Lazcluze
c417f9ee-2027-4ed5-92ad-3c19266de16c
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
LAZCLUZE, in combination with amivantamab, is indicated for the first-line treatment of adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations, as detected by an FDA-approved test [see Dosage and Administration (2.1) ] .
Dosage and Administration
The recommended dosage of LAZCLUZE is 240 mg orally once daily with or without food, given in combination with amivantamab. ( 2.2 ) Continue treatment until disease progression or unacceptable toxicity. ( 2.2 ) Administer LAZCLUZE any time prior to amivantamab when given on the same day. ( 2.2 ) Refer to the amivantamab prescribing information for recommended amivantamab dosing information. ( 2.2 ) Administer prophylactic and concomitant medications to reduce the risk of dermatologic adverse reactions. ( 2.3 ) Administer anticoagulant prophylaxis to reduce the risk of venous thromboembolic events (VTE) for the first four months of treatment. ( 2.3 )
Contraindications
None.
Warnings and Precautions
Venous Thromboembolic Events (VTE): Prophylactic anticoagulation is recommended for the first four months of treatment. Monitor for signs and symptoms of VTE and treat as medically appropriate. Withhold LAZCLUZE and amivantamab based on severity. Once anticoagulant treatment has been initiated, resume LAZCLUZE and amivantamab at the same dose at the discretion of the healthcare provider. Permanently discontinue amivantamab and continue LAZCLUZE for recurrent VTE despite therapeutic anticoagulation. ( 2.3 , 2.4 , 5.1 ) Interstitial Lung Disease (ILD)/Pneumonitis : Monitor for new or worsening symptoms indicative of ILD/pneumonitis. Withhold LAZCLUZE and amivantamab in patients with suspected ILD/pneumonitis and permanently discontinue if ILD/pneumonitis is confirmed. ( 2.4 , 5.2 ) Dermatologic Adverse Reactions : Can cause severe rash including acneiform dermatitis. At treatment initiation, prophylactic and concomitant medications are recommended. Withhold, reduce the dose or permanently discontinue LAZCLUZE and amivantamab based on severity. ( 2.3 , 2.4 , 5.3 ) Ocular Adverse Reactions : Promptly refer patients with new or worsening signs and symptoms of ocular adverse reactions, including keratitis, to an ophthalmologist for evaluation. Withhold, reduce the dose, or permanently discontinue amivantamab and continue LAZCLUZE based on severity. ( 5.4 ) Embryo-Fetal Toxicity : Can cause fetal harm. Advise patients of reproductive potential of the potential risk to a fetus and to use effective contraception. ( 5.5 , 8.1 , 8.3 )
Adverse Reactions
The following adverse reactions are discussed elsewhere in the labeling: Venous Thromboembolic Events [see Warnings and Precautions (5.1) ] Interstitial Lung Disease/Pneumonitis [see Warnings and Precautions (5.2) ] Dermatologic Adverse Reactions [see Warnings and Precautions (5.3) ] Ocular Toxicity [see Warnings and Precautions (5.4) ]
Drug Interactions
Strong and moderate CYP3A4 inducers: Avoid concomitant use. ( 7.1 )
How Supplied
LAZCLUZE ® (lazertinib) tablets are available in the strengths and packages listed below: Tablet Strength Description Package Configuration NDC Number 80 mg Yellow, oval, film-coated, debossed with "LZ" on one side and "80" on the other side 60-count bottle NDC 57894-080-60 240 mg Reddish purple, oval, film-coated, debossed with "LZ" on one side and "240" on the other side 30-count bottle NDC 57894-240-30
Storage and Handling
LAZCLUZE ® (lazertinib) tablets are available in the strengths and packages listed below: Tablet Strength Description Package Configuration NDC Number 80 mg Yellow, oval, film-coated, debossed with "LZ" on one side and "80" on the other side 60-count bottle NDC 57894-080-60 240 mg Reddish purple, oval, film-coated, debossed with "LZ" on one side and "240" on the other side 30-count bottle NDC 57894-240-30
Description
Dosage and Administration ( 2.3 ) 11/2025 Warnings and Precautions ( 5.3 ) 11/2025
Medication Information
Warnings and Precautions
Venous Thromboembolic Events (VTE): Prophylactic anticoagulation is recommended for the first four months of treatment. Monitor for signs and symptoms of VTE and treat as medically appropriate. Withhold LAZCLUZE and amivantamab based on severity. Once anticoagulant treatment has been initiated, resume LAZCLUZE and amivantamab at the same dose at the discretion of the healthcare provider. Permanently discontinue amivantamab and continue LAZCLUZE for recurrent VTE despite therapeutic anticoagulation. ( 2.3 , 2.4 , 5.1 ) Interstitial Lung Disease (ILD)/Pneumonitis : Monitor for new or worsening symptoms indicative of ILD/pneumonitis. Withhold LAZCLUZE and amivantamab in patients with suspected ILD/pneumonitis and permanently discontinue if ILD/pneumonitis is confirmed. ( 2.4 , 5.2 ) Dermatologic Adverse Reactions : Can cause severe rash including acneiform dermatitis. At treatment initiation, prophylactic and concomitant medications are recommended. Withhold, reduce the dose or permanently discontinue LAZCLUZE and amivantamab based on severity. ( 2.3 , 2.4 , 5.3 ) Ocular Adverse Reactions : Promptly refer patients with new or worsening signs and symptoms of ocular adverse reactions, including keratitis, to an ophthalmologist for evaluation. Withhold, reduce the dose, or permanently discontinue amivantamab and continue LAZCLUZE based on severity. ( 5.4 ) Embryo-Fetal Toxicity : Can cause fetal harm. Advise patients of reproductive potential of the potential risk to a fetus and to use effective contraception. ( 5.5 , 8.1 , 8.3 )
Indications and Usage
LAZCLUZE, in combination with amivantamab, is indicated for the first-line treatment of adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations, as detected by an FDA-approved test [see Dosage and Administration (2.1) ] .
Dosage and Administration
The recommended dosage of LAZCLUZE is 240 mg orally once daily with or without food, given in combination with amivantamab. ( 2.2 ) Continue treatment until disease progression or unacceptable toxicity. ( 2.2 ) Administer LAZCLUZE any time prior to amivantamab when given on the same day. ( 2.2 ) Refer to the amivantamab prescribing information for recommended amivantamab dosing information. ( 2.2 ) Administer prophylactic and concomitant medications to reduce the risk of dermatologic adverse reactions. ( 2.3 ) Administer anticoagulant prophylaxis to reduce the risk of venous thromboembolic events (VTE) for the first four months of treatment. ( 2.3 )
Contraindications
None.
Adverse Reactions
The following adverse reactions are discussed elsewhere in the labeling: Venous Thromboembolic Events [see Warnings and Precautions (5.1) ] Interstitial Lung Disease/Pneumonitis [see Warnings and Precautions (5.2) ] Dermatologic Adverse Reactions [see Warnings and Precautions (5.3) ] Ocular Toxicity [see Warnings and Precautions (5.4) ]
Drug Interactions
Strong and moderate CYP3A4 inducers: Avoid concomitant use. ( 7.1 )
Storage and Handling
LAZCLUZE ® (lazertinib) tablets are available in the strengths and packages listed below: Tablet Strength Description Package Configuration NDC Number 80 mg Yellow, oval, film-coated, debossed with "LZ" on one side and "80" on the other side 60-count bottle NDC 57894-080-60 240 mg Reddish purple, oval, film-coated, debossed with "LZ" on one side and "240" on the other side 30-count bottle NDC 57894-240-30
How Supplied
LAZCLUZE ® (lazertinib) tablets are available in the strengths and packages listed below: Tablet Strength Description Package Configuration NDC Number 80 mg Yellow, oval, film-coated, debossed with "LZ" on one side and "80" on the other side 60-count bottle NDC 57894-080-60 240 mg Reddish purple, oval, film-coated, debossed with "LZ" on one side and "240" on the other side 30-count bottle NDC 57894-240-30
Description
Dosage and Administration ( 2.3 ) 11/2025 Warnings and Precautions ( 5.3 ) 11/2025
Section 42229-5
Recommended Dosage and Administration
The recommended dosage of LAZCLUZE is 240 mg orally once daily administered in combination with amivantamab, with or without food. Swallow LAZCLUZE tablets whole. Do not crush, split, or chew. Continue treatment until disease progression or unacceptable toxicity.
Administer LAZCLUZE any time prior to amivantamab when given on the same day. Refer to the amivantamab prescribing information for recommended amivantamab dosing information.
Section 42230-3
| This Patient Information has been approved by the U.S. Food and Drug Administration. | Revised: 11/2025 |
|
PATIENT INFORMATION
LAZCLUZE ® (laz-kluez) (lazertinib) tablets, for oral use |
|
|
What is LAZCLUZE?
LAZCLUZE in combination with amivantamab is a prescription medicine for the first-line treatment of adults with non-small cell lung cancer (NSCLC) that:
It is not known if LAZCLUZE is safe and effective in children. |
|
Before taking LAZCLUZE, tell your healthcare provider about all of your medical conditions, including if you:
LAZCLUZE may affect the way other medicines work, and other medicines may affect how LAZCLUZE works. You should not start or stop any medicine before you talk with your healthcare provider that prescribed LAZCLUZE. |
|
How should I take LAZCLUZE?
|
|
|
What should I avoid while taking LAZCLUZE?
|
|
|
What are the possible side effects of LAZCLUZE?
LAZCLUZE may cause serious side effects, including:
The most common side effects of LAZCLUZE in combination with amivantamab include: |
|
|
|
| LAZCLUZE may cause fertility problems in males and females, which may affect your ability to have children. Talk to your healthcare provider if this is a concern for you.
