albuterol tablets, usp
c3fa0068-fd12-45de-818e-e929fb45ba05
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Drug Interactions
The concomitant use of albuterol tablets and other oral sympathomimetic agents is not recommended since such combined use may lead to deleterious cardiovascular effects. This recommendation does not preclude the judicious use of an aerosol bronchodilator of the adrenergic stimulant type in patients receiving albuterol tablets. Such concomitant use, however, should be individualized and not given on a routine basis. If regular coadministration is required, then alternative therapy should be considered.
Description
Albuterol tablets, USP contain albuterol sulfate, USP, the racemic form of albuterol and a relatively selective beta 2 -adrenergic bronchodilator. Albuterol sulfate has the chemical name α 1 -[( tert -Butylamino)methyl]- 4-hydroxy- m -xylene-α,α'-diol sulfate (2:1) (salt) and the following structural formula: The molecular weight of albuterol sulfate is 576.71, and the molecular formula is (C 13 H 21 NO 3 ) 2 •H 2 SO 4 . Albuterol sulfate, USP is a white or practically white powder. It is freely soluble in water, slightly soluble in alcohol, in chloroform and in ether. The World Health Organization recommended name for albuterol base is salbutamol. Each albuterol tablet, USP for oral administration contains 2 mg or 4 mg of albuterol as 2.4 mg or 4.8 mg of albuterol sulfate, USP respectively and following inactive ingredients: colloidal silicon dioxide, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, pregelatinized starch (botanical source: maize) and sodium starch glycolate. FDA approved dissolution specification differs from the USP dissolution specification.
Medication Information
Warnings
Paradoxical Bronchospasm
Albuterol tablets can produce paradoxical bronchospasm, which may be life threatening. If paradoxical bronchospasm occurs, albuterol tablets should be discontinued immediately and alternative therapy instituted.
Deterioration of Asthma
Asthma may deteriorate acutely over a period of hours, or chronically over several days or longer. If the patient needs more doses of albuterol tablets than usual, this may be a marker of destabilization of asthma and requires reevaluation of the patient and the treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, e.g., corticosteroids.
Use of Anti-Inflammatory Agents
The use of beta-adrenergic agonist bronchodilators alone may not be adequate to control asthma in many patients. Early consideration should be given to adding anti-inflammatory agents, e.g., corticosteroids.
Cardiovascular Effects
Albuterol tablets, like all other beta-adrenergic agonists, can produce a clinically significant cardiovascular effect in some patients as measured by pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of albuterol tablets at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce electrocardiogram (ECG) changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Therefore, albuterol tablets, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension.
Immediate Hypersensitivity Reactions
Immediate hypersensitivity reactions may occur after administration of albuterol, as demonstrated by rare cases of urticaria, angioedema, rash, bronchospasm, anaphylaxis and oropharyngeal edema.
Rarely, erythema multiforme and Stevens-Johnson syndrome have been associated with the administration of oral albuterol sulfate in children.
Drug Interactions
The concomitant use of albuterol tablets and other oral sympathomimetic agents is not recommended since such combined use may lead to deleterious cardiovascular effects. This recommendation does not preclude the judicious use of an aerosol bronchodilator of the adrenergic stimulant type in patients receiving albuterol tablets. Such concomitant use, however, should be individualized and not given on a routine basis. If regular coadministration is required, then alternative therapy should be considered.
Description
Albuterol tablets, USP contain albuterol sulfate, USP, the racemic form of albuterol and a relatively selective beta 2 -adrenergic bronchodilator. Albuterol sulfate has the chemical name α 1 -[( tert -Butylamino)methyl]- 4-hydroxy- m -xylene-α,α'-diol sulfate (2:1) (salt) and the following structural formula: The molecular weight of albuterol sulfate is 576.71, and the molecular formula is (C 13 H 21 NO 3 ) 2 •H 2 SO 4 . Albuterol sulfate, USP is a white or practically white powder. It is freely soluble in water, slightly soluble in alcohol, in chloroform and in ether. The World Health Organization recommended name for albuterol base is salbutamol. Each albuterol tablet, USP for oral administration contains 2 mg or 4 mg of albuterol as 2.4 mg or 4.8 mg of albuterol sulfate, USP respectively and following inactive ingredients: colloidal silicon dioxide, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, pregelatinized starch (botanical source: maize) and sodium starch glycolate. FDA approved dissolution specification differs from the USP dissolution specification.
