Lumakras
c80a362c-7ac3-4894-a076-0691e68ef8c1
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
LUMAKRAS is an inhibitor of the RAS GTPase family indicated for: KRAS G12C-mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer (NSCLC) As a single agent, for the treatment of adult patients with KRAS G12C-mutated locally advanced or metastatic NSCLC, as determined by an FDA-approved test, who have received at least one prior systemic therapy. ( 1.1 ) This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DOR). Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). ( 1.1 ) KRAS G12C-mutated Metastatic Colorectal Cancer (mCRC) In combination with panitumumab, for the treatment of adult patients with KRAS G12C-mutated mCRC as determined by an FDA approved-test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy. ( 1.2 )
Dosage and Administration
Recommended dosage as a single agent for NSCLC and in combination with panitumumab for mCRC: 960 mg orally once daily. ( 2.2 ) Swallow tablets whole with or without food. ( 2.2 )
Contraindications
None.
Warnings and Precautions
Hepatotoxicity: Monitor liver function tests every 3 weeks for the first 3 months of treatment then once monthly as clinically indicated. Consider administering systemic corticosteroids and withhold, reduce the dose, or permanently discontinue LUMAKRAS based on the severity. ( 2.3 , 5.1 ) Interstitial Lung Disease (ILD)/Pneumonitis: Monitor for new or worsening pulmonary symptoms. Immediately withhold LUMAKRAS for suspected ILD/pneumonitis and permanently discontinue if no other potential causes of ILD/pneumonitis are identified. ( 2.3 , 5.2 )
Adverse Reactions
LUMAKRAS dose reduction levels are summarized in Table 1. If adverse reactions occur, a maximum of two dose reductions are permitted. Discontinue LUMAKRAS if patients are unable to tolerate the minimum dose of 240 mg once daily. When LUMAKRAS is administered in combination with panitumumab, and LUMAKRAS is temporarily withheld or permanently discontinued, temporarily withhold or permanently discontinue panitumumab, respectively [see Clinical Studies (14.2) ] . Refer to the full prescribing information of panitumumab for dose modifications for adverse reactions associated with the use of panitumumab. Treatment with LUMAKRAS as a single agent may be continued if panitumumab is permanently discontinued [see Clinical Pharmacology (12.1) , Clinical Studies (14.2) ]. Refer to Table 2 for dose modification guidelines and management of adverse reactions associated with the use of LUMAKRAS as a single agent or as combination therapy with panitumumab. Table 1. Recommended LUMAKRAS Dose Reduction Levels for Adverse Reactions Dose Reduction Level Dose First dose reduction 480 mg (two 240 mg or four 120 mg tablets) once daily Second dose reduction 240 mg (one 240 mg or two 120 mg tablets) once daily Table 2. Recommended LUMAKRAS Dosage Modifications for Adverse Reactions Adverse Reaction Severity Grading defined by National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 5.0 . Dosage Modification When LUMAKRAS is administered in combination with panitumumab, withhold or permanently discontinue treatment with panitumumab when withholding or permanently discontinuing treatment with LUMAKRAS. ALT = alanine aminotransferase; AST = aspartate aminotransferase; ULN = upper limit of normal Hepatotoxicity [see Warnings and Precautions (5.1) ] AST or ALT > 3 × and up to 5 × ULN (or > 3 × and up to 5 × baseline if baseline abnormal) with symptoms or AST or ALT > 5 × ULN (or > 5 × baseline if baseline abnormal) Withhold LUMAKRAS until recovery to ≤ 3 × ULN or to ≤ 3 × baseline if baseline abnormal. Resume LUMAKRAS at the next lower dose level. AST or ALT > 3 × ULN with total bilirubin > 2 × ULN Permanently discontinue LUMAKRAS if no alternative cause is identified. If alternative cause is identified, do not resume LUMAKRAS until AST/ALT/bilirubin return to baseline. Interstitial Lung Disease (ILD)/ pneumonitis [see Warnings and Precautions (5.2) ] Any Grade Withhold LUMAKRAS if ILD/pneumonitis is suspected. Permanently discontinue LUMAKRAS if ILD/pneumonitis is confirmed. Nausea or vomiting despite appropriate supportive care (including anti-emetic therapy) [see Adverse Reactions (6.1) ] Grade 3 to 4 Withhold LUMAKRAS until recovery to ≤ Grade 1 or baseline. Resume LUMAKRAS at the next lower dose level. Diarrhea despite appropriate supportive care (including anti-diarrheal therapy) [see Adverse Reactions (6.1) ] Grade 3 to 4 Withhold LUMAKRAS until recovery to ≤ Grade 1 or baseline. Resume LUMAKRAS at the next lower dose level. Other adverse reactions [see Adverse Reactions (6.1) ] Grade 3 to 4 Withhold LUMAKRAS until recovery to ≤ Grade 1 or baseline. Resume LUMAKRAS at the next lower dose level.
Drug Interactions
Acid-Reducing Agents: Avoid coadministration with proton pump inhibitors (PPIs) and H 2 receptor antagonists. If an acid-reducing agent cannot be avoided, administer LUMAKRAS 4 hours before or 10 hours after a local antacid. ( 2.4 , 7.1 ) Strong CYP3A4 Inducers: Avoid coadministration with strong CYP3A4 inducers. ( 7.1 ) CYP3A4 Substrates: Avoid coadministration with CYP3A4 substrates for which minimal concentration changes may lead to therapeutic failures of the substrate. If coadministration cannot be avoided, adjust the substrate dosage in accordance to its Prescribing Information. ( 7.2 ) P-gp substrates: Avoid coadministration with P-gp substrates for which minimal concentration changes may lead to serious toxicities. If coadministration cannot be avoided, decrease the substrate dosage in accordance to its Prescribing Information. ( 7.2 )
Description
Indications and Usage ( 1 ) 01/2025 Dosage and Administration ( 2.1 , 2.2 , 2.3 ) 01/2025 Warnings and Precaution ( 5.1 , 5.2 ) 01/2025
Medication Information
Warnings and Precautions
Hepatotoxicity: Monitor liver function tests every 3 weeks for the first 3 months of treatment then once monthly as clinically indicated. Consider administering systemic corticosteroids and withhold, reduce the dose, or permanently discontinue LUMAKRAS based on the severity. ( 2.3 , 5.1 ) Interstitial Lung Disease (ILD)/Pneumonitis: Monitor for new or worsening pulmonary symptoms. Immediately withhold LUMAKRAS for suspected ILD/pneumonitis and permanently discontinue if no other potential causes of ILD/pneumonitis are identified. ( 2.3 , 5.2 )
Indications and Usage
LUMAKRAS is an inhibitor of the RAS GTPase family indicated for: KRAS G12C-mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer (NSCLC) As a single agent, for the treatment of adult patients with KRAS G12C-mutated locally advanced or metastatic NSCLC, as determined by an FDA-approved test, who have received at least one prior systemic therapy. ( 1.1 ) This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DOR). Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). ( 1.1 ) KRAS G12C-mutated Metastatic Colorectal Cancer (mCRC) In combination with panitumumab, for the treatment of adult patients with KRAS G12C-mutated mCRC as determined by an FDA approved-test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy. ( 1.2 )
Dosage and Administration
Recommended dosage as a single agent for NSCLC and in combination with panitumumab for mCRC: 960 mg orally once daily. ( 2.2 ) Swallow tablets whole with or without food. ( 2.2 )
Contraindications
None.
Adverse Reactions
LUMAKRAS dose reduction levels are summarized in Table 1. If adverse reactions occur, a maximum of two dose reductions are permitted. Discontinue LUMAKRAS if patients are unable to tolerate the minimum dose of 240 mg once daily. When LUMAKRAS is administered in combination with panitumumab, and LUMAKRAS is temporarily withheld or permanently discontinued, temporarily withhold or permanently discontinue panitumumab, respectively [see Clinical Studies (14.2) ] . Refer to the full prescribing information of panitumumab for dose modifications for adverse reactions associated with the use of panitumumab. Treatment with LUMAKRAS as a single agent may be continued if panitumumab is permanently discontinued [see Clinical Pharmacology (12.1) , Clinical Studies (14.2) ]. Refer to Table 2 for dose modification guidelines and management of adverse reactions associated with the use of LUMAKRAS as a single agent or as combination therapy with panitumumab. Table 1. Recommended LUMAKRAS Dose Reduction Levels for Adverse Reactions Dose Reduction Level Dose First dose reduction 480 mg (two 240 mg or four 120 mg tablets) once daily Second dose reduction 240 mg (one 240 mg or two 120 mg tablets) once daily Table 2. Recommended LUMAKRAS Dosage Modifications for Adverse Reactions Adverse Reaction Severity Grading defined by National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 5.0 . Dosage Modification When LUMAKRAS is administered in combination with panitumumab, withhold or permanently discontinue treatment with panitumumab when withholding or permanently discontinuing treatment with LUMAKRAS. ALT = alanine aminotransferase; AST = aspartate aminotransferase; ULN = upper limit of normal Hepatotoxicity [see Warnings and Precautions (5.1) ] AST or ALT > 3 × and up to 5 × ULN (or > 3 × and up to 5 × baseline if baseline abnormal) with symptoms or AST or ALT > 5 × ULN (or > 5 × baseline if baseline abnormal) Withhold LUMAKRAS until recovery to ≤ 3 × ULN or to ≤ 3 × baseline if baseline abnormal. Resume LUMAKRAS at the next lower dose level. AST or ALT > 3 × ULN with total bilirubin > 2 × ULN Permanently discontinue LUMAKRAS if no alternative cause is identified. If alternative cause is identified, do not resume LUMAKRAS until AST/ALT/bilirubin return to baseline. Interstitial Lung Disease (ILD)/ pneumonitis [see Warnings and Precautions (5.2) ] Any Grade Withhold LUMAKRAS if ILD/pneumonitis is suspected. Permanently discontinue LUMAKRAS if ILD/pneumonitis is confirmed. Nausea or vomiting despite appropriate supportive care (including anti-emetic therapy) [see Adverse Reactions (6.1) ] Grade 3 to 4 Withhold LUMAKRAS until recovery to ≤ Grade 1 or baseline. Resume LUMAKRAS at the next lower dose level. Diarrhea despite appropriate supportive care (including anti-diarrheal therapy) [see Adverse Reactions (6.1) ] Grade 3 to 4 Withhold LUMAKRAS until recovery to ≤ Grade 1 or baseline. Resume LUMAKRAS at the next lower dose level. Other adverse reactions [see Adverse Reactions (6.1) ] Grade 3 to 4 Withhold LUMAKRAS until recovery to ≤ Grade 1 or baseline. Resume LUMAKRAS at the next lower dose level.
