatment in patients at risk for heart failure, such as those with a prior history of heart failure and a history of renal impairment, and observe these patients for signs and symptoms of heart failure during therapy. Advise patients of the characteristic symptoms of heart failure and to immediately report such symptoms. If heart failure develops, evaluate and manage according to current standards of care and consider discontinuation of linagliptin.
8.4 pediatric Use
Safety and effectiveness of linagliptin in pediatric patients under 18 years of age have not been established.
8.5 geriatric Use
In the 15 type 2 diabetes studies with linagliptin, 1085 linagliptin-treated patients were 65 years of age and older (including 131 linagliptin-treated patients 75 years of age and older). Of these 15 studies, 12 were double-blind placebo-controlled. In these 12 studies, 591 linagliptin-treated patients were 65 years of age and older (including 82 linagliptin-treated patients 75 years of age and older). In these linagliptin studies, no overall differences in safety or effectiveness of linagliptin were observed between geriatric patients and younger adult patients.
4 contraindications
Linagliptin is contraindicated in patients with a history of a hypersensitivity reaction to linagliptin, such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial Linagliptin is contraindicated in patients with hypersensitivity to linagliptin or any of the excipients in linagliptin tablets, reactions such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial hyperreactivity have occurred [see Warnings and Precautions (5.4) and Adverse Reactions (6)] .
6 adverse Reactions
The following serious adverse reactions are described below or elsewhere in the prescribing information:
- Pancreatitis [see Warnings and Precautions (5.1)]
- Heart Failure [see Warnings and Precautions (5.2)]
- Use with Medications Known to Cause Hypoglycemia [see Warnings and Precautions (5.3)]
- Hypersensitivity Reactions [see Warnings and Precautions (5.4)]
- Severe and Disabling Arthralgia [see Warnings and Precautions (5.5)]
- Bullous Pemphigoid [see Warnings and Precautions (5.6)]
7 drug Interactions
Strong P-glycoprotein/CYP3A4 inducer: The efficacy of linagliptin may be reduced when administered in combination (e.g., with rifampin). Use of alternative treatments is strongly recommended. (7.1)
8.6 renal Impairment
No dose adjustment is recommended for patients with renal impairment [see Clinical Pharmacology (12.3)] .
Cardiac Electrophysiology
In a randomized, placebo-controlled, active-comparator, 4-way crossover study, 36 healthy subjects were administered a single oral dose of linagliptin 5 mg, linagliptin 100 mg (20 times the recommended dose), moxifloxacin, and placebo. No increase in QTc was observed with either the recommended dose of 5 mg or the 100-mg dose. At the 100-mg dose, peak linagliptin plasma concentrations were approximately 38-fold higher than the peak concentrations following a 5-mg dose.
12.2 pharmacodynamics
Linagliptin binds to DPP-4 in a reversible manner and thus increases the concentrations of incretin hormones. Linagliptin glucose dependently increases insulin secretion and lowers glucagon secretion, thus resulting in better regulation of glucose homeostasis. Linagliptin binds selectively to DPP-4, and selectively inhibits DPP-4 but not DPP-8 or DPP-9 activity in vitro at concentrations approximating therapeutic exposures.
12.3 pharmacokinetics
The pharmacokinetics of linagliptin has been characterized in healthy subjects and patients with type 2 diabetes. After oral administration of a single 5-mg dose to healthy subjects, peak plasma concentrations of linagliptin occurred at approximately 1.5 hours post dose (T max); the mean plasma area under the curve (AUC) was 139 nmol*h/L and maximum concentration (C max) was 8.9 nmol/L.
Plasma concentrations of linagliptin decline in at least a biphasic manner with a long terminal half-life (>100 hours), related to the saturable binding of linagliptin to DPP-4. The prolonged elimination phase does not contribute to the accumulation of the drug. The effective half-life for accumulation of linagliptin, as determined from oral administration of multiple doses of linagliptin 5 mg, is approximately 12 hours. After once-daily dosing, steady-state plasma concentrations of linagliptin 5 mg are reached by the third dose, and C max and AUC increased by a factor of 1.3 at steady-state compared with the first dose. The intra-subject and inter-subject coefficients of variation for linagliptin AUC were small (12.6% and 28.5%, respectively). Plasma AUC of linagliptin increased in a less than dose-proportional manner in the dose range of 1 to 10 mg. The pharmacokinetics of linagliptin is similar in healthy subjects and in patients with type 2 diabetes.
2.1 recommended Dosing
The recommended dose of linagliptin is 5 mg once daily.
Linagliptin tablets can be taken with or without food.
5.6 bullous Pemphigoid
Postmarketing cases of bullous pemphigoid requiring hospitalization have been reported with DPP-4 inhibitor use. In reported cases, patients typically recovered with topical or systemic immunosuppressive treatment and discontinuation of the DPP-4 inhibitor. Tell patients to report development of blisters or erosions while receiving linagliptin. If bullous pemphigoid is suspected, linagliptin should be discontinued and referral to a dermatologist should be considered for diagnosis and appropriate treatment.
8.7 hepatic Impairment
No dose adjustment is recommended for patients with hepatic impairment [see Clinical Pharmacology (12.3)] .
1 indications and Usage
Linagliptin is a dipeptidyl peptidase-4 (DPP-4) inhibitor indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus ( 1)
Limitations of Use
Body Mass Index (bmi)/weight
No dose adjustment is necessary based on BMI/weight. BMI/weight had no clinically meaningful effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis.
12.1 mechanism of Action
Linagliptin is an inhibitor of DPP-4, an enzyme that degrades the incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). Thus, linagliptin increases the concentrations of active incretin hormones, stimulating the release of insulin in a glucose-dependent manner and decreasing the levels of glucagon in the circulation. Both incretin hormones are involved in the physiological regulation of glucose homeostasis. Incretin hormones are secreted at a low basal level throughout the day and levels rise immediately after meal intake. GLP-1 and GIP increase insulin biosynthesis and secretion from pancreatic beta cells in the presence of normal and elevated blood glucose levels. Furthermore, GLP-1 also reduces glucagon secretion from pancreatic alpha-cells, resulting in a reduction in hepatic glucose output.