Section 42229-5
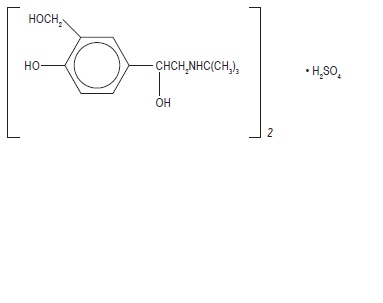
Albuterol tablets, USP contain albuterol sulfate, USP, the racemic form of albuterol and a relatively selective beta2 -adrenergic bronchodilator. Albuterol sulfate has the chemical name α1-[(tert-Butylamino)methyl]- 4-hydroxy-m-xylene-α,α'-diol sulfate (2:1) (salt) and the following structural formula:
The molecular weight of albuterol sulfate is 576.71, and the molecular formula is (C13H21NO3)2 •H2SO4. Albuterol sulfate, USP is a white or practically white powder. It is freely soluble in water, slightly soluble in alcohol, in chloroform and in ether.
The World Health Organization recommended name for albuterol base is salbutamol.
Each albuterol tablet, USP for oral administration contains 2 mg or 4 mg of albuterol as 2.4 mg or 4.8 mg of albuterol sulfate, USP respectively and following inactive ingredients: colloidal silicon dioxide, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, pregelatinized starch (botanical source: maize) and sodium starch glycolate.
FDA approved dissolution specification differs from the USP dissolution specification.
Digoxin
Mean decreases of 16% to 22% in serum digoxin levels were demonstrated after single-dose intravenous and oral administration of albuterol, respectively, to normal volunteers who had received digoxin for 10 days. The clinical significance of these findings for patients with obstructive airway disease who are receiving albuterol and digoxin on a chronic basis is unclear. Nevertheless, it would be prudent to carefully evaluate the serum digoxin levels in patients who are currently receiving digoxin and albuterol.
Monoamine Oxidase Inhibitors or Tricyclic Antidepressants
Albuterol should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents, because the action of albuterol on the vascular system may be potentiated.
General
Albuterol, as with all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension; in patients with convulsive disorders, hyperthyroidism, or diabetes mellitus; and in patients who are unusually responsive to sympathomimetic amines. Clinically significant changes in systolic and diastolic blood pressure have been seen and could be expected to occur in some patients after use of any beta-adrenergic bronchodilator.
Large doses of intravenous albuterol have been reported to aggravate preexisting diabetes mellitus and ketoacidosis. As with other beta-agonists, albuterol may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease is usually transient, not requiring supplementation.
Diuretics
The ECG changes and/or hypokalemia that may result from the administration of nonpotassium-sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the coadministration of beta-agonists with nonpotassium-sparing diuretics.
Pregnancy
Teratogenic Effects
Albuterol has been shown to be teratogenic in mice. A study in CD-1 mice at subcutaneous (sc) doses at and above 0.25mg/kg (corresponding to less than the maximum recommended daily oral dose for adults on a mg/m2 basis), induced cleft palate formation in 5 of 111 (4.5%) fetuses. At an sc dose of 2.5 mg/kg (corresponding to less than the maximum recommended daily oral dose for adults on an mg/m2 basis) albuterol sulfate induced cleft palate formation in 10 of 108 (9.3%) fetuses. The drug did not induce cleft palate formation when administered at an sc dose, 0.025 mg/kg (significantly less than the maximum recommended daily oral dose for adults on an mg/m2 basis). Cleft palate also occurred in 22 of 72 (30.5%) fetuses from females treated with 2.5 mg/kg of isoproterenol (positive control) subcutaneously.
A reproduction study in Stride Dutch rabbits revealed cranioschisis in 7 of 19 (37%) fetuses when albuterol was administered orally at a dose of 50 mg/kg (approximately 25 times the maximum recommended daily oral dose for adults on an mg/m2 basis).
Studies in pregnant rats with tritiated albuterol demonstrated that approximately 10% of the circulating maternal drug is transferred to the fetus. Disposition in the fetal lungs is comparable to maternal lungs, but fetal liver disposition is 1% of the maternal liver levels.
There are no adequate and well-controlled studies in pregnant women. Because animal
reproduction studies are not always predictive of human response, albuterol should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
During worldwide marketing experience, various congenital anomalies, including cleft palate and limb defects, have been reported in the offspring of patients being treated with albuterol. Some of the mothers were taking multiple medications during their pregnancies. Because no consistent pattern of defects can be discerned, a relationship between albuterol use and congenital anomalies has not been established.