Drug Interactions
Acid-Reducing Agents: Avoid coadministration with proton pump inhibitors (PPIs) and H 2 receptor antagonists. If an acid-reducing agent cannot be avoided, administer LUMAKRAS 4 hours before or 10 hours after a local antacid. ( 2.4 , 7.1 ) Strong CYP3A4 Inducers: Avoid coadministration with strong CYP3A4 inducers. ( 7.1 ) CYP3A4 Substrates: Avoid coadministration with CYP3A4 substrates for which minimal concentration changes may lead to therapeutic failures of the substrate. If coadministration cannot be avoided, adjust the substrate dosage in accordance to its Prescribing Information. ( 7.2 ) P-gp substrates: Avoid coadministration with P-gp substrates for which minimal concentration changes may lead to serious toxicities. If coadministration cannot be avoided, decrease the substrate dosage in accordance to its Prescribing Information. ( 7.2 )
Description
Indications and Usage ( 1 ) 01/2025 Dosage and Administration ( 2.1 , 2.2 , 2.3 ) 01/2025 Warnings and Precaution ( 5.1 , 5.2 ) 01/2025
Section 42229-5
KRAS G12C-mutated Locally Advanced or Metastatic NSCLC
Select patients for treatment of locally advanced or metastatic NSCLC with LUMAKRAS based on the presence of KRAS G12C mutation in tumor or plasma specimens. If no mutation is detected in a plasma specimen, test tumor tissue [see Clinical Studies (14.1)].
Section 42230-3
| PATIENT INFORMATION LUMAKRAS® (loo-ma-krass) (sotorasib) tablets |
||
|---|---|---|
| What is LUMAKRAS? | ||
LUMAKRAS is a prescription medicine used in adults:
It is not known if LUMAKRAS is safe and effective in children. What should I tell my healthcare provider before taking LUMAKRAS? |
||
Before taking LUMAKRAS, tell your healthcare provider about all your medical conditions, including if you:
Especially tell your healthcare provider if you take antacid medicines, including Proton Pump Inhibitor (PPI) medicines or H2 blockers during treatment with LUMAKRAS. Ask your healthcare provider if you are not sure. How should I take LUMAKRAS? |
||
|
||
LUMAKRAS may cause serious side effects, including:
|
||
|
|
|
|
||
| Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with LUMAKRAS if you develop side effects. The most common side effects of LUMAKRAS when used alone for NSCLC include: |
||
|
|
|
| The most common side effects of LUMAKRAS when used in combination with panitumumab for CRC include: | ||
|
|
|
| These are not all the possible side effects of LUMAKRAS. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. You may also report side effects to Amgen at 1-800-772-6436 (1-800-77-AMGEN). How should I store LUMAKRAS? |
||
General information about the safe and effective use of LUMAKRAS. |
||
| Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use LUMAKRAS for a condition for which it was not prescribed. Do not give LUMAKRAS to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about LUMAKRAS that is written for healthcare professionals. What are the ingredients in LUMAKRAS? |
||
|
Active Ingredient: sotorasib Inactive Ingredients: microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, and magnesium stearate. Tablet film coating material contains polyvinyl alcohol, titanium dioxide, polyethylene glycol, talc, iron oxide yellow and iron oxide red (320 mg tablet only). |
||
| Manufactured by: Amgen Inc., One Amgen Center Drive, Thousand Oaks, CA 91320-1799 U.S.A. © 2021, 2023, 2025 Amgen Inc. All rights reserved. For more information, go to www.LUMAKRAS.com or call 1-800-772-6436 (1-800-77-AMGEN). This Patient Information has been approved by the U.S. Food and Drug Administration. |
Revised: 01/2025 | |
| [part number] v3 |
Section 43683-2
Section 44425-7
Storage and Handling
Store at 20°C to 25°C (68°F to 77°F). Excursions permitted from 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
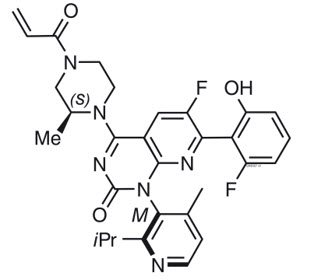
11 Description
Sotorasib is an inhibitor of the RAS GTPase family. The molecular formula is C30H30F2N6O3, and the molecular weight is 560.6 g/mol. The chemical name of sotorasib is 6-fluoro-7-(2-fluoro-6-hydroxyphenyl)-(1M)-1-[4-methyl-2-(propan-2-yl)pyridin-3-yl]-4-[(2S)-2-methyl-4-(prop-2-enoyl)piperazin-1-yl]pyrido[2,3-d]pyrimidin-2(1H)-one.
The chemical structure of sotorasib is shown below:
Sotorasib has pKa values of 8.06 and 4.56. The solubility of sotorasib in the aqueous media decreases over the range pH 1.2 to 6.8 from 1.3 mg/mL to 0.03 mg/mL.
LUMAKRAS is supplied as film-coated tablets for oral use containing 320 mg, 240 mg or 120 mg of sotorasib. Inactive ingredients in the tablet core are microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, and magnesium stearate. The film coating material consists of polyvinyl alcohol, titanium dioxide, polyethylene glycol, talc, iron oxide yellow and iron oxide red (320 mg tablet only).
8.4 Pediatric Use
The safety and effectiveness of LUMAKRAS have not been established in pediatric patients.
8.5 Geriatric Use
Of the 357 patients with any tumor type who received LUMAKRAS 960 mg orally once daily in CodeBreaK 100, 46% were 65 and over, and 10% were 75 and over. No overall differences in safety or effectiveness were observed between older patients and younger patients treated with LUMAKRAS as a single agent.
In a pooled analysis of 132 patients who received LUMAKRAS 960 mg in combination with panitumumab for KRAS G12C-mutated mCRC, 30% were 65 and over while 9% were 75 and over. No overall differences in safety or efficacy were observed between older patients (≥ 65 years of age) compared to younger patients, treated with LUMAKRAS 960 mg in combination with panitumumab.
5.1 Hepatotoxicity
LUMAKRAS can cause hepatotoxicity and increased alanine aminotransferase (ALT) or increased aspartate aminotransferase (AST) which may lead to drug-induced liver injury and hepatitis.
In the pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg [see Adverse Reactions (6.1)], hepatotoxicity occurred in 27% of patients, of which 16% were Grade ≥ 3. Among patients with hepatotoxicity who required dosage modifications, 64% required treatment with corticosteroids.
In this pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg, 17% of patients who received LUMAKRAS had increased ALT/increased AST; of which 9% were Grade ≥ 3. The median time to first onset of increased ALT/AST was 6.3 weeks (range: 0.4 to 42). Increased ALT/AST leading to dose interruption or reduction occurred in 9% of patients treated with LUMAKRAS. LUMAKRAS was permanently discontinued due to increased ALT/AST in 2.7% of patients. Drug-induced liver injury occurred in 1.6% (all grades) including 1.3% (Grade ≥ 3).
In this pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg, a total of 40% patients with recent (≤ 3 months) immunotherapy prior to starting LUMAKRAS had an event of hepatotoxicity. An event of hepatotoxicity was observed in 18% of patients who started LUMAKRAS more than 3 months after last dose of immunotherapy and in 17% of those who never received immunotherapy. Regardless of time from prior immunotherapy, 94% of hepatotoxicity events improved or resolved with dosage modification of LUMAKRAS, with or without corticosteroid treatment.