5 warnings and Precautions
- Pancreatitis: There have been reports of acute pancreatitis, including fatal pancreatitis. If pancreatitis is suspected, promptly discontinue linagliptin. (5.1)
- Heart failure: Heart failure has been observed with two other members of the DPP-4 inhibitor class. Consider risks and benefits of linagliptin in patients who have known risk factors for heart failure. Monitor for signs and symptoms. (5.2)
- Hypoglycemia: When used with an insulin secretagogue (e.g., sulfonylurea (SU)) or insulin, consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemia (5.3)
- Hypersensitivity reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema, and exfoliative skin conditions) have occurred with linagliptin. If hypersensitivity reactions occur, discontinue linagliptin, treat promptly, and monitor until signs and symptoms resolve. (5.4)
- Arthralgia: Severe and disabling arthralgia has been reported in patients taking DPP-4 inhibitors. Consider as a possible cause for severe joint pain and discontinue drug if appropriate. (5.5)
- Bullous pemphigoid: There have been reports of bullous pemphigoid requiring hospitalization. Tell patients to report development of blisters or erosions. If bullous pemphigoid is suspected, discontinue linagliptin (5.6).
2 dosage and Administration
14.1 glycemic Control Trials
Linagliptin has been studied as monotherapy and in combination with metformin, sulfonylurea, pioglitazone, and insulin. Linagliptin has also been studied in patients with type 2 diabetes and severe chronic renal impairment.
In patients with type 2 diabetes, treatment with linagliptin produced clinically significant improvements in hemoglobin A1c (A1C), fasting plasma glucose (FPG), and 2-hour post-prandial glucose (PPG) compared with placebo.
3 dosage Forms and Strengths
Linagliptin 5 mg tablets are white or off-white, round, biconvex, film-coated tablets with “S75” debossed on one side and blank on the other side.
6.2 postmarketing Experience
Additional adverse reactions have been identified during postapproval use of linagliptin. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Acute pancreatitis, including fatal pancreatitis [see Indications and Usage (1)]
- Hypersensitivity reactions including anaphylaxis, angioedema, and exfoliative skin conditions
- Severe and disabling arthralgia
- Bullous pemphigoid
- Rash
- Mouth ulceration, stomatitis
- Rhabdomyolysis
5.4 hypersensitivity Reactions
There have been postmarketing reports of serious hypersensitivity reactions in patients treated with linagliptin. These reactions include anaphylaxis, angioedema, and exfoliative skin conditions. Onset of these reactions predominantly occurred within the first 3 months after initiation of treatment with linagliptin, with some reports occurring after the first dose. If a serious hypersensitivity reaction is suspected, discontinue linagliptin, assess for other potential causes for the event, and institute alternative treatment for diabetes.
Angioedema has also been reported with other dipeptidyl peptidase-4 (DPP-4) inhibitors. Use caution in a patient with a history of angioedema to another DPP-4 inhibitor because it is unknown whether such patients will be predisposed to angioedema with linagliptin.
6.1 clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety evaluation of linagliptin 5 mg once daily in patients with type 2 diabetes is based on 14 placebo-controlled trials, 1 active-controlled study, and one study in patients with severe renal impairment. In the 14 placebo-controlled studies, a total of 3625 patients were randomized and treated with linagliptin 5 mg daily and 2176 with placebo. The mean exposure in patients treated with linagliptin across studies was 29.6 weeks. The maximum follow-up was 78 weeks.
Linagliptin 5 mg once daily was studied as monotherapy in three placebo-controlled trials of 18 and 24 weeks’ duration and in five additional placebo-controlled studies lasting ≤18 weeks. The use of linagliptin in combination with other antihyperglycemic agents was studied in six placebo-controlled trials: two with metformin (12 and 24 weeks’ treatment duration); one with a sulfonylurea (18 weeks’ treatment duration); one with metformin and sulfonylurea (24 weeks’ treatment duration); one with pioglitazone (24 weeks’ treatment duration); and one with insulin (primary endpoint at 24 weeks).
In a pooled dataset of 14 placebo-controlled clinical trials, adverse reactions that occurred in ≥2% of patients receiving linagliptin (n = 3625) and more commonly than in patients given placebo (n = 2176), are shown in Table 1. The overall incidence of adverse events with linagliptin were similar to placebo.
| Number (%) of Patients | ||
|
Linagliptin
5 mg
n = 3625 |
Placebo
n = 2176 |
|
| Nasopharyngitis | 254 (7.0) | 132 (6.1) |
| Diarrhea | 119 (3.3) | 65 (3.0) |
| Cough | 76 (2.1) | 30 (1.4) |
Rates for other adverse reactions for linagliptin 5 mg vs placebo when linagliptin was used in combination with specific anti-diabetic agents were: urinary tract infection (3.1% vs 0%) and hypertriglyceridemia (2.4% vs 0%) when linagliptin was used as add-on to sulfonylurea; hyperlipidemia (2.7% vs 0.8%) and weight increased (2.3% vs 0.8%) when linagliptin was used as add-on to pioglitazone; and constipation (2.1% vs 1%) when linagliptin was used as add-on to basal insulin therapy. Other adverse reactions reported in clinical studies with treatment of linagliptin were hypersensitivity (e.g., urticaria, angioedema, localized skin exfoliation, or bronchial hyperreactivity) and myalgia.
Following 104 weeks’ treatment in a controlled study comparing linagliptin with glimepiride in which all patients were also receiving metformin, adverse reactions reported in ≥5% of patients treated with linagliptin (n = 776) and more frequently than in patients treated with a sulfonylurea (n = 775) were back pain (9.1% vs 8.4%), arthralgia (8.1% vs 6.1%), upper respiratory tract infection (8.0% vs 7.6%), headache (6.4% vs 5.2%), cough (6.1% vs 4.9%), and pain in extremity (5.3% vs 3.9%).