Tocolysis
Albuterol has not been approved for the management of preterm labor. The benefit/risk ratio when albuterol is administered for tocolysis has not been established. Serious adverse reactions, including maternal pulmonary edema, have been reported during or following treatment of premature labor with beta2-agonists, including albuterol.
Preclinical
Intravenous studies in rats with albuterol sulfate have demonstrated that albuterol crosses the blood-brain barrier and reaches brain concentrations amounting to approximately 5% of the plasma concentrations. In structures outside the blood-brain barrier (pineal and pituitary glands), albuterol concentrations were found to be 100 times those in the whole brain.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when beta-agonists and methylxanthines are administered concurrently. The clinical significance of these findings is unknown.
Usual Dosage
Pediatric Patients 6 to 12 Years of Age:
For pediatric patients 6 to 12 years of age, the usual dosage is 2 mg three or four times a day.
Adults and Pediatric Patients Over 12 Years of Age:
For adults and pediatric patients over 12 years of age, the usual starting dosage is 2 or 4 mg three or four times a day.
Beta Blockers
Beta-adrenergic receptor blocking agents not only block the pulmonary effect of beta-agonists, such as albuterol tablets, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances, e.g., as prophylaxis after myocardial infarction, there may be no acceptable alternatives to the use of beta-adrenergic blocking agents in patients with asthma. In this setting, cardioselective beta-blockers could be considered, although they should be administered with caution.
Pediatric Use
Safety and effectiveness of albuterol tablets have been established in pediatric patients 6 years of age and older.
Safety and effectiveness in pediatric patients below the age of 6 years for albuterol tablets have not been established.
Clinical Trials
In controlled clinical trials in patients with asthma, the onset of improvement in pulmonary function, as measured by maximum midexpiratory flow rate (MMEF), was noted within 30 minutes after a dose of albuterol tablets, with peak improvement occurring between 2 and 3 hours. In controlled clinical trials in which measurements were conducted for 6 hours, significant clinical improvement in pulmonary function (defined as maintaining a 15% or more increase in FEV1 and a 20% or more increase in MMEF over baseline values) was observed in 60% of patients at 4 hours and in 40% at 6 hours. In other single-dose, controlled clinical trials, clinically significant improvement was observed in at least 40% of the patients at 8 hours with the 4 mg albuterol tablet. No decrease in the effectiveness of albuterol tablets has been reported in patients who received long-term treatment with the drug in uncontrolled studies for periods up to 6 months.
In another controlled clinical study in asthmatic patients, it has been demonstrated that the initiation of therapy with either the 4 mg albuterol extended-release tablets dosed every 12 hours or the 2 mg albuterol tablet dosed every 6 hours, achieve therapeutically comparable effects.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because of the potential for tumorigenicity shown for albuterol in some animal studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pharmacokinetics
Albuterol is rapidly and well absorbed following oral administration.
In studies involving normal volunteers, the mean steady-state peak and trough plasma levels of albuterol were 6.7 and 3.8 ng/mL, respectively, following dosing with a 2 mg albuterol tablet every 6 hours and 14.8 and 8.6 ng/mL, respectively following dosing with a 4 mg albuterol tablet every 6 hours. Maximum albuterol plasma levels are usually obtained between 2 and 3 hours after dosing, and the elimination half-life is 5 to 6 hours. These data indicate that albuterol administered orally is dose proportional and exhibits dose independent pharmacokinetics.
It has been shown that administration of a 4 mg albuterol extended-release tablets every 12 hours and 2 mg albuterol tablets every 6 hours for 5 days gave comparable peak albuterol levels and similar extent of absorption at steady state.
In other studies, the analysis of urine samples of patients given tritiated albuterol (4 to 10 mg) orally showed that 65% to 90% of the dose was excreted over 3 days, with the majority of the dose being excreted within the first 24 hours. Sixty percent of this radioactivity was shown to be the metabolite. Feces collected over this period contained 4% of the administered dose.
Dosage Adjustment
Pediatric Patients 6 to 12 Years of Age Who Fail to Res pond to the Initial Starting
Dosage of 2 mg Four Times a Day:
For pediatric patients from 6 to 12 years of age who fail to respond to the initial starting dosage of 2 mg four times a day, the dosage may be cautiously increased stepwise, but not to exceed 24 mg/day (given in divided doses).