Your healthcare provider may temporarily stop, decrease your dose or completely stop your treatment with LAZCLUZE if you have serious side effects. These are not all of the possible side effects of LAZCLUZE. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
How should I store LAZCLUZE?
|
|
|
General information about the safe and effective use of LAZCLUZE.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use LAZCLUZE for a condition for which it was not prescribed. Do not give LAZCLUZE to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about LAZCLUZE that is written for health professionals. |
|
|
What are the ingredients in LAZCLUZE?
Active ingredient : lazertinib mesylate Inactive ingredients: croscarmellose sodium, magnesium stearate, mannitol, microcrystalline cellulose, and silica hydrophobic colloidal. The tablet coating consists of glycerol monocaprylocaprate type I, iron oxide black (in 240 mg strength tablets), iron oxide red (in 240 mg strength tablets), iron oxide yellow (in 80 mg strength tablets), macrogol (PEG) polyvinyl alcohol graft copolymer, polyvinyl alcohol-partially hydrolyzed, talc, and titanium dioxide. Product of Belgium Manufactured for: Janssen Biotech, Inc., Horsham, PA 19044, USA For patent information: www.janssenpatents.com © Johnson & Johnson and its affiliates 2024–2025 For more information, call 1-800-526-7736 or go to www.lazcluze.com |
Section 44425-7
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
11 Description
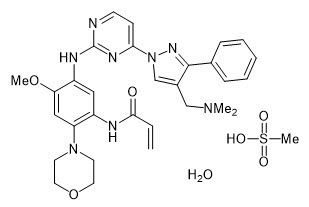
LAZCLUZE ®tablets contain lazertinib, a kinase inhibitor for oral use. Lazertinib is present as lazertinib mesylate hydrate with a molecular weight of 668.77 and molecular formula of C 30H 34N 8O 3∙CH 4O 3S∙H 2O. The chemical name is N-[5-[[4-[4-[(Dimethylamino)methyl]-3-phenyl-1 H-pyrazol-1-yl]pyrimidin-2-yl]amino]-4-methoxy-2-(morpholin-4-yl)phenyl]acrylamide methanesulfonate hydrate (1:1:1). Lazertinib mesylate hydrate is soluble or practically insoluble in aqueous media, and slightly soluble to freely soluble in organic solvents over a wide range of pH values. The structural formula is:
LAZCLUZE (lazertinib) film-coated tablets contain 80 mg or 240 mg of lazertinib, equivalent to 93.86 and 281.58 mg lazertinib mesylate (calculated on anhydrous basis), respectively. The inactive ingredients are croscarmellose sodium, magnesium stearate, mannitol, microcrystalline cellulose, and silica hydrophobic colloidal. The tablet coating consists of glycerol monocaprylocaprate type I, iron oxide black (in 240 mg strength tablets), iron oxide red (in 240 mg strength tablets), iron oxide yellow (in 80 mg strength tablets), macrogol (PEG) polyvinyl alcohol graft copolymer, polyvinyl alcohol-partially hydrolyzed, talc, and titanium dioxide.
8.4 Pediatric Use
The safety and effectiveness of LAZCLUZE in pediatric patients have not been established.
8.5 Geriatric Use
Of the 421 patients with locally advanced or metastatic NSCLC treated with LAZCLUZE in combination with amivantamab in MARIPOSA, 45% were 65 years and older and 12% were 75 years and older. No overall differences in safety or effectiveness were observed between patients aged 65 and older and younger patients.
14 Clinical Studies
The efficacy of LAZCLUZE, in combination with amivantamab, was evaluated in MARIPOSA [NCT04487080], a randomized, active-controlled, multicenter trial. Eligible patients were required to have untreated locally advanced or metastatic NSCLC with either exon 19 deletions or exon 21 L858R substitution EGFR mutations identified by local testing, not amenable to curative therapy. Patients with asymptomatic or previously treated and stable intracranial metastases were eligible to enroll.
Patients were randomized (2:2:1) to receive LAZCLUZE in combination with amivantamab (N=429), osimertinib monotherapy (N=429), or LAZCLUZE monotherapy (an unapproved regimen for NSCLC) until disease progression or unacceptable toxicity. The evaluation of efficacy for the treatment of untreated metastatic NSCLC relied upon comparison between:
- LAZCLUZE administered at 240 mg orally once daily in combination with amivantamab administered intravenously at 1050 mg (for patients < 80 kg) or 1400 mg (for patients ≥ 80 kg) once weekly for 4 weeks, then every 2 weeks thereafter starting at week 5.
- Osimertinib administered at a dose of 80 mg orally once daily.
Randomization was stratified by EGFR mutation type (exon 19 deletion or exon 21 L858R substitution mutation), Asian race (yes or no), and history of brain metastasis (yes or no). Tumor assessments were performed every 8 weeks for 30 months, and then every 12 weeks until disease progression.
The major efficacy outcome measure was progression-free survival (PFS) as assessed by blinded independent central review (BICR). Additional efficacy outcome measures included overall survival (OS), overall response rate (ORR) and duration of response (DOR).
A total of 858 patients were randomized between the two study arms, 429 to the LAZCLUZE in combination with amivantamab arm and 429 to the osimertinib arm. The median age was 63 (range: 25–88) years; 61% were female; 58% were Asian, and 38% were White, 1.6% were American Indian or Alaska Native, 0.8% were Black or African American, 0.2% were Native Hawaiian or other Pacific Islander, 0.6% were unknown race or multiple races; and 12% were Hispanic or Latino. Eastern Cooperative Oncology Group (ECOG) performance status was 0 (34%) or 1 (66%); 69% never smoked; 41% had prior brain metastases; and 89% had Stage IV cancer at initial diagnosis. Sixty percent of patients had tumors harboring exon 19 deletions and the remaining 40% had exon 21 L858R substitution mutations.
Among the 858 patients with EGFR exon 19 deletion or L858R substitution mutations that were randomized between the amivantamab plus LAZCLUZE arm versus the osimertinib arm, available tissue samples from 544 (63%) patients had evaluable results when tested retrospectively using the cobas EGFR Mutation Test v2. Of the 544 patients with evaluable results, 527 (97%) patients were positive for EGFR exon 19 deletion or L858R substitution mutations, while 17 (3%) patients were negative. Available plasma samples from patients were retrospectively tested using an FDA-approved test to confirm the biomarker status.
The trial demonstrated a statistically significant improvement in PFS by BICR assessment and OS for LAZCLUZE in combination with amivantamab compared to osimertinib (see Table 5and Figures 1and 2).
Efficacy results are provided in Table 5.
| LAZCLUZE in combination with amivantamab
(N=429) |
Osimertinib
(N=429) |
|
|---|---|---|
| CI = confidence interval; NR = not reached; NE = not estimable | ||
| Progression-free survival (PFS) | ||
| Number of events (%) | 192 (45) | 252 (59) |
| Median, months (95% CI) | 23.7 (19.1, 27.7) | 16.6 (14.8, 18.5) |
| HR
Stratified by mutation type (Exon 19del or Exon 21 L858R), prior brain metastases (yes or no), and Asian race (yes or no).
,
Stratified Cox proportional hazards regression. (95% CI); p-value
,
Stratified log-rank test.
|
0.70 (0.58, 0.85); p=0.0002 | |
| Overall survival (OS) | ||
| Number of events (%) | 173 (40) | 217 (51) |
| Median, months (95% CI) | NR (42.9, NE) | 36.7 (33.4, 41.0) |
| HR , (95% CI); p-value , | 0.75 (0.61, 0.92); p=0.0048 | |
| Overall response rate (ORR)
Confirmed responses based on the ITT population.
|
||
| ORR, % (95% CI) | 78 (74, 82) | 73 (69, 78) |
| Complete response, % | 5 | 3.5 |
| Partial response, % | 73 | 70 |
| Duration of response (DOR)
In confirmed responders.
|
||
| Median (95% CI), months | 25.8 (20.1, NE) | 16.7 (14.8, 18.5) |
| Patients with DOR ≥ 6 months
Based on observed rates. , %
|
86 | 85 |
| Patients with DOR ≥ 12 months , % | 68 | 57 |
Figure 1: Kaplan-Meier Curves of PFS by BICR Assessment in Patients with Previously Untreated NSCLC
Figure 2: Kaplan-Meier Curves of OS in Patients with Previously Untreated NSCLC
Out of all randomized patients (n=858), 367 (43%) had baseline intracranial lesions assessed by BICR using modified RECIST. Results of pre-specified analyses of intracranial ORR and DOR by BICR in the subset of patients with intracranial lesions at baseline for the LAZCLUZE in combination with amivantamab arm and the osimertinib arm are summarized in Table 6.
| LAZCLUZE in combination with amivantamab
(N=180) |
Osimertinib
(N=187) |
|
|---|---|---|
| CI = confidence interval | ||
| Intracranial Tumor Response Assessment | ||
| Intracranial ORR
Confirmed responses , % (95% CI)
|
68 (60, 75) | 69 (62, 76) |
| Complete response, % | 55 | 52 |
| Intracranial DOR
In confirmed responders
|
||
| Number of responders | 122 | 129 |
| Patients with DOR ≥ 12 months
Based on observed rates , %
|
66 | 59 |
| Patients with DOR ≥ 18 months , % | 35 | 23 |
4 Contraindications
None.
5.4 Ocular Toxicity
LAZCLUZE, in combination with amivantamab, can cause ocular toxicity, including keratitis.
In MARIPOSA [see Adverse Reactions (6.1)] , ocular toxicity occurred in 16% of patients treated with LAZCLUZE in combination with amivantamab, including Grade 3 or 4 ocular toxicity in 0.7% of patients. Promptly refer patients presenting with new or worsening eye symptoms to an ophthalmologist. Withhold, reduce the dose or permanently discontinue amivantamab and continue LAZCLUZE based on severity [see Dosage and Administration (2.4)] .