In the clinical trial program, pancreatitis was reported in 15.2 cases per 10,000 patient year exposure while being treated with linagliptin compared with 3.7 cases per 10,000 patient year exposure while being treated with comparator (placebo and active comparator, sulfonylurea). Three additional cases of pancreatitis were reported following the last administered dose of linagliptin.
17 patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Pancreatitis
Inform patients that acute pancreatitis
has been reported during use of linagliptin. Inform patients
that persistent severe abdominal pain, sometimes radiating to the
back, which may or may not be accompanied by vomiting, is the hallmark
symptom of acute pancreatitis. Instruct patients to discontinue linagliptin
promptly and contact their physician if persistent severe abdominal
pain occurs [
see
Warnings and Precautions (5.1)
].
Heart Failure
Inform patients of the signs and symptoms of heart failure. Before initiating linagliptin, patients should be asked about a history of heart failure or other risk factors for heart failure including moderate to severe renal impairment. Instruct patients to contact their healthcare provider as soon as possible if they experience symptoms of heart failure, including increasing shortness of breath, rapid increase in weight or swelling of the feet [
see
Warnings and Precautions (5.2)
].
Hypoglycemia
Inform patients that the incidence of hypoglycemia
is increased when linagliptin is added to a sulfonylurea or insulin
and that a lower dose of the sulfonylurea or insulin may be required
to reduce the risk of hypoglycemia
[see
Warnings and Precautions (5.3)]
.
Hypersensitivity Reactions
Inform patients that serious allergic reactions, such as anaphylaxis,
angioedema, and exfoliative skin conditions, have been reported during
postmarketing use of linagliptin. If symptoms of allergic reactions
(such as rash, skin flaking or peeling, urticaria, swelling of the
skin, or swelling of the face, lips, tongue, and throat that may cause
difficulty in breathing or swallowing) occur, patients must stop taking
linagliptin and seek medical advice promptly
[see
Warnings and Precautions (5.4)]
.
Severe and Disabling Arthralgia
Inform patients that severe and disabling joint pain
may occur with this class of drugs. The time to onset of symptoms
can range from one day to years. Instruct patients to seek medical
advice if severe joint pain occurs
[see
Warnings and Precautions (5.5)].
Bullous Pemphigoid
Inform patients that bullous pemphigoid has been reported during use of linagliptin. Instruct patients to seek medical advice if blisters
or erosions occur
[see
Warnings and Precautions (5.6)].
Missed Dose
Instruct patients to take linagliptin only as prescribed.
If a dose is missed, advise patients not to double their next dose.
5.5 severe and Disabling Arthralgia
There have been postmarketing reports of severe and disabling arthralgia in patients taking DPP-4 inhibitors. The time to onset of symptoms following initiation of drug therapy varied from one day to years. Patients experienced relief of symptoms upon discontinuation of the medication. A subset of patients experienced a recurrence of symptoms when restarting the same drug or a different DPP-4 inhibitor. Consider DPP-4 inhibitors as a possible cause for severe joint pain and discontinue drug if appropriate.
16 how Supplied/storage and Handling
Linagliptin tablets are available as white or off-white, round, biconvex, film-coated tablets containing 5 mg of linagliptin. Linagliptin tablets are debossed with “S75” on one side and blank on the other side.
They are supplied
as follows:
Bottles of 30 (NDC 48792-7865-1)
If repackaging is required, dispense
in a tight container as defined in USP.
7.2 insulin Secretagogues Or Insulin
Coadministration of linagliptin with an insulin secretagogue (e.g., sulfonylurea) or insulin may require lower doses of the insulin secretagogue or insulin to reduce the risk of hypoglycemia [see Warnings and Precautions (5.3)] .
7.1 inducers of P Glycoprotein Or Cyp3a4 Enzymes
Rifampin decreased linagliptin exposure, suggesting that the efficacy of linagliptin may be reduced when administered in combination with a strong P-gp or CYP3A4 inducer. Therefore, use of alternative treatments is strongly recommended when linagliptin is to be administered with a strong P-gp or CYP3A4 inducer [see Clinical Pharmacology (12.3)] .
5.3 use With Medications Known to Cause Hypoglycemia
Insulin secretagogues and insulin are known to cause hypoglycemia. The use of linagliptin in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin was associated with a higher rate of hypoglycemia compared with placebo in clinical trials [see Adverse Reactions (6.1)] . The use of linagliptin in combination with insulin in subjects with severe renal impairment was associated with a higher rate of hypoglycemia [see Adverse Reactions (6.1)] . Therefore, a lower dose of the insulin secretagogue or insulin may be required to reduce the risk of hypoglycemia when used in combination with linagliptin.
13.1 carcinogenesis, Mutagenesis, Impairment of Fertility
Linagliptin did not increase the incidence of tumors in male and female rats in a 2-year study at doses of 6, 18, and 60 mg/kg. The highest dose of 60 mg/kg is approximately 418 times the clinical dose of 5 mg/day based on AUC exposure. Linagliptin did not increase the incidence of tumors in mice in a 2-year study at doses up to 80 mg/kg (males) and 25 mg/kg (females), or approximately 35 and 270 times the clinical dose based on AUC exposure. Higher doses of linagliptin in female mice (80 mg/kg) increased the incidence of lymphoma at approximately 215 times the clinical dose based on AUC exposure.
Linagliptin was not mutagenic or clastogenic with or without metabolic activation in the Ames bacterial mutagenicity assay, a chromosomal aberration test in human lymphocytes, and an in vivo micronucleus assay.