In the pooled safety population of patients with CRC who received LUMAKRAS 960 mg in combination with panitumumab [see Adverse Reactions (6.1)], hepatotoxicity occurred in 15% of patients, of which 4.8% were Grade 3. A total of 7% of patients who received LUMAKRAS had increased ALT or increased AST, of which 0.8% were Grade 3. The median time to first onset of increased ALT or increased AST was 10 weeks (range: 2 to 22). Increased ALT or increased AST leading to dose interruption occurred in 2.4% of patients. A total of 3.2% of patients who received LUMAKRAS had hyperbilirubinemia, of which 2.4% were Grade 3. The median time to first onset of hyperbilirubinemia was 12 weeks (range: 0, 29). Hyperbilirubinemia leading to dose interruption occurred in 1.6% of patients. Among patients with hepatotoxicity, 21% received corticosteroids.
Monitor liver function tests (ALT, AST, alkaline phosphatase and total bilirubin) prior to the start of LUMAKRAS, every 3 weeks for the first 3 months of treatment, then once a month or as clinically indicated, with more frequent testing in patients who develop transaminase and/or bilirubin elevations. Withhold, reduce the dose or permanently discontinue LUMAKRAS based on severity of the adverse reaction [see Dosage and Administration (2.3) and Adverse Reactions (6.1)]. Consider administering systemic corticosteroids for the management of hepatotoxicity.
4 Contraindications
None.
6 Adverse Reactions
The following clinically significant adverse reactions are discussed in greater detail in other sections of the labeling:
- Hepatotoxicity [see Warnings and Precautions (5.1)]
- Interstitial Lung Disease (ILD)/Pneumonitis [see Warnings and Precautions (5.2)]
7 Drug Interactions
- Acid-Reducing Agents: Avoid coadministration with proton pump inhibitors (PPIs) and H2 receptor antagonists. If an acid-reducing agent cannot be avoided, administer LUMAKRAS 4 hours before or 10 hours after a local antacid. (2.4, 7.1)
- Strong CYP3A4 Inducers: Avoid coadministration with strong CYP3A4 inducers. (7.1)
- CYP3A4 Substrates: Avoid coadministration with CYP3A4 substrates for which minimal concentration changes may lead to therapeutic failures of the substrate. If coadministration cannot be avoided, adjust the substrate dosage in accordance to its Prescribing Information. (7.2)
- P-gp substrates: Avoid coadministration with P-gp substrates for which minimal concentration changes may lead to serious toxicities. If coadministration cannot be avoided, decrease the substrate dosage in accordance to its Prescribing Information. (7.2)
12.2 Pharmacodynamics
Sotorasib exposure-response relationships and the time course of the pharmacodynamic response are unknown.
12.3 Pharmacokinetics
The pharmacokinetics of sotorasib have been characterized in healthy subjects and in patients with KRAS G12C-mutated solid tumors, including NSCLC. Sotorasib exhibited non-linear, time-dependent, pharmacokinetics over the dose range of 180 mg to 960 mg (0.19 to 1 time the approved recommended dosage) once daily with similar systemic exposure (i.e., AUC0-24h and Cmax) across doses at steady state. Sotorasib systemic exposure was comparable between film-coated tablets and film-coated tablets predispersed in water administered under fasted conditions. Sotorasib plasma concentrations reached steady state within 22 days. No accumulation was observed after repeat LUMAKRAS dosages with a mean accumulation ratio of 0.56 (coefficient of variation (CV): 59%).
8.6 Hepatic Impairment
No dosage modification is recommended in patients with mild to moderate hepatic impairment (Child-Pugh A or B).
The effect of severe hepatic impairment (Child-Pugh C) on the safety of LUMAKRAS is unknown. Monitor for sotorasib adverse reactions in patients with hepatic impairment more frequently since these patients may be at increased risk for adverse reactions including hepatotoxicity [see Clinical Pharmacology (12.3)].
1 Indications and Usage
LUMAKRAS is an inhibitor of the RAS GTPase family indicated for:
KRAS G12C-mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer (NSCLC)
- As a single agent, for the treatment of adult patients with KRAS G12C-mutated locally advanced or metastatic NSCLC, as determined by an FDA-approved test, who have received at least one prior systemic therapy. (1.1)
This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DOR). Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). (1.1)
KRAS G12C-mutated Metastatic Colorectal Cancer (mCRC)
In combination with panitumumab, for the treatment of adult patients with KRAS G12C-mutated mCRC as determined by an FDA approved-test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy. (1.2)
12.1 Mechanism of Action
Sotorasib is an inhibitor of KRAS G12C, a tumor-restricted, mutant-oncogenic form of the RAS GTPase, KRAS. Sotorasib forms an irreversible, covalent bond with the unique cysteine of KRAS G12C, locking the protein in an inactive state that prevents downstream signaling without affecting wild-type KRAS. Sotorasib blocked KRAS signaling, inhibited cell growth, and promoted apoptosis only in KRAS G12C tumor cell lines. Sotorasib inhibited KRAS G12C in vitro and in vivo with minimal detectable off-target activity. In mouse tumor xenograft models, sotorasib-treatment led to tumor regressions and prolonged survival, and was associated with anti-tumor immunity in KRAS G12C models.
In the setting of KRAS G12C-mutant CRC, epidermal growth factor receptor (EGFR) activation has been identified as a mechanism of resistance to KRAS G12C inhibition. In a murine patient-derived colorectal tumor xenograft model, the combination of sotorasib and panitumumab, an EGFR antagonist, had increased antitumor activity compared to either sotorasib or panitumumab alone.
5 Warnings and Precautions
- Hepatotoxicity: Monitor liver function tests every 3 weeks for the first 3 months of treatment then once monthly as clinically indicated. Consider administering systemic corticosteroids and withhold, reduce the dose, or permanently discontinue LUMAKRAS based on the severity. (2.3, 5.1)
- Interstitial Lung Disease (ILD)/Pneumonitis: Monitor for new or worsening pulmonary symptoms. Immediately withhold LUMAKRAS for suspected ILD/pneumonitis and permanently discontinue if no other potential causes of ILD/pneumonitis are identified. (2.3, 5.2)
2 Dosage and Administration
3 Dosage Forms and Strengths
Tablets: 320 mg, beige, oval-shaped, immediate release, film-coated, debossed with "AMG" on one side and "320" on the opposite side.
Tablets: 240 mg, yellow, oval-shaped, immediate release, film-coated, debossed with "AMG" on one side and "240" on the opposite side.
Tablets: 120 mg, yellow, oblong-shaped, immediate release, film-coated, debossed with "AMG" on one side and "120" on the opposite side.
8 Use in Specific Populations
Lactation: Advise not to breastfeed. (8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The pooled safety population described in the WARNINGS AND PRECAUTIONS reflect exposure to LUMAKRAS as a single agent at 960 mg orally once daily until disease progression or unacceptable toxicity in 549 patients with NSCLC with KRAS G12C mutation in the following trials: CodeBreaK 200 (NCT04303780), CodeBreaK 100 (NCT03600883), CodeBreaK 101 (NCT04185883) and CodeBreaK 105 (NCT04380753). Among these 549 patients who received LUMAKRAS, 44% were exposed for 6 months or longer and 21% were exposed for greater than one year.
The pooled safety population described in WARNINGS AND PRECAUTIONS also reflects exposure to LUMAKRAS 960 mg once daily in combination with panitumumab in 126 patients who received LUMAKRAS in combination with panitumumab for mCRC in CodeBreaK 300 (NCT05198934) and CodeBreaK 101 (NCT04185883). Among the 126 patients who received LUMAKRAS 960 mg in combination with panitumumab, 40% were exposed for 6 months or longer and 10% were exposed for greater than one year.
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
13.2 Animal Toxicology And/or Pharmacology
In rats, renal toxicity including minimal to marked histologic tubular degeneration/necrosis and increased kidney weight, urea nitrogen, creatinine, and urinary biomarkers of renal tubular injury were present at doses resulting in exposures approximately ≥ 0.5 times the human AUC at the clinical dose of 960 mg. Increases in cysteine S-conjugate β-lyase pathway metabolism in the rat kidney compared to human may make rats more susceptible to renal toxicity due to local formation of a putative sulfur-containing metabolite than humans.
In the 3-month toxicology study in dogs, sotorasib induced findings in the liver (centrilobular hepatocellular hypertrophy), pituitary gland (hypertrophy of basophils), and thyroid gland (marked follicular cell atrophy, moderate to marked colloid depletion, and follicular cell hypertrophy) at exposures approximately 0.4 times the human exposure based on AUC at the clinical dose of 960 mg. These findings may be due to an adaptive response to hepatocellular enzyme induction and subsequent reduced thyroid hormone levels (i.e., secondary hypothyroidism). Although thyroid levels were not measured in dogs, induction of uridine diphosphate glucuronosyltransferase known to be involved in thyroid hormone metabolism was confirmed in the in vitro dog hepatocyte assay.
2.3 Dosage Modifications for Adverse Reactions
LUMAKRAS dose reduction levels are summarized in Table 1.