6 Adverse Reactions
The following adverse reactions are discussed elsewhere in the labeling:
- Venous Thromboembolic Events [see Warnings and Precautions (5.1)]
- Interstitial Lung Disease/Pneumonitis [see Warnings and Precautions (5.2)]
- Dermatologic Adverse Reactions [see Warnings and Precautions (5.3)]
- Ocular Toxicity [see Warnings and Precautions (5.4)]
7 Drug Interactions
Strong and moderate CYP3A4 inducers:Avoid concomitant use. ( 7.1)
8.6 Renal Impairment
No dose adjustment is recommended in patients with mild or moderate renal impairment (eGFR 30 – 89 mL/min) [see Clinical Pharmacology (12.3)] .
LAZCLUZE has not been studied in patients with severe renal impairment or end-stage renal disease (eGFR < 30 mL/min).
12.2 Pharmacodynamics
The exposure-response relationship and time-course of pharmacodynamic response of lazertinib have not been fully characterized.
12.3 Pharmacokinetics
Lazertinib pharmacokinetics are presented as mean (CV%) for descriptive parameters unless otherwise specified.
Lazertinib maximum plasma concentration (C max) and area under plasma concentration time curve (AUC) increased dose proportionally from 20 mg to 320 mg (0.08 to 1.3 times the approved recommended dosage) following a single administration and once daily administration. Lazertinib steady state plasma exposure was achieved by day 15 with approximately 2-fold accumulation for AUC.
2.1 Patient Selection
Select patients for the first-line treatment of NSCLC with LAZCLUZE, in combination with amivantamab, based on the presence of EGFR exon 19 deletions or exon 21 L858R substitution mutations in tumor or plasma specimens [see Clinical Studies (14)] . If these mutations are not detected in a plasma specimen, test tumor tissue. Information on FDA-approved tests is available at: http://www.fda.gov/CompanionDiagnostics.
8.7 Hepatic Impairment
No dose adjustment is recommended in patients with mild (total bilirubin ≤ ULN and AST > ULN or total bilirubin ≤ 1.5×ULN and any AST) or moderate (total bilirubin ≤ 1.5 to 3×ULN and any AST) hepatic impairment [see Clinical Pharmacology (12.3)] .
LAZCLUZE has not been studied in patients with severe hepatic impairment (total bilirubin > 3×ULN and any AST).
1 Indications and Usage
LAZCLUZE, in combination with amivantamab, is indicated for the first-line treatment of adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations, as detected by an FDA-approved test [see Dosage and Administration (2.1)] .
12.1 Mechanism of Action
Lazertinib is a kinase inhibitor of epidermal growth factor receptor (EGFR) that inhibits EGFR exon 19 deletions and exon 21 L858R substitution mutations at lower concentrations than wild-type EGFR. In human NSCLC cells and mouse xenograft models of EGFR exon 19 deletions or EGFR L858R substitution mutations, lazertinib demonstrated anti-tumor activity. Treatment with lazertinib in combination with amivantamab increased in vivo anti-tumor activity compared to either agent alone in a mouse xenograft model of human NSCLC with an EGFR L858R mutation.
5.5 Embryo Fetal Toxicity
Based on findings from animal studies and its mechanism of action, LAZCLUZE can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, oral administration of lazertinib to pregnant animals during the period of organogenesis resulted in reduced embryo-fetal survival and fetal body weight in rats and malformations in rabbits at exposures approximately 4 and 0.5 times, respectively, the human exposure at the recommended dose of 240 mg/day based on AUC.
Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with LAZCLUZE and for 3 weeks after the last dose. Advise male patients with female partners of reproductive potential to use effective contraception during treatment with LAZCLUZE and for 3 weeks after the last dose [see Use in Specific Populations (8.1, 8.3)].
5 Warnings and Precautions
- Venous Thromboembolic Events (VTE):Prophylactic anticoagulation is recommended for the first four months of treatment. Monitor for signs and symptoms of VTE and treat as medically appropriate. Withhold LAZCLUZE and amivantamab based on severity. Once anticoagulant treatment has been initiated, resume LAZCLUZE and amivantamab at the same dose at the discretion of the healthcare provider. Permanently discontinue amivantamab and continue LAZCLUZE for recurrent VTE despite therapeutic anticoagulation. (2.3, 2.4, 5.1)
- Interstitial Lung Disease (ILD)/Pneumonitis: Monitor for new or worsening symptoms indicative of ILD/pneumonitis. Withhold LAZCLUZE and amivantamab in patients with suspected ILD/pneumonitis and permanently discontinue if ILD/pneumonitis is confirmed. ( 2.4, 5.2)
- Dermatologic Adverse Reactions: Can cause severe rash including acneiform dermatitis. At treatment initiation, prophylactic and concomitant medications are recommended. Withhold, reduce the dose or permanently discontinue LAZCLUZE and amivantamab based on severity. (2.3, 2.4, 5.3)
- Ocular Adverse Reactions: Promptly refer patients with new or worsening signs and symptoms of ocular adverse reactions, including keratitis, to an ophthalmologist for evaluation. Withhold, reduce the dose, or permanently discontinue amivantamab and continue LAZCLUZE based on severity. ( 5.4)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise patients of reproductive potential of the potential risk to a fetus and to use effective contraception. ( 5.5, 8.1, 8.3)
2 Dosage and Administration
- The recommended dosage of LAZCLUZE is 240 mg orally once daily with or without food, given in combination with amivantamab. (2.2)
- Continue treatment until disease progression or unacceptable toxicity. ( 2.2)
- Administer LAZCLUZE any time prior to amivantamab when given on the same day. (2.2)
- Refer to the amivantamab prescribing information for recommended amivantamab dosing information. ( 2.2)
- Administer prophylactic and concomitant medications to reduce the risk of dermatologic adverse reactions. (2.3)
- Administer anticoagulant prophylaxis to reduce the risk of venous thromboembolic events (VTE) for the first four months of treatment. ( 2.3)
3 Dosage Forms and Strengths
Tablets:80 mg and 240 mg. ( 3)
8 Use in Specific Populations
Lactation:Advise not to breastfeed. ( 8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in WARNINGS AND PRECAUTIONS and below reflect exposure to LAZCLUZE in combination with amivantamab in 421 previously untreated patients with locally advanced or metastatic NSCLC whose tumors have EGFR exon 19 deletions or exon 21 L858R substitution mutations in MARIPOSA [see Clinical Studies (14)] . Patients received LAZCLUZE 240 mg orally once daily in combination with amivantamab intravenously at 1,050 mg (for patients < 80 kg) or 1,400 mg (for patients ≥ 80 kg) once weekly for 4 weeks, then every 2 weeks thereafter starting at week 5. Among the 421 patients who received LAZCLUZE in combination with amivantamab, 84% were exposed to LAZCLUZE for ≥ 6 months and 73% were exposed to LAZCLUZE for > 1 year.
The median age of patients who received LAZCLUZE in combination with amivantamab was 64 years (25 to 88); 64% were female; 59% were Asian, 38% were White, 1.7% were American Indian or Alaska Native, 0.7% were Black or African American, 1% were of unknown or other races; 13% were Hispanic or Latino; 67% had Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 1, 33% had ECOG PS of 0; 60% had EGFR exon 19 deletions, and 40% had EGFR exon 21 L858R substitution mutations.
Serious adverse reactions occurred in 49% of patients who received LAZCLUZE in combination with amivantamab. Serious adverse reactions occurring in ≥ 2% of patients included VTE (11%), pneumonia (4%), rash and ILD/pneumonitis (2.9% each), COVID-19 (2.4%), and pleural effusion and infusion-related reaction (amivantamab) (2.1% each). Fatal adverse reactions occurred in 7% of patients who received LAZCLUZE in combination with amivantamab due to death not otherwise specified (1.2%); sepsis and respiratory failure (1% each); pneumonia, myocardial infarction, and sudden death (0.7% each); cerebral infarction, pulmonary embolism (PE), and COVID-19 infection (0.5% each); and ILD/pneumonitis, acute respiratory distress syndrome (ARDS), and cardiopulmonary arrest (0.2% each).
Permanent discontinuation of LAZCLUZE due to an adverse reaction occurred in 21% of patients. Adverse reactions which resulted in permanent discontinuation of LAZCLUZE in ≥ 1% of patients included ILD/pneumonitis, pneumonia, VTE, rash, respiratory failure, and sudden death.
Dosage interruption of LAZCLUZE due to an adverse reaction occurred in 72% of patients. Adverse reactions which required dosage interruption in ≥ 5% of patients were rash, nail toxicity, COVID-19, VTE, increased ALT, and increased AST.
Dose reductions of LAZCLUZE due to an adverse reaction occurred in 42% of patients. Adverse reactions requiring LAZCLUZE dose reductions in ≥ 5% of patients were rash and nail toxicity.
The most common adverse reactions (≥ 20%) were rash, nail toxicity, infusion-related reaction (amivantamab), musculoskeletal pain, edema, stomatitis, VTE, paresthesia, fatigue, diarrhea, constipation, COVID-19, hemorrhage, dry skin, decreased appetite, pruritus, and nausea. The most common Grade 3 or 4 laboratory abnormalities (≥ 2%) were decreased albumin, decreased sodium, increased ALT, decreased potassium, decreased hemoglobin, increased AST, increased GGT, and increased magnesium.