In fertility studies in rats, linagliptin had no adverse effects on early embryonic development, mating, fertility, or bearing live young up to the highest dose of 240 mg/kg (approximately 943 times the clinical dose based on AUC exposure).
Structured Label Content
Race
No dose adjustment is necessary based on race. Race had no clinically meaningful effect on the pharmacokinetics of linagliptin based on available pharmacokinetic data, including subjects of White, Hispanic, Black, and Asian racial groups.
Gender
No dose adjustment is necessary based on gender. Gender had no clinically meaningful effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis.
Section 42229-5 (42229-5)
Linagliptin tablet is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus [see Clinical Studies (14.1)] .
Section 42231-1 (42231-1)
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: 6/2020 | |||
|
MEDICATION GUIDE
Linagliptin (LIN-a-GLIP-tin) Tablets for oral use |
||||
| Read this Medication Guide carefully before you start taking linagliptin tablets and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or your treatment. If you have any questions about linagliptin tablets, ask your doctor or pharmacist. | ||||
|
What is the most important information I should know about linagliptin tablets?
Linagliptin can cause serious side effects, including :
|
||||
|
|
|||
|
||||
What is linagliptin tablet?
|
||||
|
Who should not take linagliptin tablets?
Do not take linagliptin tablets if you:
|
||||
|
What should I tell my doctor before taking linagliptin tablets?
Before taking linagliptin tablets, tell your doctor about all of your medical conditions, including if you:
linagliptin tablets may affect the way other medicines work, and other medicines may affect how linagliptin tablets work. Especially tell your doctor if you take:
|
||||
How should I take linagliptin tablets?
|
||||
|
What are the possible side effects of linagliptin tablets?
linagliptin tablets may cause serious side effects, including:
|
||||
|
|
|
|
|
|
||||
|
|
|||
Tell your doctor if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of linagliptin tablets. For more information, ask your doctor or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
||||
How should I store linagliptin tablets?
|
||||
|
General information about the safe and effective use of linagliptin tablets.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use linagliptin tablets for a condition for which it was not prescribed. Do not give linagliptin tablets to other people, even if they have the same symptoms you have. It may harm them. You can ask your pharmacist or doctor for information about linagliptin tablets that is written for health professionals. |
||||
|
What are the ingredients in linagliptin tablets?
Active Ingredient: linagliptin Inactive Ingredients: mannitol, pregelatinized starch, copovidone, and magnesium stearate. The film coating contains the following inactive ingredients: hypromellose, titanium dioxide, and polyethylene glycol. |
||||
|
Manufactured by:
Sunshine Lake Pharma Co., Ltd. Northern Industry Road 1#, Song Shan Lake, DongGuan, GuangDong Province, 523808, P.R. China Manufactured for: HEC Pharm USA Inc. 13200 Townsend Road, Philadelphia, PA 19154 The brands listed are trademarks of their respective owners and are not trademarks of HEC Pharm Co., Ltd. The makers of these brands are not affiliated with and do not endorse HEC Pharm Co., Ltd., or its products. |
Section 43683-2 (43683-2)
Section 51945-4 (51945-4)
Linagliptin tablets
5 mg
30 tablets
NDC 48792-7865-1
In Vivo (In vivo)
Strong inducers of CYP3A4 or P-gp (e.g., rifampin) decrease exposure to linagliptin to subtherapeutic and likely ineffective concentrations [see Drug Interactions (7)] . In vivo studies indicated evidence of a low propensity for causing drug interactions with substrates of CYP3A4, CYP2C9, CYP2C8, P-gp and organic cationic transporter (OCT).
In Vitro (In vitro)
Linagliptin is a weak to moderate inhibitor of CYP isozyme CYP3A4, but does not inhibit other CYP isozymes and is not an inducer of CYP isozymes, including CYP1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, and 4A11.
Linagliptin is a P-glycoprotein (P-gp) substrate, and inhibits P-gp mediated transport of digoxin at high concentrations. Based on these results and in vivo drug interaction studies, linagliptin is considered unlikely to cause interactions with other P-gp substrates at therapeutic concentrations.
Geriatric
Age did not have a clinically meaningful impact on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis.
Pediatric
Studies characterizing the pharmacokinetics of linagliptin in pediatric patients have not yet been performed.
Absorption
The absolute bioavailability of linagliptin is approximately 30%. A high-fat meal reduced C max by 15% and increased AUC by 4%; this effect is not clinically relevant. Linagliptin may be administered with or without food.
Distribution
The mean apparent volume of distribution at steady state following a single intravenous dose of linagliptin 5 mg to healthy subjects is approximately 1110 L, indicating that linagliptin extensively distributes to the tissues. Plasma protein binding of linagliptin is concentration-dependent, decreasing from about 99% at 1 nmol/L to 75%-89% at ≥30 nmol/L, reflecting saturation of binding to DPP-4 with increasing concentration of linagliptin. At high concentrations, where DPP-4 is fully saturated, 70% to 80% of linagliptin remains bound to plasma proteins and 20% to 30% is unbound in plasma. Plasma binding is not altered in patients with renal or hepatic impairment.
Laboratory Tests
Changes in laboratory findings were similar in patients treated with linagliptin 5 mg compared to patients treated with placebo.
Increase in Uric Acid: Changes in laboratory values that occurred more frequently in the linagliptin group and >1% more than in the placebo group were increases in uric acid (1.3% in the placebo group, 2.7% in the linagliptin group).
Increase in Lipase: In a placebo-controlled clinical trial with linagliptin in type 2 diabetes mellitus patients with micro- or macroalbuminuria, a mean increase of 30% in lipase concentrations from baseline to 24 weeks was observed in the linagliptin arm compared to a mean decrease of 2% in the placebo arm. Lipase levels above 3 times upper limit of normal were seen in 8.2% compared to 1.7% patients in the linagliptin and placebo arms, respectively.
The clinical significance of elevations in lipase with linagliptin is unknown in the absence of potential signs and symptoms of pancreatitis [see Warnings and Precautions (5.1)].