If adverse reactions occur, a maximum of two dose reductions are permitted. Discontinue LUMAKRAS if patients are unable to tolerate the minimum dose of 240 mg once daily.
When LUMAKRAS is administered in combination with panitumumab, and LUMAKRAS is temporarily withheld or permanently discontinued, temporarily withhold or permanently discontinue panitumumab, respectively [see Clinical Studies (14.2)]. Refer to the full prescribing information of panitumumab for dose modifications for adverse reactions associated with the use of panitumumab.
Treatment with LUMAKRAS as a single agent may be continued if panitumumab is permanently discontinued [see Clinical Pharmacology (12.1), Clinical Studies (14.2)].
Refer to Table 2 for dose modification guidelines and management of adverse reactions associated with the use of LUMAKRAS as a single agent or as combination therapy with panitumumab.
| Dose Reduction Level | Dose |
|---|---|
| First dose reduction | 480 mg (two 240 mg or four 120 mg tablets) once daily |
| Second dose reduction | 240 mg (one 240 mg or two 120 mg tablets) once daily |
| Adverse Reaction | Severity
Grading defined by National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 5.0.
|
Dosage Modification When LUMAKRAS is administered in combination with panitumumab, withhold or permanently discontinue treatment with panitumumab when withholding or permanently discontinuing treatment with LUMAKRAS.
|
|---|---|---|
| ALT = alanine aminotransferase; AST = aspartate aminotransferase; ULN = upper limit of normal | ||
| Hepatotoxicity [see Warnings and Precautions (5.1)] | AST or ALT > 3 × and up to 5 × ULN (or > 3 × and up to 5 × baseline if baseline abnormal) with symptoms or AST or ALT > 5 × ULN (or > 5 × baseline if baseline abnormal) |
|
| AST or ALT > 3 × ULN with total bilirubin > 2 × ULN |
|
|
| Interstitial Lung Disease (ILD)/ pneumonitis [see Warnings and Precautions (5.2)] | Any Grade |
|
| Nausea or vomiting despite appropriate supportive care (including anti-emetic therapy) [see Adverse Reactions (6.1)] |
Grade 3 to 4 |
|
| Diarrhea despite appropriate supportive care (including anti-diarrheal therapy) [see Adverse Reactions (6.1)] |
Grade 3 to 4 |
|
| Other adverse reactions [see Adverse Reactions (6.1)] |
Grade 3 to 4 |
|
5.2 Interstitial Lung Disease (ild)/pneumonitis
LUMAKRAS can cause ILD/pneumonitis that can be fatal.
In the pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg [see Adverse Reactions (6.1)], ILD/pneumonitis occurred in 2.2% of patients, of which 1.1% were Grade ≥ 3, and 1 case was fatal. The median time to first onset for ILD/pneumonitis was 8.6 weeks (range: 2.1 to 36.7 weeks). LUMAKRAS was permanently discontinued due to ILD/pneumonitis in 1.3% of LUMAKRAS-treated patients. Monitor patients for new or worsening pulmonary symptoms indicative of ILD/pneumonitis (e.g., dyspnea, cough, fever). Immediately withhold LUMAKRAS in patients with suspected ILD/pneumonitis and permanently discontinue LUMAKRAS if no other potential causes of ILD/pneumonitis are identified [see Dosage and Administration (2.3) and Adverse Reactions (6.1)].
In the pooled safety population of patients with CRC who received LUMAKRAS 960 mg in combination with panitumumab, 1 patient experienced a Grade 1 event of ILD/pneumonitis [see Adverse Reactions (6.1)].
14.2 Kras G12c Mutated Metastatic Colorectal Cancer
The efficacy of LUMAKRAS in combination with panitumumab was evaluated in CodeBreaK 300 [NCT05198934], a multicenter, randomized, open-label, active-controlled study conducted in previously treated patients with KRAS G12C-mutated mCRC. Key eligibility criteria included patients 18 years of age or older, who had received at least one prior line of therapy for mCRC, and who had received fluoropyrimidine, oxaliplatin, and irinotecan for metastatic disease unless there was a medical contraindication.
All patients were also required to have prospectively identified KRAS G12C-mutated mCRC in tumor tissue samples by using the QIAGEN therascreen® KRAS RGQ PCR Kit performed in a central laboratory. Other eligibility criteria included an ECOG PS of ≤ 2 and at least one measurable lesion as defined by RECIST v1.1.
A total of 160 patients with previously treated mCRC with the KRAS G12C mutation were randomized 1:1:1 to receive either LUMAKRAS 960 mg orally once daily and panitumumab 6 mg/kg IV every 2 weeks (N = 53), or LUMAKRAS 240 mg orally once daily and panitumumab 6 mg/kg IV every 2 weeks (N = 53), or investigator's choice of SOC trifluridine/tipiracil or regorafenib (N = 54). Randomization was stratified by prior anti-angiogenic therapy (yes or no), time from initial diagnosis of metastatic disease to randomization (≥ 18 months; < 18 months), and ECOG status (0 or 1 versus 2). Patients received treatment until disease progression, lack of clinical benefit or intolerance to treatment. LUMAKRAS discontinuation required panitumumab discontinuation, however, patients could continue to receive LUMAKRAS if panitumumab was discontinued [see Dosage and Administration (2.3)]. Four patients randomized to LUMAKRAS 960 mg in combination with panitumumab continued LUMAKRAS single agent therapy after discontinuing panitumumab.
The major efficacy outcome measure was progression-free survival (PFS) as evaluated by BICR according to RECIST 1.1. Additional efficacy outcome measures included overall survival (OS), overall response rate (ORR), and duration of response (DOR). Only the results of the approved dosing regimen LUMAKRAS 960 mg in combination with panitumumab are described below.
Of the 107 patients randomized to either LUMAKRAS 960 mg once daily in combination with panitumumab or the control arms, the median age was 64 years (range: 34-81 years); 46% were age 65 years or older; 50% were female; 74% were White; 17% were Asian and 97% of the patients had ECOG PS 0 or 1. The primary site of disease was colon (69%) or rectum (31%). The median number of prior lines of therapy for metastatic disease was 2. Among the 107 patients, 100% received prior fluoropyrimidine, 99% received prior oxaliplatin, 93% received prior irinotecan and 18% of patients had received prior trifluridine and tipiracil, or regorafenib.
The trial demonstrated a statistically significant improvement in PFS for patients randomized to LUMAKRAS 960 mg in combination with panitumumab compared to the investigator's choice SOC. The final analysis of OS was not statistically significant.
The final analysis of PFS for patients randomized to LUMAKRAS 240 mg in combination with panitumumab compared to investigator's choice of SOC was not statistically significant.
The efficacy results from CodeBreaK 300 are summarized in Table 8 and Figure 1.
| Efficacy Parameters | Sotorasib 960 mg QD + Panitumumab (N = 53) |
SOC (trifluridine/tipiracil or regorafenib) (N = 54) |
|---|---|---|
| N = Number of randomized subjects, NR = Not Reached, QD = once daily, SOC = standard of care, CR = complete response, PR = partial response, BICR = Blinded Independent Central Review Committee, CI = Confidence Interval |
||
| Progression-Free Survival (PFS) per BICR | ||
| Number of Events (%) | 32 (60) | 35 (65) |
| Median in months (95% CI) | 5.6 (4.2, 6.3) | 2 (1.9, 3.9) |
| Hazard ratio (95% CI) Hazard ratios and 95% CIs were estimated using a stratified Cox proportional hazards model.
|
0.48 (0.3,0.78) | |
| p-value (2-sided) p-value was calculated using a stratified log-rank test.
|
0.005 | |
|
Overall Survival (OS)
OS analysis was based on 6-month additional follow-up data from the time of PFS primary analysis.
|
||
| Deaths (%) | 24 (45) | 30 (56) |
| Median in months (95% CI) | NR (8.6, NR) | 10.3 (7, NR) |
| Hazard ratio (95% CI) | 0.7 (0.41, 1.18) | |
| Overall Response Rate (ORR) per BICR | ||
| ORR, % (95% CI) 95% CIs were estimated using the Clopper-Pearson method.
|
26 (15, 40) | 0 (0, 7) |
| CR, n (%) | 1 (1.9) | 0 |
| PR, n (%) | 13 (25) | 0 |
| Duration of Response (DOR) | ||
| Median in months, (range) For DOR + indicates censored subjects.
|
4.4 (1.9+, 6+) | - |
| Figure 1. Kaplan-Meier Curve for Progression-Free Survival in CodeBreaK 300 |
|---|
1.2 Kras G12c Mutated Metastatic Colorectal Cancer (mcrc)
LUMAKRAS, in combination with panitumumab, is indicated for the treatment of adult patients with KRAS G12C-mutated metastatic colorectal cancer (mCRC), as determined by an FDA-approved test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy [see Dosage and Administration (2.1) and Clinical Studies (14.2)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been performed with sotorasib.
Sotorasib was not mutagenic in an in vitro bacterial reverse mutation (Ames) assay and was not genotoxic in the in vivo rat micronucleus and comet assays.
Fertility/early embryonic development studies were not conducted with sotorasib. There were no adverse effects on female or male reproductive organs in general toxicology studies conducted in dogs and rats.