Adults and Pediatric Patients Over 12 Years of Age:
For adults and pediatric patients over 12 years of age, a dosage above 4 mg four times a day should be used only when the patient fails to respond to lower dose. The dosage should be cautiously increased stepwise up to a maximum of 8 mg four times a day as tolerated if a favorable response does not occur with the 4 mg initial dosage.
Elderly Patients and Those Sensitive to Beta-adrenergic Stimulators:
An initial dosage of 2 mg three or four times a day is recommended for elderly patients and for those with a history of unusual sensitivity to beta-adrenergic stimulators. If adequate bronchodilation is not obtained, dosage may be increased gradually as tolerated to as much as 8 mg three or four times a day.
The total daily dose should not exceed 24 mg per day in pediatric patients from 6 to 12 years of age and 32 mg in adults and pediatric patients over 12 years of age.
Information for Patients
Patients being treated with albuterol tablets should receive the following information and instructions. This information is intended to aid in the safe and effective use of this medication. It is not a disclosure of all possible adverse or intended effects.
The action of albuterol tablets may last up to 6 to 8 hours or longer. Albuterol tablets should not be taken more frequently than recommended. Do not increase the dose or frequency of albuterol tablets without consulting your physician. If you find that treatment with albuterol tablets becomes less effective for symptomatic relief, your symptoms get worse, and/or you need to take the product more frequently than usual, you should seek medical attention immediately. While you are taking albuterol tablets, other inhaled drugs and asthma medications should be taken only as directed by your physician. Common adverse effects include palpitations, chest pain, rapid heart rate, and tremor or nervousness. If you are pregnant or nursing, contact your physician about use of albuterol tablets. Effective and safe use of albuterol tablets includes an understanding of the way that it should be administered.
Labor and Delivery Use in Labor
Because of the potential for beta-agonist interference with uterine contractility, use of albuterol tablets for relief of bronchospasm during labor should be restricted to those patients in whom the benefits clearly outweigh the risk.
Package Label.principal Display Panel
NDC 70710-1061-1 in bottle of 100 tablets
Albuterol tablets USP, 2 mg
Rx only
100 Tablets
ZYDUS
NDC 70710-1062-1 in bottle of 100 tablets
Albuterol tablets USP, 4 mg
Rx only
100 Tablets
ZYDUS
Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 2-year study in Sprague-Dawley rats, albuterol sulfate caused a significant dose-related increase in the incidence of benign leiomyomas of the mesovarium at and above dietary doses of 2 mg/kg (corresponding to less than the maximum recommended daily oral dose for adults and children on an mg/m2 basis). In another study this effect was blocked by the coadministration of propranolol, a non-selective beta-adrenergic antagonist.
In an 18-month study in CD-1 mice albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 500 mg/kg, (approximately 65 times the maximum recommended daily oral dose for adults on an mg/m2 basis, or, approximately 50 times the maximum recommended daily oral dose for children on an mg/m2 basis). In a 22-month study in the Golden hamster, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 50 mg/kg, (approximately 8 times the maximum recommended daily oral dose for adults and children on an mg/m2 basis).
Albuterol sulfate was not mutagenic in the Ames test with or without metabolic activation using tester strains S. typhimurium TA1537, TA1538, and TA98 or E. Coli WP2, WP2uvrA, and WP67. No forward mutation was seen in yeast strain S. cerevisiae S9 nor any mitotic gene conversion in yeast strain S. cerevisiae JD1 with or without metabolic activation. Fluctuation assays in S. typhimurium TA98 and E. Coli WP2, both with metabolic activation, were negative. Albuterol sulfate was not clastogenic in a human peripheral lymphocyte assay or in an AH1 strain mouse micronucleus assay.
Reproduction studies in rats demonstrated no evidence of impaired fertility at oral doses up to 50 mg/kg (approximately 15 times the maximum recommended daily oral dose for adults on an mg/m2 basis).
Structured Label Content
Warnings (WARNINGS)
Paradoxical Bronchospasm
Albuterol tablets can produce paradoxical bronchospasm, which may be life threatening. If paradoxical bronchospasm occurs, albuterol tablets should be discontinued immediately and alternative therapy instituted.
Deterioration of Asthma
Asthma may deteriorate acutely over a period of hours, or chronically over several days or longer. If the patient needs more doses of albuterol tablets than usual, this may be a marker of destabilization of asthma and requires reevaluation of the patient and the treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, e.g., corticosteroids.
Use of Anti-Inflammatory Agents
The use of beta-adrenergic agonist bronchodilators alone may not be adequate to control asthma in many patients. Early consideration should be given to adding anti-inflammatory agents, e.g., corticosteroids.