Vital
Signs
No clinically meaningful changes in vital signs were
observed in patients treated with linagliptin.
Renal Impairment
An open-label pharmacokinetic study evaluated the pharmacokinetics of linagliptin 5 mg in male and female patients with varying degrees of chronic renal impairment. The study included 6 healthy subjects with normal renal function (creatinine clearance [CrCl] ≥80 mL/min), 6 patients with mild renal impairment (CrCl 50 to <80 mL/min), 6 patients with moderate renal impairment (CrCl 30 to <50 mL/min), 10 patients with type 2 diabetes mellitus and severe renal impairment (CrCl <30 mL/min), and 11 patients with type 2 diabetes mellitus and normal renal function. Creatinine clearance was measured by 24-hour urinary creatinine clearance measurements or estimated from serum creatinine based on the Cockcroft-Gault formula.
Under steady-state conditions, linagliptin exposure in patients with mild renal impairment was comparable to healthy subjects.
In patients with moderate renal impairment under steady-state conditions, mean exposure of linagliptin increased (AUC τ,ss by 71% and C max by 46%) compared with healthy subjects. This increase was not associated with a prolonged accumulation half-life, terminal half-life, or an increased accumulation factor. Renal excretion of linagliptin was below 5% of the administered dose and was not affected by decreased renal function.
Patients with type 2 diabetes mellitus and severe renal impairment showed steady-state exposure approximately 40% higher than that of patients with type 2 diabetes mellitus and normal renal function (increase in AUC τ,ss by 42% and C max by 35%). For both type 2 diabetes mellitus groups, renal excretion was below 7% of the administered dose.
These findings were further supported by the results of population pharmacokinetic analyses.
10 overdosage (10 OVERDOSAGE)
In the event of an overdose with linagliptin, contact the Poison Control Center. Removal of linagliptin by hemodialysis or peritoneal dialysis is unlikely.
Hepatic Impairment
In patients with mild hepatic impairment (Child-Pugh class A), steady-state exposure (AUC τ,ss) of linagliptin was approximately 25% lower and C max,ss was approximately 36% lower than in healthy subjects. In patients with moderate hepatic impairment (Child-Pugh class B), AUC ss of linagliptin was about 14% lower and C max,ss was approximately 8% lower than in healthy subjects. Patients with severe hepatic impairment (Child-Pugh class C) had comparable exposure of linagliptin in terms of AUC 0-24 and approximately 23% lower C max compared with healthy subjects. Reductions in the pharmacokinetic parameters seen in patients with hepatic impairment did not result in reductions in DPP-4 inhibition.
11 description (11 DESCRIPTION)
Linagliptin tablets contain, as the active ingredient, an orally-active inhibitor of the dipeptidyl peptidase-4 (DPP-4) enzyme.
Linagliptin is described chemically as 1H-Purine-2,6-dione, 8-[(3R)-3-amino-1-piperidinyl]-7-(2-butyn-1-yl)-3,7-dihydro-3-methyl-1-[(4-methyl-2-quinazolinyl)methyl]-
The empirical formula is C 25H 28N 8O 2 and the molecular weight is 472.54 g/mol. The structural formula is:
Linagliptin is a white to yellowish, not or only slightly hygroscopic solid substance. It is very slightly soluble in water (0.9 mg/mL). Linagliptin is soluble in methanol (ca. 60 mg/mL), sparingly soluble in ethanol (ca. 10 mg/mL), very slightly soluble in isopropanol (<1 mg/mL), and very slightly soluble in acetone (ca. 1 mg/mL).
Each film-coated tablet of linagliptin contains 5 mg of linagliptin free base and the following inactive ingredients: mannitol, pregelatinized starch, copovidone, and magnesium stearate. In addition, the film coating contains the following inactive ingredients: hypromellose, titanium dioxide and polyethylene glycol.
5.1 pancreatitis (5.1 Pancreatitis)
Acute pancreatitis, including fatal pancreatitis, has been reported in patients treated with linagliptin.
Take careful notice of potential signs and symptoms of pancreatitis. If pancreatitis is suspected, promptly discontinue linagliptin and initiate appropriate management. It is unknown whether patients with a history of pancreatitis are at increased risk for the development of pancreatitis while using linagliptin.
5.2 heart Failure (5.2 Heart Failure)
An association between DPP-4 inhibitor treatment and heart failure has been observed in cardiovascular outcomes trials for two other members of the DPP-4 inhibitor class. These trials evaluated patients with type 2 diabetes mellitus and atherosclerotic cardiovascular disease.
Consider the risks and benefits of linagliptin prior to initiating treatment in patients at risk for heart failure, such as those with a prior history of heart failure and a history of renal impairment, and observe these patients for signs and symptoms of heart failure during therapy. Advise patients of the characteristic symptoms of heart failure and to immediately report such symptoms. If heart failure develops, evaluate and manage according to current standards of care and consider discontinuation of linagliptin.
8.4 pediatric Use (8.4 Pediatric Use)
Safety and effectiveness of linagliptin in pediatric patients under 18 years of age have not been established.
8.5 geriatric Use (8.5 Geriatric Use)
In the 15 type 2 diabetes studies with linagliptin, 1085 linagliptin-treated patients were 65 years of age and older (including 131 linagliptin-treated patients 75 years of age and older). Of these 15 studies, 12 were double-blind placebo-controlled. In these 12 studies, 591 linagliptin-treated patients were 65 years of age and older (including 82 linagliptin-treated patients 75 years of age and older). In these linagliptin studies, no overall differences in safety or effectiveness of linagliptin were observed between geriatric patients and younger adult patients.
4 contraindications (4 CONTRAINDICATIONS)
Linagliptin is contraindicated in patients with a history of a hypersensitivity reaction to linagliptin, such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial Linagliptin is contraindicated in patients with hypersensitivity to linagliptin or any of the excipients in linagliptin tablets, reactions such as anaphylaxis, angioedema, exfoliative skin conditions, urticaria, or bronchial hyperreactivity have occurred [see Warnings and Precautions (5.4) and Adverse Reactions (6)] .