Table 3 summarizes the adverse reactions (≥ 10%) in MARIPOSA.
| Adverse Reaction | LAZCLUZE in combination with amivantamab
(N=421) |
Osimertinib
(N=428) |
||
|---|---|---|---|---|
| All Grades
(%) |
Grade 3 or 4
(%) |
All Grades
(%) |
Grade 3 or 4
(%) |
|
| Skin and subcutaneous tissue disorders | ||||
| Rash
Grouped terms
|
86 | 26 | 48 | 1.2 |
| Nail toxicity | 71 | 11 | 34 | 0.7 |
| Dry skin | 25 | 1 | 18 | 0.2 |
| Pruritus | 24 | 0.5 | 17 | 0.2 |
| Injury, poisoning and procedural complications | ||||
| Infusion-related reaction
Applicable only to amivantamab
|
63 | 6 | 0 | 0 |
| Musculoskeletal and connective tissue disorders | ||||
| Musculoskeletal pain | 47 | 2.1 | 39 | 1.9 |
| Gastrointestinal disorders | ||||
| Stomatitis | 43 | 2.4 | 27 | 0.5 |
| Diarrhea | 31 | 2.6 | 45 | 0.9 |
| Constipation | 29 | 0 | 13 | 0 |
| Nausea | 21 | 1.2 | 14 | 0.2 |
| Vomiting | 12 | 0.5 | 5 | 0 |
| Abdominal pain | 11 | 0 | 10 | 0 |
| Hemorrhoids | 10 | 0.2 | 2.1 | 0.2 |
| General disorders and administration site conditions | ||||
| Edema | 43 | 2.6 | 8 | 0 |
| Fatigue | 32 | 3.8 | 20 | 1.9 |
| Pyrexia | 12 | 0 | 9 | 0 |
| Vascular disorders | ||||
| Venous thromboembolism | 36 | 11 | 8 | 2.8 |
| Hemorrhage | 25 | 1 | 13 | 1.2 |
| Nervous system disorders | ||||
| Paresthesia | 35 | 1.7 | 10 | 0.2 |
| Dizziness | 14 | 0 | 10 | 0 |
| Headache | 13 | 0.2 | 13 | 0 |
| Infections and infestations | ||||
| COVID-19 | 26 | 1.7 | 24 | 1.4 |
| Conjunctivitis | 11 | 0.2 | 1.6 | 0 |
| Metabolism and nutrition disorders | ||||
| Decreased appetite | 24 | 1 | 18 | 1.4 |
| Respiratory, thoracic and mediastinal disorders | ||||
| Cough | 19 | 0 | 23 | 0 |
| Dyspnea | 14 | 1.7 | 17 | 3.5 |
| Eye disorders | ||||
| Ocular toxicity | 16 | 0.7 | 7 | 0 |
| Psychiatric disorders | ||||
| Insomnia | 10 | 0 | 11 | 0 |
Clinically relevant adverse reactions occurring in < 10% of patients who received LAZCLUZE in combination with amivantamab included skin ulcer (applicable to amivantamab) and ILD/pneumonitis.
Table 4 summarizes the laboratory abnormalities in MARIPOSA.
| Laboratory Abnormality | LAZCLUZE in combination with amivantamab
(N=421) |
Osimertinib
(N=428) |
||
|---|---|---|---|---|
| All Grades
(%) |
Grade 3 or 4
(%) |
All Grades
(%) |
Grade 3 or 4
(%) |
|
| Chemistry | ||||
| Decreased albumin | 89 | 8 | 22 | 0.2 |
| Increased ALT | 65 | 7 | 29 | 2.6 |
| Increased AST | 52 | 3.8 | 36 | 1.9 |
| Increased alkaline phosphatase | 45 | 0.5 | 15 | 0.5 |
| Decreased calcium (corrected) | 41 | 1.4 | 27 | 0.7 |
| Increased GGT | 39 | 2.6 | 24 | 1.9 |
| Decreased sodium | 38 | 7 | 35 | 5 |
| Decreased potassium | 30 | 5 | 15 | 1.2 |
| Increased creatinine | 26 | 0.7 | 35 | 0.7 |
| Decreased magnesium | 25 | 0.7 | 10 | 0.2 |
| Increased magnesium | 12 | 2.6 | 20 | 4.8 |
| Hematology | ||||
| Decreased platelet count | 52 | 0.7 | 57 | 1.4 |
| Decreased hemoglobin | 47 | 3.8 | 56 | 1.9 |
| Decreased white blood cell | 38 | 1.0 | 66 | 0.7 |
| Decreased neutrophils | 15 | 1.4 | 33 | 1.4 |
5.1 Venous Thromboembolic Events
LAZCLUZE in combination with amivantamab can cause serious and fatal venous thromboembolic events (VTE), including deep venous thrombosis (DVT) and pulmonary embolism (PE). The majority of these events occurred during the first four months of therapy [see Adverse Reactions (6.1)] .
In MARIPOSA [see Adverse Reactions (6.1)] , VTE occurred in 36% of patients receiving LAZCLUZE in combination with amivantamab, including Grade 3 in 10% and Grade 4 in 0.5% of patients. On-study VTEs occurred in 1.2% of patients (n=5) while receiving anticoagulation therapy. There were two fatal cases of VTE (0.5%), 7% of patients had VTE leading to dose interruptions of LAZCLUZE, 0.5% of patients had VTE leading to dose reductions of LAZCLUZE, and 1.9% of patients permanently discontinued LAZCLUZE due to VTE. The median time to onset of VTEs was 84 days (range: 6 to 777).
Administer prophylactic anticoagulation for the first four months of treatment [see Dosage and Administration (2.3)] . The use of Vitamin K antagonists is not recommended. Monitor for signs and symptoms of VTE and treat as medically appropriate.
Withhold LAZCLUZE and amivantamab based on severity [see Dosage and Administration (2.4)]. Once anticoagulant treatment has been initiated, resume LAZCLUZE and amivantamab at the same dose level at the discretion of the healthcare provider. In the event of VTE recurrence despite therapeutic anticoagulation, permanently discontinue amivantamab. Continue treatment with LAZCLUZE at the same dose level at the discretion of the healthcare provider [see Dosage and Administration (2.4)] . Refer to the amivantamab prescribing information for recommended amivantamab dosage modification.
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
5.3 Dermatologic Adverse Reactions
LAZCLUZE in combination with amivantamab can cause severe rash including dermatitis acneiform, pruritus and dry skin.
In MARIPOSA [see Adverse Reactions (6.1)] , rash occurred in 86% of patients treated with LAZCLUZE in combination with amivantamab, including Grade 3 in 26% of patients. The median time to onset of rash was 14 days (range: 1 to 556 days). Rash leading to dose reduction of LAZCLUZE occurred in 19% of patients, rash leading to dose interruption of LAZCLUZE occurred in 30% of patients, and LAZCLUZE was permanently discontinued due to rash in 1.7% of patients [see Adverse Reactions (6.1)].
When initiating treatment with LAZCLUZE in combination with amivantamab, prophylactic and concomitant medications are recommended to reduce the risk and severity of dermatologic adverse reactions [see Dosage and Administration (2.3)]. Instruct patients to limit sun exposure during and for 2 months after treatment with LAZCLUZE in combination with amivantamab. Advise patients to wear protective clothing and use broad-spectrum UVA/UVB sunscreen.
If skin reactions develop, administer supportive care including topical corticosteroids and topical and/or oral antibiotics. For Grade 3 reactions, administer oral steroids and consider dermatologic consultation. Promptly refer patients presenting with severe rash, atypical appearance or distribution, or lack of improvement within 2 weeks to a dermatologist. Withhold, reduce the dose or permanently discontinue LAZCLUZE and amivantamab based on severity [see Dosage and Administration (2.4)] .
16 How Supplied/storage and Handling
LAZCLUZE ®(lazertinib) tablets are available in the strengths and packages listed below:
| Tablet Strength | Description | Package Configuration | NDC Number |
|---|---|---|---|
| 80 mg | Yellow, oval, film-coated, debossed with "LZ" on one side and "80" on the other side | 60-count bottle | NDC 57894-080-60 |
| 240 mg | Reddish purple, oval, film-coated, debossed with "LZ" on one side and "240" on the other side | 30-count bottle | NDC 57894-240-30 |
13.2 Animal Toxicology And/or Pharmacology
In repeat-dose oral general toxicology studies up to 13-weeks duration in rats and dogs, lazertinib induced multi-organ histologic hyperplasia at exposures approximately equivalent or greater to the human exposure at the recommended dose of 240 mg. Hyperplasia was not reversible in the mandibular lymph node in the 4-week rat study. In rats, lazertinib induced renal toxicity characterized by histologic hyperplasia and inflammation in the kidney at doses ≥ 25 mg/kg (approximately 0.9 times the human exposure at the recommended dose of 240 mg/day based on AUC), along with increased urea nitrogen and histologic papillary necrosis, tubule degeneration/regeneration, and tubule dilatation at exposures approximately 4.4 times the human exposure at the recommended dose of 240 mg/day based on AUC. Increased urea nitrogen, papillary necrosis, and tubule dilatation showed evidence of recovery. In the 13-week toxicology study in dogs, one high dose animal exhibited unilateral tubule cell renal carcinoma at 8 mg/kg/day (approximately 2 times the human exposure at the recommended dose of 240 mg/day based on AUC). Other renal findings in high dose dogs included tubule degeneration/regeneration and infarct, which showed evidence of recovery. In the 4-week toxicology study, lazertinib induced cardiac toxicity in two dogs characterized by histologic findings in the heart (degeneration/necrosis of the myocardium and vessels, fibrosis, hemorrhage, thrombus, mixed cell/vessel inflammation) at 20 mg/kg (approximately 4.8 times the clinical AUC at the 240 mg human dose). One of these dogs also exhibited increased cardiac troponin I and premature ventricular complexes. These cardiac findings were not seen after a 2-week recovery period.