2.4 Coadministration of Lumakras With Acid Reducing Agents
Avoid coadministration of proton pump inhibitors (PPIs) and H2 receptor antagonists with LUMAKRAS. If treatment with an acid-reducing agent cannot be avoided, take LUMAKRAS 4 hours before or 10 hours after administration of a local antacid [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
Principal Display Panel 240 Mg Tablet Bottle Carton Label
NDC 55513-512-60
LUMAKRAS®
(sotorasib) TABLETS
240 mg | New strength
Each tablet contains 240 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F).
Excursions permitted from 15°C to 30°C
(59°F to 86°F).
Recommended Dosage: See Prescribing
Information.
AMGEN®
Principal Display Panel 320 Mg Tablet Bottle Carton Label
NDC 55513-504-50
LUMAKRAS®
(sotorasib) TABLETS
320 mg | New strength
Each tablet contains 320 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F).
Excursions permitted from 15°C to 30°C
(59°F to 86°F).
Recommended Dosage: See Prescribing
Information.
AMGEN®
Principal Display Panel 120 Mg Tablet Bottle Carton Label Ndc 55513 488 02
NDC 55513-488-02
LUMAKRAS™
(sotorasib) TABLETS
120 mg
Each tablet contains 120 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F). Excursions
permitted from 15°C to 30°C (59°F to 86°F).
Recommended Dosage: See Prescribing Information.
AMGEN®
Principal Display Panel 120 Mg Tablet Bottle Carton Label Ndc 55513 488 24
NDC 55513-488-24
LUMAKRAS™
(sotorasib) TABLETS
120 mg
Each tablet contains 120 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F).
Excursions permitted from 15°C to 30°C
(59°F to 86°F).
Recommended Dosage: See Prescribing
Information.
AMGEN®
14.1 Kras G12c Mutated Locally Advanced Or Metastatic Non Small Cell Lung Cancer
The efficacy of LUMAKRAS was demonstrated in a subset of patients enrolled in a single-arm, open-label, multicenter trial (CodeBreaK 100 [NCT03600883]). Eligible patients were required to have locally advanced or metastatic KRAS G12C-mutated NSCLC with disease progression after receiving an immune checkpoint inhibitor and/or platinum-based chemotherapy, an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1, and at least one measurable lesion as defined by Response Evaluation Criteria in Solid Tumors (RECIST v1.1).
All patients were required to have prospectively identified KRAS G12C-mutated NSCLC in tumor tissue samples by using the QIAGEN therascreen ® KRAS RGQ PCR Kit performed in a central laboratory. Of 126 total enrolled subjects, 2 (2%) were unevaluable for efficacy analysis due to the absence of radiographically measurable lesions at baseline. Of the 124 patients with KRAS G12C mutations confirmed in tumor tissue, plasma samples from 112 patients were tested retrospectively using the Guardant360® CDx. 78/112 patients (70%) had KRAS G12C mutation identified in plasma specimen, 31/112 patients (28%) did not have KRAS G12C mutation identified in plasma specimen and 3/112 (2%) were unevaluable due to Guardant360® CDx test failure.
A total of 124 patients had at least one measurable lesion at baseline assessed by Blinded Independent Central Review (BICR) according to RECIST v1.1 and were treated with LUMAKRAS 960 mg once daily until disease progression or unacceptable toxicity. The major efficacy outcome measures were objective response rate (ORR), and duration of response (DOR) as evaluated by BICR according to RECIST v1.1.
The baseline demographic and disease characteristics of the study population were: median age 64 years (range: 37 to 80) with 48% ≥ 65 years and 8% ≥ 75 years; 50% Female; 82% White, 15% Asian, 2% Black; 70% ECOG PS 1; 96% had stage IV disease; 99% with non-squamous histology; 81% former smokers, 12% current smokers, 5% never smokers. All patients received at least 1 prior line of systemic therapy for metastatic NSCLC; 43% received only 1 prior line of therapy, 35% received 2 prior lines of therapy, 23% received 3 prior lines of therapy; 91% received prior anti-PD-1/PD-L1 immunotherapy, 90% received prior platinum-based chemotherapy, 81% received both platinum-based chemotherapy and anti-PD-1/PD-L1. The sites of known extra-thoracic metastasis included 48% bone, 21% brain, and 21% liver.
Efficacy results are summarized in Table 7.
| Efficacy Parameter | LUMAKRAS N = 124 |
|---|---|
| CI = confidence interval | |
|
Objective Response Rate (95% CI)
Assessed by Blinded Independent Central Review (BICR).
|
36 (28, 45) |
| Complete response rate, % | 2 |
| Partial response rate, % | 35 |
| Duration of Response | |
| Median Estimate using Kaplan-Meier method. , months (range) |
10 (1.3+, 11.1) |
| Patients with duration ≥ 6 months Observed proportion of patients with duration of response beyond landmark time. , % |
58% |
1.1 Kras G12c Mutated Locally Advanced Or Metastatic Non Small Cell Lung Cancer (nsclc)
LUMAKRAS as a single agent is indicated for the treatment of adult patients with KRAS G12C-mutated locally advanced or metastatic non-small cell lung cancer (NSCLC), as determined by an FDA-approved test [see Dosage and Administration (2.1)], who have received at least one prior systemic therapy.
This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DOR) [see Clinical Studies (14.1)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s).
Structured Label Content
Section 42229-5 (42229-5)
KRAS G12C-mutated Locally Advanced or Metastatic NSCLC
Select patients for treatment of locally advanced or metastatic NSCLC with LUMAKRAS based on the presence of KRAS G12C mutation in tumor or plasma specimens. If no mutation is detected in a plasma specimen, test tumor tissue [see Clinical Studies (14.1)].
Section 42230-3 (42230-3)
| PATIENT INFORMATION LUMAKRAS® (loo-ma-krass) (sotorasib) tablets |
||
|---|---|---|
| What is LUMAKRAS? | ||
LUMAKRAS is a prescription medicine used in adults:
It is not known if LUMAKRAS is safe and effective in children. What should I tell my healthcare provider before taking LUMAKRAS? |
||
Before taking LUMAKRAS, tell your healthcare provider about all your medical conditions, including if you:
Especially tell your healthcare provider if you take antacid medicines, including Proton Pump Inhibitor (PPI) medicines or H2 blockers during treatment with LUMAKRAS. Ask your healthcare provider if you are not sure. How should I take LUMAKRAS? |
||
|
||
LUMAKRAS may cause serious side effects, including:
|
||
|
|
|
|
||
| Your healthcare provider may change your dose, temporarily stop, or permanently stop treatment with LUMAKRAS if you develop side effects. The most common side effects of LUMAKRAS when used alone for NSCLC include: |
||
|
|
|
| The most common side effects of LUMAKRAS when used in combination with panitumumab for CRC include: | ||
|
|
|
| These are not all the possible side effects of LUMAKRAS. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. You may also report side effects to Amgen at 1-800-772-6436 (1-800-77-AMGEN). How should I store LUMAKRAS? |
||
General information about the safe and effective use of LUMAKRAS. |
||
| Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use LUMAKRAS for a condition for which it was not prescribed. Do not give LUMAKRAS to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about LUMAKRAS that is written for healthcare professionals. What are the ingredients in LUMAKRAS? |
||
|
Active Ingredient: sotorasib Inactive Ingredients: microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, and magnesium stearate. Tablet film coating material contains polyvinyl alcohol, titanium dioxide, polyethylene glycol, talc, iron oxide yellow and iron oxide red (320 mg tablet only). |
||
| Manufactured by: Amgen Inc., One Amgen Center Drive, Thousand Oaks, CA 91320-1799 U.S.A. © 2021, 2023, 2025 Amgen Inc. All rights reserved. For more information, go to www.LUMAKRAS.com or call 1-800-772-6436 (1-800-77-AMGEN). This Patient Information has been approved by the U.S. Food and Drug Administration. |
Revised: 01/2025 | |
| [part number] v3 |
Section 43683-2 (43683-2)
Section 44425-7 (44425-7)
Storage and Handling
Store at 20°C to 25°C (68°F to 77°F). Excursions permitted from 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
11 Description (11 DESCRIPTION)
Sotorasib is an inhibitor of the RAS GTPase family. The molecular formula is C30H30F2N6O3, and the molecular weight is 560.6 g/mol. The chemical name of sotorasib is 6-fluoro-7-(2-fluoro-6-hydroxyphenyl)-(1M)-1-[4-methyl-2-(propan-2-yl)pyridin-3-yl]-4-[(2S)-2-methyl-4-(prop-2-enoyl)piperazin-1-yl]pyrido[2,3-d]pyrimidin-2(1H)-one.
The chemical structure of sotorasib is shown below:
Sotorasib has pKa values of 8.06 and 4.56. The solubility of sotorasib in the aqueous media decreases over the range pH 1.2 to 6.8 from 1.3 mg/mL to 0.03 mg/mL.