6 adverse Reactions (6 ADVERSE REACTIONS)
The following serious adverse reactions are described below or elsewhere in the prescribing information:
- Pancreatitis [see Warnings and Precautions (5.1)]
- Heart Failure [see Warnings and Precautions (5.2)]
- Use with Medications Known to Cause Hypoglycemia [see Warnings and Precautions (5.3)]
- Hypersensitivity Reactions [see Warnings and Precautions (5.4)]
- Severe and Disabling Arthralgia [see Warnings and Precautions (5.5)]
- Bullous Pemphigoid [see Warnings and Precautions (5.6)]
7 drug Interactions (7 DRUG INTERACTIONS)
Strong P-glycoprotein/CYP3A4 inducer: The efficacy of linagliptin may be reduced when administered in combination (e.g., with rifampin). Use of alternative treatments is strongly recommended. (7.1)
8.6 renal Impairment (8.6 Renal Impairment)
No dose adjustment is recommended for patients with renal impairment [see Clinical Pharmacology (12.3)] .
Cardiac Electrophysiology
In a randomized, placebo-controlled, active-comparator, 4-way crossover study, 36 healthy subjects were administered a single oral dose of linagliptin 5 mg, linagliptin 100 mg (20 times the recommended dose), moxifloxacin, and placebo. No increase in QTc was observed with either the recommended dose of 5 mg or the 100-mg dose. At the 100-mg dose, peak linagliptin plasma concentrations were approximately 38-fold higher than the peak concentrations following a 5-mg dose.
12.2 pharmacodynamics (12.2 Pharmacodynamics)
Linagliptin binds to DPP-4 in a reversible manner and thus increases the concentrations of incretin hormones. Linagliptin glucose dependently increases insulin secretion and lowers glucagon secretion, thus resulting in better regulation of glucose homeostasis. Linagliptin binds selectively to DPP-4, and selectively inhibits DPP-4 but not DPP-8 or DPP-9 activity in vitro at concentrations approximating therapeutic exposures.
12.3 pharmacokinetics (12.3 Pharmacokinetics)
The pharmacokinetics of linagliptin has been characterized in healthy subjects and patients with type 2 diabetes. After oral administration of a single 5-mg dose to healthy subjects, peak plasma concentrations of linagliptin occurred at approximately 1.5 hours post dose (T max); the mean plasma area under the curve (AUC) was 139 nmol*h/L and maximum concentration (C max) was 8.9 nmol/L.
Plasma concentrations of linagliptin decline in at least a biphasic manner with a long terminal half-life (>100 hours), related to the saturable binding of linagliptin to DPP-4. The prolonged elimination phase does not contribute to the accumulation of the drug. The effective half-life for accumulation of linagliptin, as determined from oral administration of multiple doses of linagliptin 5 mg, is approximately 12 hours. After once-daily dosing, steady-state plasma concentrations of linagliptin 5 mg are reached by the third dose, and C max and AUC increased by a factor of 1.3 at steady-state compared with the first dose. The intra-subject and inter-subject coefficients of variation for linagliptin AUC were small (12.6% and 28.5%, respectively). Plasma AUC of linagliptin increased in a less than dose-proportional manner in the dose range of 1 to 10 mg. The pharmacokinetics of linagliptin is similar in healthy subjects and in patients with type 2 diabetes.
2.1 recommended Dosing (2.1 Recommended Dosing)
The recommended dose of linagliptin is 5 mg once daily.
Linagliptin tablets can be taken with or without food.
5.6 bullous Pemphigoid (5.6 Bullous Pemphigoid)
Postmarketing cases of bullous pemphigoid requiring hospitalization have been reported with DPP-4 inhibitor use. In reported cases, patients typically recovered with topical or systemic immunosuppressive treatment and discontinuation of the DPP-4 inhibitor. Tell patients to report development of blisters or erosions while receiving linagliptin. If bullous pemphigoid is suspected, linagliptin should be discontinued and referral to a dermatologist should be considered for diagnosis and appropriate treatment.
8.7 hepatic Impairment (8.7 Hepatic Impairment)
No dose adjustment is recommended for patients with hepatic impairment [see Clinical Pharmacology (12.3)] .
1 indications and Usage (1 INDICATIONS AND USAGE)
Linagliptin is a dipeptidyl peptidase-4 (DPP-4) inhibitor indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus ( 1)
Limitations of Use
Body Mass Index (bmi)/weight (Body Mass Index (BMI)/Weight)
No dose adjustment is necessary based on BMI/weight. BMI/weight had no clinically meaningful effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis.
12.1 mechanism of Action (12.1 Mechanism of Action)
Linagliptin is an inhibitor of DPP-4, an enzyme that degrades the incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). Thus, linagliptin increases the concentrations of active incretin hormones, stimulating the release of insulin in a glucose-dependent manner and decreasing the levels of glucagon in the circulation. Both incretin hormones are involved in the physiological regulation of glucose homeostasis. Incretin hormones are secreted at a low basal level throughout the day and levels rise immediately after meal intake. GLP-1 and GIP increase insulin biosynthesis and secretion from pancreatic beta cells in the presence of normal and elevated blood glucose levels. Furthermore, GLP-1 also reduces glucagon secretion from pancreatic alpha-cells, resulting in a reduction in hepatic glucose output.