2.4 Dosage Modifications for Adverse Reactions
The recommended LAZCLUZE dose reductions for adverse reactions are presented in Table 1.
| Dose at which the adverse reaction occurred | 1 st Dose Reduction | 2 nd Dose Reduction | 3 rd Dose Reduction |
|---|---|---|---|
| 240 mg once daily
(one 240 mg tablet) |
160 mg once daily
(two 80 mg tablets) |
80 mg once daily
(one 80 mg tablet) |
Discontinue LAZCLUZE |
The recommended management and dosage modifications of LAZCLUZE for specific adverse reactions are presented in Table 2. Refer to the amivantamab prescribing information for information about dosage modifications for amivantamab.
| Adverse Reaction | Severity | Dosage Modification |
|---|---|---|
| Venous Thromboembolic Events (VTE)
[see Warnings and Precautions (5.1)] |
Grade 2 or 3 |
|
| Grade 4 or recurrent Grade 2 or 3 despite therapeutic level anticoagulation |
|
|
| Interstitial Lung Disease (ILD)/Pneumonitis
[see Warnings and Precautions (5.2)] |
Any Grade |
|
| Dermatologic Adverse Reactions (including dermatitis acneiform, pruritus, dry skin) [see Warnings and Precautions (5.3)] | Grade 1 |
|
| Grade 2 |
|
|
| Grade 3 |
|
|
| Grade 4
(including severe bullous, blistering or exfoliating skin conditions) |
|
|
| Other Adverse Reactions [see Adverse Reactions (6.1)] | Grade 3–4 |
|
5.2 Interstitial Lung Disease (ild)/pneumonitis
LAZCLUZE in combination with amivantamab can cause interstitial lung disease (ILD)/pneumonitis.
In MARIPOSA [see Adverse Reactions (6.1)], ILD/pneumonitis occurred in 3.1% of patients treated with LAZCLUZE in combination with amivantamab, including Grade 3 in 1.0% and Grade 4 in 0.2% of patients. There was one fatal case (0.2%) of ILD/pneumonitis and 2.9% of patients permanently discontinued LAZCLUZE and amivantamab due to ILD/pneumonitis [see Adverse Reactions (6.1)].
Monitor patients for new or worsening symptoms indicative of ILD/pneumonitis (e.g., dyspnea, cough, fever). Immediately withhold LAZCLUZE and amivantamab in patients with suspected ILD/pneumonitis and permanently discontinue if ILD/pneumonitis is confirmed [see Dosage and Administration (2.4)].
8.3 Females and Males of Reproductive Potential
Based on animal data and its mechanism of action, LAZCLUZE can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)] .
Principal Display Panel 80 Mg Tablet Bottle Carton
NDC 57894-080-60
Lazcluze™
(lazertinib)
tablets
80 mg
Each film-coated tablet contains
80 mg of lazertinib equivalent to
93.86 mg lazertinib mesylate
(on anhydrous basis).
Rx only
60 film-coated tablets
janssen
Principal Display Panel 240 Mg Tablet Bottle Carton
NDC 57894-240-30
Lazcluze™
(lazertinib)
tablets
240 mg
Each film-coated tablet contains
240 mg of lazertinib equivalent
to 281.58 mg lazertinib mesylate
(on anhydrous basis).
Rx only
30 film-coated tablets
janssen
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with lazertinib.
Lazertinib was not genotoxic in an in vitro bacterial reverse mutation (Ames) assay, an in vitro chromosomal aberration assay, or an in vivo micronucleus assay in rats.
In a dedicated fertility and early embryonic development study, male and female rats received oral doses of 7.5, 15, or 30 mg/kg/day of lazertinib. Males were dosed for 10 weeks (29 days prior to pairing, during mating period and continuing post-pairing). Females were dosed for 15 days prior to pairing, during mating period and up to Gestation Day 7. Lazertinib did not have clear effects on estrous cyclicity, mating, fertility, or sperm parameters, but induced an increase in post-implantation loss and decreased number of live fetuses at 30 mg/kg/day (approximately 1.2 times the recommended human dose of 240 mg based on body surface area). In repeat-dose oral general toxicology studies up to 13-weeks duration, lazertinib induced histologic tubular degeneration in the testis; cellular lumen debris, degeneration/necrosis, and reduced sperm in the epididymis; decreased corpora lutea in the ovary; and atrophy in the uterus and vagina. These effects were observed at exposures approximately equivalent to the human exposure at the recommended dose of 240 mg in males, and at exposures approximately 2 times the human exposure at the recommended dose of 240 mg dose in females. Findings in female reproductive organs were reversible. The tubular degeneration in the testis observed in rats at exposures approximately 4 times the human exposure at the recommended dose was not reversible within a 2-week recovery period.
Structured Label Content
Section 42229-5 (42229-5)
Recommended Dosage and Administration
The recommended dosage of LAZCLUZE is 240 mg orally once daily administered in combination with amivantamab, with or without food. Swallow LAZCLUZE tablets whole. Do not crush, split, or chew. Continue treatment until disease progression or unacceptable toxicity.
Administer LAZCLUZE any time prior to amivantamab when given on the same day. Refer to the amivantamab prescribing information for recommended amivantamab dosing information.
Section 42230-3 (42230-3)
| This Patient Information has been approved by the U.S. Food and Drug Administration. | Revised: 11/2025 |
|
PATIENT INFORMATION
LAZCLUZE ® (laz-kluez) (lazertinib) tablets, for oral use |
|
|
What is LAZCLUZE?
LAZCLUZE in combination with amivantamab is a prescription medicine for the first-line treatment of adults with non-small cell lung cancer (NSCLC) that:
It is not known if LAZCLUZE is safe and effective in children. |
|
Before taking LAZCLUZE, tell your healthcare provider about all of your medical conditions, including if you:
LAZCLUZE may affect the way other medicines work, and other medicines may affect how LAZCLUZE works. You should not start or stop any medicine before you talk with your healthcare provider that prescribed LAZCLUZE. |
|
How should I take LAZCLUZE?
|
|
|
What should I avoid while taking LAZCLUZE?
|
|
|
What are the possible side effects of LAZCLUZE?
LAZCLUZE may cause serious side effects, including:
The most common side effects of LAZCLUZE in combination with amivantamab include: |
|
|
|
| LAZCLUZE may cause fertility problems in males and females, which may affect your ability to have children. Talk to your healthcare provider if this is a concern for you.
Your healthcare provider may temporarily stop, decrease your dose or completely stop your treatment with LAZCLUZE if you have serious side effects. These are not all of the possible side effects of LAZCLUZE. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
How should I store LAZCLUZE?
|
|
|
General information about the safe and effective use of LAZCLUZE.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use LAZCLUZE for a condition for which it was not prescribed. Do not give LAZCLUZE to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about LAZCLUZE that is written for health professionals. |
|
|
What are the ingredients in LAZCLUZE?
Active ingredient : lazertinib mesylate Inactive ingredients: croscarmellose sodium, magnesium stearate, mannitol, microcrystalline cellulose, and silica hydrophobic colloidal. The tablet coating consists of glycerol monocaprylocaprate type I, iron oxide black (in 240 mg strength tablets), iron oxide red (in 240 mg strength tablets), iron oxide yellow (in 80 mg strength tablets), macrogol (PEG) polyvinyl alcohol graft copolymer, polyvinyl alcohol-partially hydrolyzed, talc, and titanium dioxide. Product of Belgium Manufactured for: Janssen Biotech, Inc., Horsham, PA 19044, USA For patent information: www.janssenpatents.com © Johnson & Johnson and its affiliates 2024–2025 For more information, call 1-800-526-7736 or go to www.lazcluze.com |
Section 43683-2 (43683-2)
Section 44425-7 (44425-7)
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
11 Description (11 DESCRIPTION)
LAZCLUZE ®tablets contain lazertinib, a kinase inhibitor for oral use. Lazertinib is present as lazertinib mesylate hydrate with a molecular weight of 668.77 and molecular formula of C 30H 34N 8O 3∙CH 4O 3S∙H 2O. The chemical name is N-[5-[[4-[4-[(Dimethylamino)methyl]-3-phenyl-1 H-pyrazol-1-yl]pyrimidin-2-yl]amino]-4-methoxy-2-(morpholin-4-yl)phenyl]acrylamide methanesulfonate hydrate (1:1:1). Lazertinib mesylate hydrate is soluble or practically insoluble in aqueous media, and slightly soluble to freely soluble in organic solvents over a wide range of pH values. The structural formula is:
LAZCLUZE (lazertinib) film-coated tablets contain 80 mg or 240 mg of lazertinib, equivalent to 93.86 and 281.58 mg lazertinib mesylate (calculated on anhydrous basis), respectively. The inactive ingredients are croscarmellose sodium, magnesium stearate, mannitol, microcrystalline cellulose, and silica hydrophobic colloidal. The tablet coating consists of glycerol monocaprylocaprate type I, iron oxide black (in 240 mg strength tablets), iron oxide red (in 240 mg strength tablets), iron oxide yellow (in 80 mg strength tablets), macrogol (PEG) polyvinyl alcohol graft copolymer, polyvinyl alcohol-partially hydrolyzed, talc, and titanium dioxide.
8.4 Pediatric Use
The safety and effectiveness of LAZCLUZE in pediatric patients have not been established.
8.5 Geriatric Use
Of the 421 patients with locally advanced or metastatic NSCLC treated with LAZCLUZE in combination with amivantamab in MARIPOSA, 45% were 65 years and older and 12% were 75 years and older. No overall differences in safety or effectiveness were observed between patients aged 65 and older and younger patients.
14 Clinical Studies (14 CLINICAL STUDIES)
The efficacy of LAZCLUZE, in combination with amivantamab, was evaluated in MARIPOSA [NCT04487080], a randomized, active-controlled, multicenter trial. Eligible patients were required to have untreated locally advanced or metastatic NSCLC with either exon 19 deletions or exon 21 L858R substitution EGFR mutations identified by local testing, not amenable to curative therapy. Patients with asymptomatic or previously treated and stable intracranial metastases were eligible to enroll.
Patients were randomized (2:2:1) to receive LAZCLUZE in combination with amivantamab (N=429), osimertinib monotherapy (N=429), or LAZCLUZE monotherapy (an unapproved regimen for NSCLC) until disease progression or unacceptable toxicity. The evaluation of efficacy for the treatment of untreated metastatic NSCLC relied upon comparison between:
- LAZCLUZE administered at 240 mg orally once daily in combination with amivantamab administered intravenously at 1050 mg (for patients < 80 kg) or 1400 mg (for patients ≥ 80 kg) once weekly for 4 weeks, then every 2 weeks thereafter starting at week 5.
- Osimertinib administered at a dose of 80 mg orally once daily.