LUMAKRAS is supplied as film-coated tablets for oral use containing 320 mg, 240 mg or 120 mg of sotorasib. Inactive ingredients in the tablet core are microcrystalline cellulose, lactose monohydrate, croscarmellose sodium, and magnesium stearate. The film coating material consists of polyvinyl alcohol, titanium dioxide, polyethylene glycol, talc, iron oxide yellow and iron oxide red (320 mg tablet only).
8.4 Pediatric Use
The safety and effectiveness of LUMAKRAS have not been established in pediatric patients.
8.5 Geriatric Use
Of the 357 patients with any tumor type who received LUMAKRAS 960 mg orally once daily in CodeBreaK 100, 46% were 65 and over, and 10% were 75 and over. No overall differences in safety or effectiveness were observed between older patients and younger patients treated with LUMAKRAS as a single agent.
In a pooled analysis of 132 patients who received LUMAKRAS 960 mg in combination with panitumumab for KRAS G12C-mutated mCRC, 30% were 65 and over while 9% were 75 and over. No overall differences in safety or efficacy were observed between older patients (≥ 65 years of age) compared to younger patients, treated with LUMAKRAS 960 mg in combination with panitumumab.
5.1 Hepatotoxicity
LUMAKRAS can cause hepatotoxicity and increased alanine aminotransferase (ALT) or increased aspartate aminotransferase (AST) which may lead to drug-induced liver injury and hepatitis.
In the pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg [see Adverse Reactions (6.1)], hepatotoxicity occurred in 27% of patients, of which 16% were Grade ≥ 3. Among patients with hepatotoxicity who required dosage modifications, 64% required treatment with corticosteroids.
In this pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg, 17% of patients who received LUMAKRAS had increased ALT/increased AST; of which 9% were Grade ≥ 3. The median time to first onset of increased ALT/AST was 6.3 weeks (range: 0.4 to 42). Increased ALT/AST leading to dose interruption or reduction occurred in 9% of patients treated with LUMAKRAS. LUMAKRAS was permanently discontinued due to increased ALT/AST in 2.7% of patients. Drug-induced liver injury occurred in 1.6% (all grades) including 1.3% (Grade ≥ 3).
In this pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg, a total of 40% patients with recent (≤ 3 months) immunotherapy prior to starting LUMAKRAS had an event of hepatotoxicity. An event of hepatotoxicity was observed in 18% of patients who started LUMAKRAS more than 3 months after last dose of immunotherapy and in 17% of those who never received immunotherapy. Regardless of time from prior immunotherapy, 94% of hepatotoxicity events improved or resolved with dosage modification of LUMAKRAS, with or without corticosteroid treatment.
In the pooled safety population of patients with CRC who received LUMAKRAS 960 mg in combination with panitumumab [see Adverse Reactions (6.1)], hepatotoxicity occurred in 15% of patients, of which 4.8% were Grade 3. A total of 7% of patients who received LUMAKRAS had increased ALT or increased AST, of which 0.8% were Grade 3. The median time to first onset of increased ALT or increased AST was 10 weeks (range: 2 to 22). Increased ALT or increased AST leading to dose interruption occurred in 2.4% of patients. A total of 3.2% of patients who received LUMAKRAS had hyperbilirubinemia, of which 2.4% were Grade 3. The median time to first onset of hyperbilirubinemia was 12 weeks (range: 0, 29). Hyperbilirubinemia leading to dose interruption occurred in 1.6% of patients. Among patients with hepatotoxicity, 21% received corticosteroids.
Monitor liver function tests (ALT, AST, alkaline phosphatase and total bilirubin) prior to the start of LUMAKRAS, every 3 weeks for the first 3 months of treatment, then once a month or as clinically indicated, with more frequent testing in patients who develop transaminase and/or bilirubin elevations. Withhold, reduce the dose or permanently discontinue LUMAKRAS based on severity of the adverse reaction [see Dosage and Administration (2.3) and Adverse Reactions (6.1)]. Consider administering systemic corticosteroids for the management of hepatotoxicity.
4 Contraindications (4 CONTRAINDICATIONS)
None.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are discussed in greater detail in other sections of the labeling:
- Hepatotoxicity [see Warnings and Precautions (5.1)]
- Interstitial Lung Disease (ILD)/Pneumonitis [see Warnings and Precautions (5.2)]
7 Drug Interactions (7 DRUG INTERACTIONS)
- Acid-Reducing Agents: Avoid coadministration with proton pump inhibitors (PPIs) and H2 receptor antagonists. If an acid-reducing agent cannot be avoided, administer LUMAKRAS 4 hours before or 10 hours after a local antacid. (2.4, 7.1)
- Strong CYP3A4 Inducers: Avoid coadministration with strong CYP3A4 inducers. (7.1)
- CYP3A4 Substrates: Avoid coadministration with CYP3A4 substrates for which minimal concentration changes may lead to therapeutic failures of the substrate. If coadministration cannot be avoided, adjust the substrate dosage in accordance to its Prescribing Information. (7.2)
- P-gp substrates: Avoid coadministration with P-gp substrates for which minimal concentration changes may lead to serious toxicities. If coadministration cannot be avoided, decrease the substrate dosage in accordance to its Prescribing Information. (7.2)
12.2 Pharmacodynamics
Sotorasib exposure-response relationships and the time course of the pharmacodynamic response are unknown.
12.3 Pharmacokinetics
The pharmacokinetics of sotorasib have been characterized in healthy subjects and in patients with KRAS G12C-mutated solid tumors, including NSCLC. Sotorasib exhibited non-linear, time-dependent, pharmacokinetics over the dose range of 180 mg to 960 mg (0.19 to 1 time the approved recommended dosage) once daily with similar systemic exposure (i.e., AUC0-24h and Cmax) across doses at steady state. Sotorasib systemic exposure was comparable between film-coated tablets and film-coated tablets predispersed in water administered under fasted conditions. Sotorasib plasma concentrations reached steady state within 22 days. No accumulation was observed after repeat LUMAKRAS dosages with a mean accumulation ratio of 0.56 (coefficient of variation (CV): 59%).
8.6 Hepatic Impairment
No dosage modification is recommended in patients with mild to moderate hepatic impairment (Child-Pugh A or B).
The effect of severe hepatic impairment (Child-Pugh C) on the safety of LUMAKRAS is unknown. Monitor for sotorasib adverse reactions in patients with hepatic impairment more frequently since these patients may be at increased risk for adverse reactions including hepatotoxicity [see Clinical Pharmacology (12.3)].
1 Indications and Usage (1 INDICATIONS AND USAGE)
LUMAKRAS is an inhibitor of the RAS GTPase family indicated for:
KRAS G12C-mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer (NSCLC)
- As a single agent, for the treatment of adult patients with KRAS G12C-mutated locally advanced or metastatic NSCLC, as determined by an FDA-approved test, who have received at least one prior systemic therapy. (1.1)
This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DOR). Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). (1.1)
KRAS G12C-mutated Metastatic Colorectal Cancer (mCRC)
In combination with panitumumab, for the treatment of adult patients with KRAS G12C-mutated mCRC as determined by an FDA approved-test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy. (1.2)
12.1 Mechanism of Action
Sotorasib is an inhibitor of KRAS G12C, a tumor-restricted, mutant-oncogenic form of the RAS GTPase, KRAS. Sotorasib forms an irreversible, covalent bond with the unique cysteine of KRAS G12C, locking the protein in an inactive state that prevents downstream signaling without affecting wild-type KRAS. Sotorasib blocked KRAS signaling, inhibited cell growth, and promoted apoptosis only in KRAS G12C tumor cell lines. Sotorasib inhibited KRAS G12C in vitro and in vivo with minimal detectable off-target activity. In mouse tumor xenograft models, sotorasib-treatment led to tumor regressions and prolonged survival, and was associated with anti-tumor immunity in KRAS G12C models.
In the setting of KRAS G12C-mutant CRC, epidermal growth factor receptor (EGFR) activation has been identified as a mechanism of resistance to KRAS G12C inhibition. In a murine patient-derived colorectal tumor xenograft model, the combination of sotorasib and panitumumab, an EGFR antagonist, had increased antitumor activity compared to either sotorasib or panitumumab alone.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Hepatotoxicity: Monitor liver function tests every 3 weeks for the first 3 months of treatment then once monthly as clinically indicated. Consider administering systemic corticosteroids and withhold, reduce the dose, or permanently discontinue LUMAKRAS based on the severity. (2.3, 5.1)
- Interstitial Lung Disease (ILD)/Pneumonitis: Monitor for new or worsening pulmonary symptoms. Immediately withhold LUMAKRAS for suspected ILD/pneumonitis and permanently discontinue if no other potential causes of ILD/pneumonitis are identified. (2.3, 5.2)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Tablets: 320 mg, beige, oval-shaped, immediate release, film-coated, debossed with "AMG" on one side and "320" on the opposite side.
Tablets: 240 mg, yellow, oval-shaped, immediate release, film-coated, debossed with "AMG" on one side and "240" on the opposite side.
Tablets: 120 mg, yellow, oblong-shaped, immediate release, film-coated, debossed with "AMG" on one side and "120" on the opposite side.