5 warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Pancreatitis: There have been reports of acute pancreatitis, including fatal pancreatitis. If pancreatitis is suspected, promptly discontinue linagliptin. (5.1)
- Heart failure: Heart failure has been observed with two other members of the DPP-4 inhibitor class. Consider risks and benefits of linagliptin in patients who have known risk factors for heart failure. Monitor for signs and symptoms. (5.2)
- Hypoglycemia: When used with an insulin secretagogue (e.g., sulfonylurea (SU)) or insulin, consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemia (5.3)
- Hypersensitivity reactions: Serious hypersensitivity reactions (e.g., anaphylaxis, angioedema, and exfoliative skin conditions) have occurred with linagliptin. If hypersensitivity reactions occur, discontinue linagliptin, treat promptly, and monitor until signs and symptoms resolve. (5.4)
- Arthralgia: Severe and disabling arthralgia has been reported in patients taking DPP-4 inhibitors. Consider as a possible cause for severe joint pain and discontinue drug if appropriate. (5.5)
- Bullous pemphigoid: There have been reports of bullous pemphigoid requiring hospitalization. Tell patients to report development of blisters or erosions. If bullous pemphigoid is suspected, discontinue linagliptin (5.6).
2 dosage and Administration (2 DOSAGE AND ADMINISTRATION)
14.1 glycemic Control Trials (14.1 Glycemic Control Trials)
Linagliptin has been studied as monotherapy and in combination with metformin, sulfonylurea, pioglitazone, and insulin. Linagliptin has also been studied in patients with type 2 diabetes and severe chronic renal impairment.
In patients with type 2 diabetes, treatment with linagliptin produced clinically significant improvements in hemoglobin A1c (A1C), fasting plasma glucose (FPG), and 2-hour post-prandial glucose (PPG) compared with placebo.
3 dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Linagliptin 5 mg tablets are white or off-white, round, biconvex, film-coated tablets with “S75” debossed on one side and blank on the other side.
6.2 postmarketing Experience (6.2 Postmarketing Experience)
Additional adverse reactions have been identified during postapproval use of linagliptin. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Acute pancreatitis, including fatal pancreatitis [see Indications and Usage (1)]
- Hypersensitivity reactions including anaphylaxis, angioedema, and exfoliative skin conditions
- Severe and disabling arthralgia
- Bullous pemphigoid
- Rash
- Mouth ulceration, stomatitis
- Rhabdomyolysis
5.4 hypersensitivity Reactions (5.4 Hypersensitivity Reactions)
There have been postmarketing reports of serious hypersensitivity reactions in patients treated with linagliptin. These reactions include anaphylaxis, angioedema, and exfoliative skin conditions. Onset of these reactions predominantly occurred within the first 3 months after initiation of treatment with linagliptin, with some reports occurring after the first dose. If a serious hypersensitivity reaction is suspected, discontinue linagliptin, assess for other potential causes for the event, and institute alternative treatment for diabetes.
Angioedema has also been reported with other dipeptidyl peptidase-4 (DPP-4) inhibitors. Use caution in a patient with a history of angioedema to another DPP-4 inhibitor because it is unknown whether such patients will be predisposed to angioedema with linagliptin.
6.1 clinical Trials Experience (6.1 Clinical Trials Experience)
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety evaluation of linagliptin 5 mg once daily in patients with type 2 diabetes is based on 14 placebo-controlled trials, 1 active-controlled study, and one study in patients with severe renal impairment. In the 14 placebo-controlled studies, a total of 3625 patients were randomized and treated with linagliptin 5 mg daily and 2176 with placebo. The mean exposure in patients treated with linagliptin across studies was 29.6 weeks. The maximum follow-up was 78 weeks.
Linagliptin 5 mg once daily was studied as monotherapy in three placebo-controlled trials of 18 and 24 weeks’ duration and in five additional placebo-controlled studies lasting ≤18 weeks. The use of linagliptin in combination with other antihyperglycemic agents was studied in six placebo-controlled trials: two with metformin (12 and 24 weeks’ treatment duration); one with a sulfonylurea (18 weeks’ treatment duration); one with metformin and sulfonylurea (24 weeks’ treatment duration); one with pioglitazone (24 weeks’ treatment duration); and one with insulin (primary endpoint at 24 weeks).
In a pooled dataset of 14 placebo-controlled clinical trials, adverse reactions that occurred in ≥2% of patients receiving linagliptin (n = 3625) and more commonly than in patients given placebo (n = 2176), are shown in Table 1. The overall incidence of adverse events with linagliptin were similar to placebo.
| Number (%) of Patients | ||
|
Linagliptin
5 mg
n = 3625 |
Placebo
n = 2176 |
|
| Nasopharyngitis | 254 (7.0) | 132 (6.1) |
| Diarrhea | 119 (3.3) | 65 (3.0) |
| Cough | 76 (2.1) | 30 (1.4) |
Rates for other adverse reactions for linagliptin 5 mg vs placebo when linagliptin was used in combination with specific anti-diabetic agents were: urinary tract infection (3.1% vs 0%) and hypertriglyceridemia (2.4% vs 0%) when linagliptin was used as add-on to sulfonylurea; hyperlipidemia (2.7% vs 0.8%) and weight increased (2.3% vs 0.8%) when linagliptin was used as add-on to pioglitazone; and constipation (2.1% vs 1%) when linagliptin was used as add-on to basal insulin therapy. Other adverse reactions reported in clinical studies with treatment of linagliptin were hypersensitivity (e.g., urticaria, angioedema, localized skin exfoliation, or bronchial hyperreactivity) and myalgia.
Following 104 weeks’ treatment in a controlled study comparing linagliptin with glimepiride in which all patients were also receiving metformin, adverse reactions reported in ≥5% of patients treated with linagliptin (n = 776) and more frequently than in patients treated with a sulfonylurea (n = 775) were back pain (9.1% vs 8.4%), arthralgia (8.1% vs 6.1%), upper respiratory tract infection (8.0% vs 7.6%), headache (6.4% vs 5.2%), cough (6.1% vs 4.9%), and pain in extremity (5.3% vs 3.9%).