Randomization was stratified by EGFR mutation type (exon 19 deletion or exon 21 L858R substitution mutation), Asian race (yes or no), and history of brain metastasis (yes or no). Tumor assessments were performed every 8 weeks for 30 months, and then every 12 weeks until disease progression.
The major efficacy outcome measure was progression-free survival (PFS) as assessed by blinded independent central review (BICR). Additional efficacy outcome measures included overall survival (OS), overall response rate (ORR) and duration of response (DOR).
A total of 858 patients were randomized between the two study arms, 429 to the LAZCLUZE in combination with amivantamab arm and 429 to the osimertinib arm. The median age was 63 (range: 25–88) years; 61% were female; 58% were Asian, and 38% were White, 1.6% were American Indian or Alaska Native, 0.8% were Black or African American, 0.2% were Native Hawaiian or other Pacific Islander, 0.6% were unknown race or multiple races; and 12% were Hispanic or Latino. Eastern Cooperative Oncology Group (ECOG) performance status was 0 (34%) or 1 (66%); 69% never smoked; 41% had prior brain metastases; and 89% had Stage IV cancer at initial diagnosis. Sixty percent of patients had tumors harboring exon 19 deletions and the remaining 40% had exon 21 L858R substitution mutations.
Among the 858 patients with EGFR exon 19 deletion or L858R substitution mutations that were randomized between the amivantamab plus LAZCLUZE arm versus the osimertinib arm, available tissue samples from 544 (63%) patients had evaluable results when tested retrospectively using the cobas EGFR Mutation Test v2. Of the 544 patients with evaluable results, 527 (97%) patients were positive for EGFR exon 19 deletion or L858R substitution mutations, while 17 (3%) patients were negative. Available plasma samples from patients were retrospectively tested using an FDA-approved test to confirm the biomarker status.
The trial demonstrated a statistically significant improvement in PFS by BICR assessment and OS for LAZCLUZE in combination with amivantamab compared to osimertinib (see Table 5and Figures 1and 2).
Efficacy results are provided in Table 5.
| LAZCLUZE in combination with amivantamab
(N=429) |
Osimertinib
(N=429) |
|
|---|---|---|
| CI = confidence interval; NR = not reached; NE = not estimable | ||
| Progression-free survival (PFS) | ||
| Number of events (%) | 192 (45) | 252 (59) |
| Median, months (95% CI) | 23.7 (19.1, 27.7) | 16.6 (14.8, 18.5) |
| HR
Stratified by mutation type (Exon 19del or Exon 21 L858R), prior brain metastases (yes or no), and Asian race (yes or no).
,
Stratified Cox proportional hazards regression. (95% CI); p-value
,
Stratified log-rank test.
|
0.70 (0.58, 0.85); p=0.0002 | |
| Overall survival (OS) | ||
| Number of events (%) | 173 (40) | 217 (51) |
| Median, months (95% CI) | NR (42.9, NE) | 36.7 (33.4, 41.0) |
| HR , (95% CI); p-value , | 0.75 (0.61, 0.92); p=0.0048 | |
| Overall response rate (ORR)
Confirmed responses based on the ITT population.
|
||
| ORR, % (95% CI) | 78 (74, 82) | 73 (69, 78) |
| Complete response, % | 5 | 3.5 |
| Partial response, % | 73 | 70 |
| Duration of response (DOR)
In confirmed responders.
|
||
| Median (95% CI), months | 25.8 (20.1, NE) | 16.7 (14.8, 18.5) |
| Patients with DOR ≥ 6 months
Based on observed rates. , %
|
86 | 85 |
| Patients with DOR ≥ 12 months , % | 68 | 57 |
Figure 1: Kaplan-Meier Curves of PFS by BICR Assessment in Patients with Previously Untreated NSCLC
Figure 2: Kaplan-Meier Curves of OS in Patients with Previously Untreated NSCLC
Out of all randomized patients (n=858), 367 (43%) had baseline intracranial lesions assessed by BICR using modified RECIST. Results of pre-specified analyses of intracranial ORR and DOR by BICR in the subset of patients with intracranial lesions at baseline for the LAZCLUZE in combination with amivantamab arm and the osimertinib arm are summarized in Table 6.
| LAZCLUZE in combination with amivantamab
(N=180) |
Osimertinib
(N=187) |
|
|---|---|---|
| CI = confidence interval | ||
| Intracranial Tumor Response Assessment | ||
| Intracranial ORR
Confirmed responses , % (95% CI)
|
68 (60, 75) | 69 (62, 76) |
| Complete response, % | 55 | 52 |
| Intracranial DOR
In confirmed responders
|
||
| Number of responders | 122 | 129 |
| Patients with DOR ≥ 12 months
Based on observed rates , %
|
66 | 59 |
| Patients with DOR ≥ 18 months , % | 35 | 23 |
4 Contraindications (4 CONTRAINDICATIONS)
None.
5.4 Ocular Toxicity
LAZCLUZE, in combination with amivantamab, can cause ocular toxicity, including keratitis.
In MARIPOSA [see Adverse Reactions (6.1)] , ocular toxicity occurred in 16% of patients treated with LAZCLUZE in combination with amivantamab, including Grade 3 or 4 ocular toxicity in 0.7% of patients. Promptly refer patients presenting with new or worsening eye symptoms to an ophthalmologist. Withhold, reduce the dose or permanently discontinue amivantamab and continue LAZCLUZE based on severity [see Dosage and Administration (2.4)] .
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following adverse reactions are discussed elsewhere in the labeling:
- Venous Thromboembolic Events [see Warnings and Precautions (5.1)]
- Interstitial Lung Disease/Pneumonitis [see Warnings and Precautions (5.2)]
- Dermatologic Adverse Reactions [see Warnings and Precautions (5.3)]
- Ocular Toxicity [see Warnings and Precautions (5.4)]
7 Drug Interactions (7 DRUG INTERACTIONS)
Strong and moderate CYP3A4 inducers:Avoid concomitant use. ( 7.1)
8.6 Renal Impairment
No dose adjustment is recommended in patients with mild or moderate renal impairment (eGFR 30 – 89 mL/min) [see Clinical Pharmacology (12.3)] .
LAZCLUZE has not been studied in patients with severe renal impairment or end-stage renal disease (eGFR < 30 mL/min).
12.2 Pharmacodynamics
The exposure-response relationship and time-course of pharmacodynamic response of lazertinib have not been fully characterized.
12.3 Pharmacokinetics
Lazertinib pharmacokinetics are presented as mean (CV%) for descriptive parameters unless otherwise specified.
Lazertinib maximum plasma concentration (C max) and area under plasma concentration time curve (AUC) increased dose proportionally from 20 mg to 320 mg (0.08 to 1.3 times the approved recommended dosage) following a single administration and once daily administration. Lazertinib steady state plasma exposure was achieved by day 15 with approximately 2-fold accumulation for AUC.
2.1 Patient Selection
Select patients for the first-line treatment of NSCLC with LAZCLUZE, in combination with amivantamab, based on the presence of EGFR exon 19 deletions or exon 21 L858R substitution mutations in tumor or plasma specimens [see Clinical Studies (14)] . If these mutations are not detected in a plasma specimen, test tumor tissue. Information on FDA-approved tests is available at: http://www.fda.gov/CompanionDiagnostics.
8.7 Hepatic Impairment
No dose adjustment is recommended in patients with mild (total bilirubin ≤ ULN and AST > ULN or total bilirubin ≤ 1.5×ULN and any AST) or moderate (total bilirubin ≤ 1.5 to 3×ULN and any AST) hepatic impairment [see Clinical Pharmacology (12.3)] .
LAZCLUZE has not been studied in patients with severe hepatic impairment (total bilirubin > 3×ULN and any AST).
1 Indications and Usage (1 INDICATIONS AND USAGE)
LAZCLUZE, in combination with amivantamab, is indicated for the first-line treatment of adult patients with locally advanced or metastatic non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletions or exon 21 L858R substitution mutations, as detected by an FDA-approved test [see Dosage and Administration (2.1)] .
12.1 Mechanism of Action
Lazertinib is a kinase inhibitor of epidermal growth factor receptor (EGFR) that inhibits EGFR exon 19 deletions and exon 21 L858R substitution mutations at lower concentrations than wild-type EGFR. In human NSCLC cells and mouse xenograft models of EGFR exon 19 deletions or EGFR L858R substitution mutations, lazertinib demonstrated anti-tumor activity. Treatment with lazertinib in combination with amivantamab increased in vivo anti-tumor activity compared to either agent alone in a mouse xenograft model of human NSCLC with an EGFR L858R mutation.
5.5 Embryo Fetal Toxicity (5.5 Embryo-Fetal Toxicity)
Based on findings from animal studies and its mechanism of action, LAZCLUZE can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, oral administration of lazertinib to pregnant animals during the period of organogenesis resulted in reduced embryo-fetal survival and fetal body weight in rats and malformations in rabbits at exposures approximately 4 and 0.5 times, respectively, the human exposure at the recommended dose of 240 mg/day based on AUC.
Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with LAZCLUZE and for 3 weeks after the last dose. Advise male patients with female partners of reproductive potential to use effective contraception during treatment with LAZCLUZE and for 3 weeks after the last dose [see Use in Specific Populations (8.1, 8.3)].