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
Lactation: Advise not to breastfeed. (8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The pooled safety population described in the WARNINGS AND PRECAUTIONS reflect exposure to LUMAKRAS as a single agent at 960 mg orally once daily until disease progression or unacceptable toxicity in 549 patients with NSCLC with KRAS G12C mutation in the following trials: CodeBreaK 200 (NCT04303780), CodeBreaK 100 (NCT03600883), CodeBreaK 101 (NCT04185883) and CodeBreaK 105 (NCT04380753). Among these 549 patients who received LUMAKRAS, 44% were exposed for 6 months or longer and 21% were exposed for greater than one year.
The pooled safety population described in WARNINGS AND PRECAUTIONS also reflects exposure to LUMAKRAS 960 mg once daily in combination with panitumumab in 126 patients who received LUMAKRAS in combination with panitumumab for mCRC in CodeBreaK 300 (NCT05198934) and CodeBreaK 101 (NCT04185883). Among the 126 patients who received LUMAKRAS 960 mg in combination with panitumumab, 40% were exposed for 6 months or longer and 10% were exposed for greater than one year.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise the patient to read the FDA-approved patient labeling (Patient Information).
13.2 Animal Toxicology And/or Pharmacology (13.2 Animal Toxicology and/or Pharmacology)
In rats, renal toxicity including minimal to marked histologic tubular degeneration/necrosis and increased kidney weight, urea nitrogen, creatinine, and urinary biomarkers of renal tubular injury were present at doses resulting in exposures approximately ≥ 0.5 times the human AUC at the clinical dose of 960 mg. Increases in cysteine S-conjugate β-lyase pathway metabolism in the rat kidney compared to human may make rats more susceptible to renal toxicity due to local formation of a putative sulfur-containing metabolite than humans.
In the 3-month toxicology study in dogs, sotorasib induced findings in the liver (centrilobular hepatocellular hypertrophy), pituitary gland (hypertrophy of basophils), and thyroid gland (marked follicular cell atrophy, moderate to marked colloid depletion, and follicular cell hypertrophy) at exposures approximately 0.4 times the human exposure based on AUC at the clinical dose of 960 mg. These findings may be due to an adaptive response to hepatocellular enzyme induction and subsequent reduced thyroid hormone levels (i.e., secondary hypothyroidism). Although thyroid levels were not measured in dogs, induction of uridine diphosphate glucuronosyltransferase known to be involved in thyroid hormone metabolism was confirmed in the in vitro dog hepatocyte assay.
2.3 Dosage Modifications for Adverse Reactions
LUMAKRAS dose reduction levels are summarized in Table 1.
If adverse reactions occur, a maximum of two dose reductions are permitted. Discontinue LUMAKRAS if patients are unable to tolerate the minimum dose of 240 mg once daily.
When LUMAKRAS is administered in combination with panitumumab, and LUMAKRAS is temporarily withheld or permanently discontinued, temporarily withhold or permanently discontinue panitumumab, respectively [see Clinical Studies (14.2)]. Refer to the full prescribing information of panitumumab for dose modifications for adverse reactions associated with the use of panitumumab.
Treatment with LUMAKRAS as a single agent may be continued if panitumumab is permanently discontinued [see Clinical Pharmacology (12.1), Clinical Studies (14.2)].
Refer to Table 2 for dose modification guidelines and management of adverse reactions associated with the use of LUMAKRAS as a single agent or as combination therapy with panitumumab.
| Dose Reduction Level | Dose |
|---|---|
| First dose reduction | 480 mg (two 240 mg or four 120 mg tablets) once daily |
| Second dose reduction | 240 mg (one 240 mg or two 120 mg tablets) once daily |
| Adverse Reaction | Severity
Grading defined by National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 5.0.
|
Dosage Modification When LUMAKRAS is administered in combination with panitumumab, withhold or permanently discontinue treatment with panitumumab when withholding or permanently discontinuing treatment with LUMAKRAS.
|
|---|---|---|
| ALT = alanine aminotransferase; AST = aspartate aminotransferase; ULN = upper limit of normal | ||
| Hepatotoxicity [see Warnings and Precautions (5.1)] | AST or ALT > 3 × and up to 5 × ULN (or > 3 × and up to 5 × baseline if baseline abnormal) with symptoms or AST or ALT > 5 × ULN (or > 5 × baseline if baseline abnormal) |
|
| AST or ALT > 3 × ULN with total bilirubin > 2 × ULN |
|
|
| Interstitial Lung Disease (ILD)/ pneumonitis [see Warnings and Precautions (5.2)] | Any Grade |
|
| Nausea or vomiting despite appropriate supportive care (including anti-emetic therapy) [see Adverse Reactions (6.1)] |
Grade 3 to 4 |
|
| Diarrhea despite appropriate supportive care (including anti-diarrheal therapy) [see Adverse Reactions (6.1)] |
Grade 3 to 4 |
|
| Other adverse reactions [see Adverse Reactions (6.1)] |
Grade 3 to 4 |
|
5.2 Interstitial Lung Disease (ild)/pneumonitis (5.2 Interstitial Lung Disease (ILD)/Pneumonitis)
LUMAKRAS can cause ILD/pneumonitis that can be fatal.
In the pooled safety population of patients with NSCLC who received single agent LUMAKRAS 960 mg [see Adverse Reactions (6.1)], ILD/pneumonitis occurred in 2.2% of patients, of which 1.1% were Grade ≥ 3, and 1 case was fatal. The median time to first onset for ILD/pneumonitis was 8.6 weeks (range: 2.1 to 36.7 weeks). LUMAKRAS was permanently discontinued due to ILD/pneumonitis in 1.3% of LUMAKRAS-treated patients. Monitor patients for new or worsening pulmonary symptoms indicative of ILD/pneumonitis (e.g., dyspnea, cough, fever). Immediately withhold LUMAKRAS in patients with suspected ILD/pneumonitis and permanently discontinue LUMAKRAS if no other potential causes of ILD/pneumonitis are identified [see Dosage and Administration (2.3) and Adverse Reactions (6.1)].
In the pooled safety population of patients with CRC who received LUMAKRAS 960 mg in combination with panitumumab, 1 patient experienced a Grade 1 event of ILD/pneumonitis [see Adverse Reactions (6.1)].
14.2 Kras G12c Mutated Metastatic Colorectal Cancer (14.2 KRAS G12C-mutated Metastatic Colorectal Cancer)
The efficacy of LUMAKRAS in combination with panitumumab was evaluated in CodeBreaK 300 [NCT05198934], a multicenter, randomized, open-label, active-controlled study conducted in previously treated patients with KRAS G12C-mutated mCRC. Key eligibility criteria included patients 18 years of age or older, who had received at least one prior line of therapy for mCRC, and who had received fluoropyrimidine, oxaliplatin, and irinotecan for metastatic disease unless there was a medical contraindication.
All patients were also required to have prospectively identified KRAS G12C-mutated mCRC in tumor tissue samples by using the QIAGEN therascreen® KRAS RGQ PCR Kit performed in a central laboratory. Other eligibility criteria included an ECOG PS of ≤ 2 and at least one measurable lesion as defined by RECIST v1.1.
A total of 160 patients with previously treated mCRC with the KRAS G12C mutation were randomized 1:1:1 to receive either LUMAKRAS 960 mg orally once daily and panitumumab 6 mg/kg IV every 2 weeks (N = 53), or LUMAKRAS 240 mg orally once daily and panitumumab 6 mg/kg IV every 2 weeks (N = 53), or investigator's choice of SOC trifluridine/tipiracil or regorafenib (N = 54). Randomization was stratified by prior anti-angiogenic therapy (yes or no), time from initial diagnosis of metastatic disease to randomization (≥ 18 months; < 18 months), and ECOG status (0 or 1 versus 2). Patients received treatment until disease progression, lack of clinical benefit or intolerance to treatment. LUMAKRAS discontinuation required panitumumab discontinuation, however, patients could continue to receive LUMAKRAS if panitumumab was discontinued [see Dosage and Administration (2.3)]. Four patients randomized to LUMAKRAS 960 mg in combination with panitumumab continued LUMAKRAS single agent therapy after discontinuing panitumumab.
The major efficacy outcome measure was progression-free survival (PFS) as evaluated by BICR according to RECIST 1.1. Additional efficacy outcome measures included overall survival (OS), overall response rate (ORR), and duration of response (DOR). Only the results of the approved dosing regimen LUMAKRAS 960 mg in combination with panitumumab are described below.
Of the 107 patients randomized to either LUMAKRAS 960 mg once daily in combination with panitumumab or the control arms, the median age was 64 years (range: 34-81 years); 46% were age 65 years or older; 50% were female; 74% were White; 17% were Asian and 97% of the patients had ECOG PS 0 or 1. The primary site of disease was colon (69%) or rectum (31%). The median number of prior lines of therapy for metastatic disease was 2. Among the 107 patients, 100% received prior fluoropyrimidine, 99% received prior oxaliplatin, 93% received prior irinotecan and 18% of patients had received prior trifluridine and tipiracil, or regorafenib.