In the clinical trial program, pancreatitis was reported in 15.2 cases per 10,000 patient year exposure while being treated with linagliptin compared with 3.7 cases per 10,000 patient year exposure while being treated with comparator (placebo and active comparator, sulfonylurea). Three additional cases of pancreatitis were reported following the last administered dose of linagliptin.
17 patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Pancreatitis
Inform patients that acute pancreatitis
has been reported during use of linagliptin. Inform patients
that persistent severe abdominal pain, sometimes radiating to the
back, which may or may not be accompanied by vomiting, is the hallmark
symptom of acute pancreatitis. Instruct patients to discontinue linagliptin
promptly and contact their physician if persistent severe abdominal
pain occurs [
see
Warnings and Precautions (5.1)
].
Heart Failure
Inform patients of the signs and symptoms of heart failure. Before initiating linagliptin, patients should be asked about a history of heart failure or other risk factors for heart failure including moderate to severe renal impairment. Instruct patients to contact their healthcare provider as soon as possible if they experience symptoms of heart failure, including increasing shortness of breath, rapid increase in weight or swelling of the feet [
see
Warnings and Precautions (5.2)
].
Hypoglycemia
Inform patients that the incidence of hypoglycemia
is increased when linagliptin is added to a sulfonylurea or insulin
and that a lower dose of the sulfonylurea or insulin may be required
to reduce the risk of hypoglycemia
[see
Warnings and Precautions (5.3)]
.
Hypersensitivity Reactions
Inform patients that serious allergic reactions, such as anaphylaxis,
angioedema, and exfoliative skin conditions, have been reported during
postmarketing use of linagliptin. If symptoms of allergic reactions
(such as rash, skin flaking or peeling, urticaria, swelling of the
skin, or swelling of the face, lips, tongue, and throat that may cause
difficulty in breathing or swallowing) occur, patients must stop taking
linagliptin and seek medical advice promptly
[see
Warnings and Precautions (5.4)]
.
Severe and Disabling Arthralgia
Inform patients that severe and disabling joint pain
may occur with this class of drugs. The time to onset of symptoms
can range from one day to years. Instruct patients to seek medical
advice if severe joint pain occurs
[see
Warnings and Precautions (5.5)].
Bullous Pemphigoid
Inform patients that bullous pemphigoid has been reported during use of linagliptin. Instruct patients to seek medical advice if blisters
or erosions occur
[see
Warnings and Precautions (5.6)].
Missed Dose
Instruct patients to take linagliptin only as prescribed.
If a dose is missed, advise patients not to double their next dose.
5.5 severe and Disabling Arthralgia (5.5 Severe and Disabling Arthralgia)
There have been postmarketing reports of severe and disabling arthralgia in patients taking DPP-4 inhibitors. The time to onset of symptoms following initiation of drug therapy varied from one day to years. Patients experienced relief of symptoms upon discontinuation of the medication. A subset of patients experienced a recurrence of symptoms when restarting the same drug or a different DPP-4 inhibitor. Consider DPP-4 inhibitors as a possible cause for severe joint pain and discontinue drug if appropriate.
16 how Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
Linagliptin tablets are available as white or off-white, round, biconvex, film-coated tablets containing 5 mg of linagliptin. Linagliptin tablets are debossed with “S75” on one side and blank on the other side.
They are supplied
as follows:
Bottles of 30 (NDC 48792-7865-1)
If repackaging is required, dispense
in a tight container as defined in USP.
7.2 insulin Secretagogues Or Insulin (7.2 Insulin Secretagogues or Insulin)
Coadministration of linagliptin with an insulin secretagogue (e.g., sulfonylurea) or insulin may require lower doses of the insulin secretagogue or insulin to reduce the risk of hypoglycemia [see Warnings and Precautions (5.3)] .
7.1 inducers of P Glycoprotein Or Cyp3a4 Enzymes (7.1 Inducers of P-glycoprotein or CYP3A4 Enzymes)
Rifampin decreased linagliptin exposure, suggesting that the efficacy of linagliptin may be reduced when administered in combination with a strong P-gp or CYP3A4 inducer. Therefore, use of alternative treatments is strongly recommended when linagliptin is to be administered with a strong P-gp or CYP3A4 inducer [see Clinical Pharmacology (12.3)] .
5.3 use With Medications Known to Cause Hypoglycemia (5.3 Use with Medications Known to Cause Hypoglycemia)
Insulin secretagogues and insulin are known to cause hypoglycemia. The use of linagliptin in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin was associated with a higher rate of hypoglycemia compared with placebo in clinical trials [see Adverse Reactions (6.1)] . The use of linagliptin in combination with insulin in subjects with severe renal impairment was associated with a higher rate of hypoglycemia [see Adverse Reactions (6.1)] . Therefore, a lower dose of the insulin secretagogue or insulin may be required to reduce the risk of hypoglycemia when used in combination with linagliptin.
13.1 carcinogenesis, Mutagenesis, Impairment of Fertility (13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility)
Linagliptin did not increase the incidence of tumors in male and female rats in a 2-year study at doses of 6, 18, and 60 mg/kg. The highest dose of 60 mg/kg is approximately 418 times the clinical dose of 5 mg/day based on AUC exposure. Linagliptin did not increase the incidence of tumors in mice in a 2-year study at doses up to 80 mg/kg (males) and 25 mg/kg (females), or approximately 35 and 270 times the clinical dose based on AUC exposure. Higher doses of linagliptin in female mice (80 mg/kg) increased the incidence of lymphoma at approximately 215 times the clinical dose based on AUC exposure.
Linagliptin was not mutagenic or clastogenic with or without metabolic activation in the Ames bacterial mutagenicity assay, a chromosomal aberration test in human lymphocytes, and an in vivo micronucleus assay.
In fertility studies in rats, linagliptin had no adverse effects on early embryonic development, mating, fertility, or bearing live young up to the highest dose of 240 mg/kg (approximately 943 times the clinical dose based on AUC exposure).
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:52:23.332181 · Updated: 2026-03-14T22:43:29.901552