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Venous Thromboembolic Events (VTE):Prophylactic anticoagulation is recommended for the first four months of treatment. Monitor for signs and symptoms of VTE and treat as medically appropriate. Withhold LAZCLUZE and amivantamab based on severity. Once anticoagulant treatment has been initiated, resume LAZCLUZE and amivantamab at the same dose at the discretion of the healthcare provider. Permanently discontinue amivantamab and continue LAZCLUZE for recurrent VTE despite therapeutic anticoagulation. (2.3, 2.4, 5.1)
- Interstitial Lung Disease (ILD)/Pneumonitis: Monitor for new or worsening symptoms indicative of ILD/pneumonitis. Withhold LAZCLUZE and amivantamab in patients with suspected ILD/pneumonitis and permanently discontinue if ILD/pneumonitis is confirmed. ( 2.4, 5.2)
- Dermatologic Adverse Reactions: Can cause severe rash including acneiform dermatitis. At treatment initiation, prophylactic and concomitant medications are recommended. Withhold, reduce the dose or permanently discontinue LAZCLUZE and amivantamab based on severity. (2.3, 2.4, 5.3)
- Ocular Adverse Reactions: Promptly refer patients with new or worsening signs and symptoms of ocular adverse reactions, including keratitis, to an ophthalmologist for evaluation. Withhold, reduce the dose, or permanently discontinue amivantamab and continue LAZCLUZE based on severity. ( 5.4)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise patients of reproductive potential of the potential risk to a fetus and to use effective contraception. ( 5.5, 8.1, 8.3)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
- The recommended dosage of LAZCLUZE is 240 mg orally once daily with or without food, given in combination with amivantamab. (2.2)
- Continue treatment until disease progression or unacceptable toxicity. ( 2.2)
- Administer LAZCLUZE any time prior to amivantamab when given on the same day. (2.2)
- Refer to the amivantamab prescribing information for recommended amivantamab dosing information. ( 2.2)
- Administer prophylactic and concomitant medications to reduce the risk of dermatologic adverse reactions. (2.3)
- Administer anticoagulant prophylaxis to reduce the risk of venous thromboembolic events (VTE) for the first four months of treatment. ( 2.3)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Tablets:80 mg and 240 mg. ( 3)
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
Lactation:Advise not to breastfeed. ( 8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in WARNINGS AND PRECAUTIONS and below reflect exposure to LAZCLUZE in combination with amivantamab in 421 previously untreated patients with locally advanced or metastatic NSCLC whose tumors have EGFR exon 19 deletions or exon 21 L858R substitution mutations in MARIPOSA [see Clinical Studies (14)] . Patients received LAZCLUZE 240 mg orally once daily in combination with amivantamab intravenously at 1,050 mg (for patients < 80 kg) or 1,400 mg (for patients ≥ 80 kg) once weekly for 4 weeks, then every 2 weeks thereafter starting at week 5. Among the 421 patients who received LAZCLUZE in combination with amivantamab, 84% were exposed to LAZCLUZE for ≥ 6 months and 73% were exposed to LAZCLUZE for > 1 year.
The median age of patients who received LAZCLUZE in combination with amivantamab was 64 years (25 to 88); 64% were female; 59% were Asian, 38% were White, 1.7% were American Indian or Alaska Native, 0.7% were Black or African American, 1% were of unknown or other races; 13% were Hispanic or Latino; 67% had Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 1, 33% had ECOG PS of 0; 60% had EGFR exon 19 deletions, and 40% had EGFR exon 21 L858R substitution mutations.
Serious adverse reactions occurred in 49% of patients who received LAZCLUZE in combination with amivantamab. Serious adverse reactions occurring in ≥ 2% of patients included VTE (11%), pneumonia (4%), rash and ILD/pneumonitis (2.9% each), COVID-19 (2.4%), and pleural effusion and infusion-related reaction (amivantamab) (2.1% each). Fatal adverse reactions occurred in 7% of patients who received LAZCLUZE in combination with amivantamab due to death not otherwise specified (1.2%); sepsis and respiratory failure (1% each); pneumonia, myocardial infarction, and sudden death (0.7% each); cerebral infarction, pulmonary embolism (PE), and COVID-19 infection (0.5% each); and ILD/pneumonitis, acute respiratory distress syndrome (ARDS), and cardiopulmonary arrest (0.2% each).
Permanent discontinuation of LAZCLUZE due to an adverse reaction occurred in 21% of patients. Adverse reactions which resulted in permanent discontinuation of LAZCLUZE in ≥ 1% of patients included ILD/pneumonitis, pneumonia, VTE, rash, respiratory failure, and sudden death.
Dosage interruption of LAZCLUZE due to an adverse reaction occurred in 72% of patients. Adverse reactions which required dosage interruption in ≥ 5% of patients were rash, nail toxicity, COVID-19, VTE, increased ALT, and increased AST.
Dose reductions of LAZCLUZE due to an adverse reaction occurred in 42% of patients. Adverse reactions requiring LAZCLUZE dose reductions in ≥ 5% of patients were rash and nail toxicity.
The most common adverse reactions (≥ 20%) were rash, nail toxicity, infusion-related reaction (amivantamab), musculoskeletal pain, edema, stomatitis, VTE, paresthesia, fatigue, diarrhea, constipation, COVID-19, hemorrhage, dry skin, decreased appetite, pruritus, and nausea. The most common Grade 3 or 4 laboratory abnormalities (≥ 2%) were decreased albumin, decreased sodium, increased ALT, decreased potassium, decreased hemoglobin, increased AST, increased GGT, and increased magnesium.
Table 3 summarizes the adverse reactions (≥ 10%) in MARIPOSA.
| Adverse Reaction | LAZCLUZE in combination with amivantamab
(N=421) |
Osimertinib
(N=428) |
||
|---|---|---|---|---|
| All Grades
(%) |
Grade 3 or 4
(%) |
All Grades
(%) |
Grade 3 or 4
(%) |
|
| Skin and subcutaneous tissue disorders | ||||
| Rash
Grouped terms
|
86 | 26 | 48 | 1.2 |
| Nail toxicity | 71 | 11 | 34 | 0.7 |
| Dry skin | 25 | 1 | 18 | 0.2 |
| Pruritus | 24 | 0.5 | 17 | 0.2 |
| Injury, poisoning and procedural complications | ||||
| Infusion-related reaction
Applicable only to amivantamab
|
63 | 6 | 0 | 0 |
| Musculoskeletal and connective tissue disorders | ||||
| Musculoskeletal pain | 47 | 2.1 | 39 | 1.9 |
| Gastrointestinal disorders | ||||
| Stomatitis | 43 | 2.4 | 27 | 0.5 |
| Diarrhea | 31 | 2.6 | 45 | 0.9 |
| Constipation | 29 | 0 | 13 | 0 |
| Nausea | 21 | 1.2 | 14 | 0.2 |
| Vomiting | 12 | 0.5 | 5 | 0 |
| Abdominal pain | 11 | 0 | 10 | 0 |
| Hemorrhoids | 10 | 0.2 | 2.1 | 0.2 |
| General disorders and administration site conditions | ||||
| Edema | 43 | 2.6 | 8 | 0 |
| Fatigue | 32 | 3.8 | 20 | 1.9 |
| Pyrexia | 12 | 0 | 9 | 0 |
| Vascular disorders | ||||
| Venous thromboembolism | 36 | 11 | 8 | 2.8 |
| Hemorrhage | 25 | 1 | 13 | 1.2 |
| Nervous system disorders | ||||
| Paresthesia | 35 | 1.7 | 10 | 0.2 |
| Dizziness | 14 | 0 | 10 | 0 |
| Headache | 13 | 0.2 | 13 | 0 |
| Infections and infestations | ||||
| COVID-19 | 26 | 1.7 | 24 | 1.4 |
| Conjunctivitis | 11 | 0.2 | 1.6 | 0 |
| Metabolism and nutrition disorders | ||||
| Decreased appetite | 24 | 1 | 18 | 1.4 |
| Respiratory, thoracic and mediastinal disorders | ||||
| Cough | 19 | 0 | 23 | 0 |
| Dyspnea | 14 | 1.7 | 17 | 3.5 |
| Eye disorders | ||||
| Ocular toxicity | 16 | 0.7 | 7 | 0 |
| Psychiatric disorders | ||||
| Insomnia | 10 | 0 | 11 | 0 |
Clinically relevant adverse reactions occurring in < 10% of patients who received LAZCLUZE in combination with amivantamab included skin ulcer (applicable to amivantamab) and ILD/pneumonitis.
Table 4 summarizes the laboratory abnormalities in MARIPOSA.
| Laboratory Abnormality | LAZCLUZE in combination with amivantamab
(N=421) |
Osimertinib
(N=428) |
||
|---|---|---|---|---|
| All Grades
(%) |
Grade 3 or 4
(%) |
All Grades
(%) |
Grade 3 or 4
(%) |
|
| Chemistry | ||||
| Decreased albumin | 89 | 8 | 22 | 0.2 |
| Increased ALT | 65 | 7 | 29 | 2.6 |
| Increased AST | 52 | 3.8 | 36 | 1.9 |
| Increased alkaline phosphatase | 45 | 0.5 | 15 | 0.5 |
| Decreased calcium (corrected) | 41 | 1.4 | 27 | 0.7 |
| Increased GGT | 39 | 2.6 | 24 | 1.9 |
| Decreased sodium | 38 | 7 | 35 | 5 |
| Decreased potassium | 30 | 5 | 15 | 1.2 |
| Increased creatinine | 26 | 0.7 | 35 | 0.7 |
| Decreased magnesium | 25 | 0.7 | 10 | 0.2 |
| Increased magnesium | 12 | 2.6 | 20 | 4.8 |
| Hematology | ||||
| Decreased platelet count | 52 | 0.7 | 57 | 1.4 |
| Decreased hemoglobin | 47 | 3.8 | 56 | 1.9 |
| Decreased white blood cell | 38 | 1.0 | 66 | 0.7 |
| Decreased neutrophils | 15 | 1.4 | 33 | 1.4 |
5.1 Venous Thromboembolic Events
LAZCLUZE in combination with amivantamab can cause serious and fatal venous thromboembolic events (VTE), including deep venous thrombosis (DVT) and pulmonary embolism (PE). The majority of these events occurred during the first four months of therapy [see Adverse Reactions (6.1)] .