The trial demonstrated a statistically significant improvement in PFS for patients randomized to LUMAKRAS 960 mg in combination with panitumumab compared to the investigator's choice SOC. The final analysis of OS was not statistically significant.
The final analysis of PFS for patients randomized to LUMAKRAS 240 mg in combination with panitumumab compared to investigator's choice of SOC was not statistically significant.
The efficacy results from CodeBreaK 300 are summarized in Table 8 and Figure 1.
| Efficacy Parameters | Sotorasib 960 mg QD + Panitumumab (N = 53) |
SOC (trifluridine/tipiracil or regorafenib) (N = 54) |
|---|---|---|
| N = Number of randomized subjects, NR = Not Reached, QD = once daily, SOC = standard of care, CR = complete response, PR = partial response, BICR = Blinded Independent Central Review Committee, CI = Confidence Interval |
||
| Progression-Free Survival (PFS) per BICR | ||
| Number of Events (%) | 32 (60) | 35 (65) |
| Median in months (95% CI) | 5.6 (4.2, 6.3) | 2 (1.9, 3.9) |
| Hazard ratio (95% CI) Hazard ratios and 95% CIs were estimated using a stratified Cox proportional hazards model.
|
0.48 (0.3,0.78) | |
| p-value (2-sided) p-value was calculated using a stratified log-rank test.
|
0.005 | |
|
Overall Survival (OS)
OS analysis was based on 6-month additional follow-up data from the time of PFS primary analysis.
|
||
| Deaths (%) | 24 (45) | 30 (56) |
| Median in months (95% CI) | NR (8.6, NR) | 10.3 (7, NR) |
| Hazard ratio (95% CI) | 0.7 (0.41, 1.18) | |
| Overall Response Rate (ORR) per BICR | ||
| ORR, % (95% CI) 95% CIs were estimated using the Clopper-Pearson method.
|
26 (15, 40) | 0 (0, 7) |
| CR, n (%) | 1 (1.9) | 0 |
| PR, n (%) | 13 (25) | 0 |
| Duration of Response (DOR) | ||
| Median in months, (range) For DOR + indicates censored subjects.
|
4.4 (1.9+, 6+) | - |
| Figure 1. Kaplan-Meier Curve for Progression-Free Survival in CodeBreaK 300 |
|---|
1.2 Kras G12c Mutated Metastatic Colorectal Cancer (mcrc) (1.2 KRAS G12C-mutated Metastatic Colorectal Cancer (mCRC))
LUMAKRAS, in combination with panitumumab, is indicated for the treatment of adult patients with KRAS G12C-mutated metastatic colorectal cancer (mCRC), as determined by an FDA-approved test, who have received prior fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy [see Dosage and Administration (2.1) and Clinical Studies (14.2)].
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been performed with sotorasib.
Sotorasib was not mutagenic in an in vitro bacterial reverse mutation (Ames) assay and was not genotoxic in the in vivo rat micronucleus and comet assays.
Fertility/early embryonic development studies were not conducted with sotorasib. There were no adverse effects on female or male reproductive organs in general toxicology studies conducted in dogs and rats.
2.4 Coadministration of Lumakras With Acid Reducing Agents (2.4 Coadministration of LUMAKRAS with Acid-Reducing Agents)
Avoid coadministration of proton pump inhibitors (PPIs) and H2 receptor antagonists with LUMAKRAS. If treatment with an acid-reducing agent cannot be avoided, take LUMAKRAS 4 hours before or 10 hours after administration of a local antacid [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
Principal Display Panel 240 Mg Tablet Bottle Carton Label (PRINCIPAL DISPLAY PANEL - 240 mg Tablet Bottle Carton Label)
NDC 55513-512-60
LUMAKRAS®
(sotorasib) TABLETS
240 mg | New strength
Each tablet contains 240 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F).
Excursions permitted from 15°C to 30°C
(59°F to 86°F).
Recommended Dosage: See Prescribing
Information.
AMGEN®
Principal Display Panel 320 Mg Tablet Bottle Carton Label (PRINCIPAL DISPLAY PANEL - 320 mg Tablet Bottle Carton Label)
NDC 55513-504-50
LUMAKRAS®
(sotorasib) TABLETS
320 mg | New strength
Each tablet contains 320 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F).
Excursions permitted from 15°C to 30°C
(59°F to 86°F).
Recommended Dosage: See Prescribing
Information.
AMGEN®
Principal Display Panel 120 Mg Tablet Bottle Carton Label Ndc 55513 488 02 (PRINCIPAL DISPLAY PANEL - 120 mg Tablet Bottle Carton Label - NDC 55513-488-02)
NDC 55513-488-02
LUMAKRAS™
(sotorasib) TABLETS
120 mg
Each tablet contains 120 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F). Excursions
permitted from 15°C to 30°C (59°F to 86°F).
Recommended Dosage: See Prescribing Information.
AMGEN®
Principal Display Panel 120 Mg Tablet Bottle Carton Label Ndc 55513 488 24 (PRINCIPAL DISPLAY PANEL - 120 mg Tablet Bottle Carton Label - NDC 55513-488-24)
NDC 55513-488-24
LUMAKRAS™
(sotorasib) TABLETS
120 mg
Each tablet contains 120 mg sotorasib.
Store at 20°C to 25°C (68°F to 77°F).
Excursions permitted from 15°C to 30°C
(59°F to 86°F).
Recommended Dosage: See Prescribing
Information.
AMGEN®
14.1 Kras G12c Mutated Locally Advanced Or Metastatic Non Small Cell Lung Cancer (14.1 KRAS G12C-mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer)
The efficacy of LUMAKRAS was demonstrated in a subset of patients enrolled in a single-arm, open-label, multicenter trial (CodeBreaK 100 [NCT03600883]). Eligible patients were required to have locally advanced or metastatic KRAS G12C-mutated NSCLC with disease progression after receiving an immune checkpoint inhibitor and/or platinum-based chemotherapy, an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 or 1, and at least one measurable lesion as defined by Response Evaluation Criteria in Solid Tumors (RECIST v1.1).
All patients were required to have prospectively identified KRAS G12C-mutated NSCLC in tumor tissue samples by using the QIAGEN therascreen ® KRAS RGQ PCR Kit performed in a central laboratory. Of 126 total enrolled subjects, 2 (2%) were unevaluable for efficacy analysis due to the absence of radiographically measurable lesions at baseline. Of the 124 patients with KRAS G12C mutations confirmed in tumor tissue, plasma samples from 112 patients were tested retrospectively using the Guardant360® CDx. 78/112 patients (70%) had KRAS G12C mutation identified in plasma specimen, 31/112 patients (28%) did not have KRAS G12C mutation identified in plasma specimen and 3/112 (2%) were unevaluable due to Guardant360® CDx test failure.
A total of 124 patients had at least one measurable lesion at baseline assessed by Blinded Independent Central Review (BICR) according to RECIST v1.1 and were treated with LUMAKRAS 960 mg once daily until disease progression or unacceptable toxicity. The major efficacy outcome measures were objective response rate (ORR), and duration of response (DOR) as evaluated by BICR according to RECIST v1.1.
The baseline demographic and disease characteristics of the study population were: median age 64 years (range: 37 to 80) with 48% ≥ 65 years and 8% ≥ 75 years; 50% Female; 82% White, 15% Asian, 2% Black; 70% ECOG PS 1; 96% had stage IV disease; 99% with non-squamous histology; 81% former smokers, 12% current smokers, 5% never smokers. All patients received at least 1 prior line of systemic therapy for metastatic NSCLC; 43% received only 1 prior line of therapy, 35% received 2 prior lines of therapy, 23% received 3 prior lines of therapy; 91% received prior anti-PD-1/PD-L1 immunotherapy, 90% received prior platinum-based chemotherapy, 81% received both platinum-based chemotherapy and anti-PD-1/PD-L1. The sites of known extra-thoracic metastasis included 48% bone, 21% brain, and 21% liver.
Efficacy results are summarized in Table 7.
| Efficacy Parameter | LUMAKRAS N = 124 |
|---|---|
| CI = confidence interval | |
|
Objective Response Rate (95% CI)
Assessed by Blinded Independent Central Review (BICR).
|
36 (28, 45) |
| Complete response rate, % | 2 |
| Partial response rate, % | 35 |
| Duration of Response | |
| Median Estimate using Kaplan-Meier method. , months (range) |
10 (1.3+, 11.1) |
| Patients with duration ≥ 6 months Observed proportion of patients with duration of response beyond landmark time. , % |
58% |
1.1 Kras G12c Mutated Locally Advanced Or Metastatic Non Small Cell Lung Cancer (nsclc) (1.1 KRAS G12C-mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer (NSCLC))
LUMAKRAS as a single agent is indicated for the treatment of adult patients with KRAS G12C-mutated locally advanced or metastatic non-small cell lung cancer (NSCLC), as determined by an FDA-approved test [see Dosage and Administration (2.1)], who have received at least one prior systemic therapy.
This indication is approved under accelerated approval based on overall response rate (ORR) and duration of response (DOR) [see Clinical Studies (14.1)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s).
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:45:21.970652 · Updated: 2026-03-14T22:22:19.833821