In MARIPOSA [see Adverse Reactions (6.1)] , VTE occurred in 36% of patients receiving LAZCLUZE in combination with amivantamab, including Grade 3 in 10% and Grade 4 in 0.5% of patients. On-study VTEs occurred in 1.2% of patients (n=5) while receiving anticoagulation therapy. There were two fatal cases of VTE (0.5%), 7% of patients had VTE leading to dose interruptions of LAZCLUZE, 0.5% of patients had VTE leading to dose reductions of LAZCLUZE, and 1.9% of patients permanently discontinued LAZCLUZE due to VTE. The median time to onset of VTEs was 84 days (range: 6 to 777).
Administer prophylactic anticoagulation for the first four months of treatment [see Dosage and Administration (2.3)] . The use of Vitamin K antagonists is not recommended. Monitor for signs and symptoms of VTE and treat as medically appropriate.
Withhold LAZCLUZE and amivantamab based on severity [see Dosage and Administration (2.4)]. Once anticoagulant treatment has been initiated, resume LAZCLUZE and amivantamab at the same dose level at the discretion of the healthcare provider. In the event of VTE recurrence despite therapeutic anticoagulation, permanently discontinue amivantamab. Continue treatment with LAZCLUZE at the same dose level at the discretion of the healthcare provider [see Dosage and Administration (2.4)] . Refer to the amivantamab prescribing information for recommended amivantamab dosage modification.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise the patient to read the FDA-approved patient labeling (Patient Information).
5.3 Dermatologic Adverse Reactions
LAZCLUZE in combination with amivantamab can cause severe rash including dermatitis acneiform, pruritus and dry skin.
In MARIPOSA [see Adverse Reactions (6.1)] , rash occurred in 86% of patients treated with LAZCLUZE in combination with amivantamab, including Grade 3 in 26% of patients. The median time to onset of rash was 14 days (range: 1 to 556 days). Rash leading to dose reduction of LAZCLUZE occurred in 19% of patients, rash leading to dose interruption of LAZCLUZE occurred in 30% of patients, and LAZCLUZE was permanently discontinued due to rash in 1.7% of patients [see Adverse Reactions (6.1)].
When initiating treatment with LAZCLUZE in combination with amivantamab, prophylactic and concomitant medications are recommended to reduce the risk and severity of dermatologic adverse reactions [see Dosage and Administration (2.3)]. Instruct patients to limit sun exposure during and for 2 months after treatment with LAZCLUZE in combination with amivantamab. Advise patients to wear protective clothing and use broad-spectrum UVA/UVB sunscreen.
If skin reactions develop, administer supportive care including topical corticosteroids and topical and/or oral antibiotics. For Grade 3 reactions, administer oral steroids and consider dermatologic consultation. Promptly refer patients presenting with severe rash, atypical appearance or distribution, or lack of improvement within 2 weeks to a dermatologist. Withhold, reduce the dose or permanently discontinue LAZCLUZE and amivantamab based on severity [see Dosage and Administration (2.4)] .
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
LAZCLUZE ®(lazertinib) tablets are available in the strengths and packages listed below:
| Tablet Strength | Description | Package Configuration | NDC Number |
|---|---|---|---|
| 80 mg | Yellow, oval, film-coated, debossed with "LZ" on one side and "80" on the other side | 60-count bottle | NDC 57894-080-60 |
| 240 mg | Reddish purple, oval, film-coated, debossed with "LZ" on one side and "240" on the other side | 30-count bottle | NDC 57894-240-30 |
13.2 Animal Toxicology And/or Pharmacology (13.2 Animal Toxicology and/or Pharmacology)
In repeat-dose oral general toxicology studies up to 13-weeks duration in rats and dogs, lazertinib induced multi-organ histologic hyperplasia at exposures approximately equivalent or greater to the human exposure at the recommended dose of 240 mg. Hyperplasia was not reversible in the mandibular lymph node in the 4-week rat study. In rats, lazertinib induced renal toxicity characterized by histologic hyperplasia and inflammation in the kidney at doses ≥ 25 mg/kg (approximately 0.9 times the human exposure at the recommended dose of 240 mg/day based on AUC), along with increased urea nitrogen and histologic papillary necrosis, tubule degeneration/regeneration, and tubule dilatation at exposures approximately 4.4 times the human exposure at the recommended dose of 240 mg/day based on AUC. Increased urea nitrogen, papillary necrosis, and tubule dilatation showed evidence of recovery. In the 13-week toxicology study in dogs, one high dose animal exhibited unilateral tubule cell renal carcinoma at 8 mg/kg/day (approximately 2 times the human exposure at the recommended dose of 240 mg/day based on AUC). Other renal findings in high dose dogs included tubule degeneration/regeneration and infarct, which showed evidence of recovery. In the 4-week toxicology study, lazertinib induced cardiac toxicity in two dogs characterized by histologic findings in the heart (degeneration/necrosis of the myocardium and vessels, fibrosis, hemorrhage, thrombus, mixed cell/vessel inflammation) at 20 mg/kg (approximately 4.8 times the clinical AUC at the 240 mg human dose). One of these dogs also exhibited increased cardiac troponin I and premature ventricular complexes. These cardiac findings were not seen after a 2-week recovery period.
2.4 Dosage Modifications for Adverse Reactions
The recommended LAZCLUZE dose reductions for adverse reactions are presented in Table 1.
| Dose at which the adverse reaction occurred | 1 st Dose Reduction | 2 nd Dose Reduction | 3 rd Dose Reduction |
|---|---|---|---|
| 240 mg once daily
(one 240 mg tablet) |
160 mg once daily
(two 80 mg tablets) |
80 mg once daily
(one 80 mg tablet) |
Discontinue LAZCLUZE |
The recommended management and dosage modifications of LAZCLUZE for specific adverse reactions are presented in Table 2. Refer to the amivantamab prescribing information for information about dosage modifications for amivantamab.
| Adverse Reaction | Severity | Dosage Modification |
|---|---|---|
| Venous Thromboembolic Events (VTE)
[see Warnings and Precautions (5.1)] |
Grade 2 or 3 |
|
| Grade 4 or recurrent Grade 2 or 3 despite therapeutic level anticoagulation |
|
|
| Interstitial Lung Disease (ILD)/Pneumonitis
[see Warnings and Precautions (5.2)] |
Any Grade |
|
| Dermatologic Adverse Reactions (including dermatitis acneiform, pruritus, dry skin) [see Warnings and Precautions (5.3)] | Grade 1 |
|
| Grade 2 |
|
|
| Grade 3 |
|
|
| Grade 4
(including severe bullous, blistering or exfoliating skin conditions) |
|
|
| Other Adverse Reactions [see Adverse Reactions (6.1)] | Grade 3–4 |
|
5.2 Interstitial Lung Disease (ild)/pneumonitis (5.2 Interstitial Lung Disease (ILD)/Pneumonitis)
LAZCLUZE in combination with amivantamab can cause interstitial lung disease (ILD)/pneumonitis.
In MARIPOSA [see Adverse Reactions (6.1)], ILD/pneumonitis occurred in 3.1% of patients treated with LAZCLUZE in combination with amivantamab, including Grade 3 in 1.0% and Grade 4 in 0.2% of patients. There was one fatal case (0.2%) of ILD/pneumonitis and 2.9% of patients permanently discontinued LAZCLUZE and amivantamab due to ILD/pneumonitis [see Adverse Reactions (6.1)].
Monitor patients for new or worsening symptoms indicative of ILD/pneumonitis (e.g., dyspnea, cough, fever). Immediately withhold LAZCLUZE and amivantamab in patients with suspected ILD/pneumonitis and permanently discontinue if ILD/pneumonitis is confirmed [see Dosage and Administration (2.4)].
8.3 Females and Males of Reproductive Potential
Based on animal data and its mechanism of action, LAZCLUZE can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)] .
Principal Display Panel 80 Mg Tablet Bottle Carton (PRINCIPAL DISPLAY PANEL - 80 mg Tablet Bottle Carton)
NDC 57894-080-60
Lazcluze™
(lazertinib)
tablets
80 mg
Each film-coated tablet contains
80 mg of lazertinib equivalent to
93.86 mg lazertinib mesylate
(on anhydrous basis).
Rx only
60 film-coated tablets
janssen
Principal Display Panel 240 Mg Tablet Bottle Carton (PRINCIPAL DISPLAY PANEL - 240 mg Tablet Bottle Carton)
NDC 57894-240-30
Lazcluze™
(lazertinib)
tablets
240 mg
Each film-coated tablet contains
240 mg of lazertinib equivalent
to 281.58 mg lazertinib mesylate
(on anhydrous basis).
Rx only
30 film-coated tablets
janssen
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with lazertinib.
Lazertinib was not genotoxic in an in vitro bacterial reverse mutation (Ames) assay, an in vitro chromosomal aberration assay, or an in vivo micronucleus assay in rats.
In a dedicated fertility and early embryonic development study, male and female rats received oral doses of 7.5, 15, or 30 mg/kg/day of lazertinib. Males were dosed for 10 weeks (29 days prior to pairing, during mating period and continuing post-pairing). Females were dosed for 15 days prior to pairing, during mating period and up to Gestation Day 7. Lazertinib did not have clear effects on estrous cyclicity, mating, fertility, or sperm parameters, but induced an increase in post-implantation loss and decreased number of live fetuses at 30 mg/kg/day (approximately 1.2 times the recommended human dose of 240 mg based on body surface area). In repeat-dose oral general toxicology studies up to 13-weeks duration, lazertinib induced histologic tubular degeneration in the testis; cellular lumen debris, degeneration/necrosis, and reduced sperm in the epididymis; decreased corpora lutea in the ovary; and atrophy in the uterus and vagina. These effects were observed at exposures approximately equivalent to the human exposure at the recommended dose of 240 mg in males, and at exposures approximately 2 times the human exposure at the recommended dose of 240 mg dose in females. Findings in female reproductive organs were reversible. The tubular degeneration in the testis observed in rats at exposures approximately 4 times the human exposure at the recommended dose was not reversible within a 2-week recovery period.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:49:02.882936 · Updated: 2026-03-14T22:37:42.596050