Cardiovascular Effects
Albuterol tablets, like all other beta-adrenergic agonists, can produce a clinically significant cardiovascular effect in some patients as measured by pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of albuterol tablets at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce electrocardiogram (ECG) changes, such as flattening of the T wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Therefore, albuterol tablets, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension.
Immediate Hypersensitivity Reactions
Immediate hypersensitivity reactions may occur after administration of albuterol, as demonstrated by rare cases of urticaria, angioedema, rash, bronchospasm, anaphylaxis and oropharyngeal edema.
Rarely, erythema multiforme and Stevens-Johnson syndrome have been associated with the administration of oral albuterol sulfate in children.
Drug Interactions
The concomitant use of albuterol tablets and other oral sympathomimetic agents is not recommended since such combined use may lead to deleterious cardiovascular effects. This recommendation does not preclude the judicious use of an aerosol bronchodilator of the adrenergic stimulant type in patients receiving albuterol tablets. Such concomitant use, however, should be individualized and not given on a routine basis. If regular coadministration is required, then alternative therapy should be considered.
Section 42229-5 (42229-5)
Albuterol tablets, USP contain albuterol sulfate, USP, the racemic form of albuterol and a relatively selective beta2 -adrenergic bronchodilator. Albuterol sulfate has the chemical name α1-[(tert-Butylamino)methyl]- 4-hydroxy-m-xylene-α,α'-diol sulfate (2:1) (salt) and the following structural formula:
The molecular weight of albuterol sulfate is 576.71, and the molecular formula is (C13H21NO3)2 •H2SO4. Albuterol sulfate, USP is a white or practically white powder. It is freely soluble in water, slightly soluble in alcohol, in chloroform and in ether.
The World Health Organization recommended name for albuterol base is salbutamol.
Each albuterol tablet, USP for oral administration contains 2 mg or 4 mg of albuterol as 2.4 mg or 4.8 mg of albuterol sulfate, USP respectively and following inactive ingredients: colloidal silicon dioxide, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone, pregelatinized starch (botanical source: maize) and sodium starch glycolate.
FDA approved dissolution specification differs from the USP dissolution specification.
Digoxin
Mean decreases of 16% to 22% in serum digoxin levels were demonstrated after single-dose intravenous and oral administration of albuterol, respectively, to normal volunteers who had received digoxin for 10 days. The clinical significance of these findings for patients with obstructive airway disease who are receiving albuterol and digoxin on a chronic basis is unclear. Nevertheless, it would be prudent to carefully evaluate the serum digoxin levels in patients who are currently receiving digoxin and albuterol.
Monoamine Oxidase Inhibitors or Tricyclic Antidepressants
Albuterol should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents, because the action of albuterol on the vascular system may be potentiated.
General
Albuterol, as with all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension; in patients with convulsive disorders, hyperthyroidism, or diabetes mellitus; and in patients who are unusually responsive to sympathomimetic amines. Clinically significant changes in systolic and diastolic blood pressure have been seen and could be expected to occur in some patients after use of any beta-adrenergic bronchodilator.
Large doses of intravenous albuterol have been reported to aggravate preexisting diabetes mellitus and ketoacidosis. As with other beta-agonists, albuterol may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease is usually transient, not requiring supplementation.
Diuretics
The ECG changes and/or hypokalemia that may result from the administration of nonpotassium-sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the coadministration of beta-agonists with nonpotassium-sparing diuretics.
Pregnancy
Teratogenic Effects
Albuterol has been shown to be teratogenic in mice. A study in CD-1 mice at subcutaneous (sc) doses at and above 0.25mg/kg (corresponding to less than the maximum recommended daily oral dose for adults on a mg/m2 basis), induced cleft palate formation in 5 of 111 (4.5%) fetuses. At an sc dose of 2.5 mg/kg (corresponding to less than the maximum recommended daily oral dose for adults on an mg/m2 basis) albuterol sulfate induced cleft palate formation in 10 of 108 (9.3%) fetuses. The drug did not induce cleft palate formation when administered at an sc dose, 0.025 mg/kg (significantly less than the maximum recommended daily oral dose for adults on an mg/m2 basis). Cleft palate also occurred in 22 of 72 (30.5%) fetuses from females treated with 2.5 mg/kg of isoproterenol (positive control) subcutaneously.
A reproduction study in Stride Dutch rabbits revealed cranioschisis in 7 of 19 (37%) fetuses when albuterol was administered orally at a dose of 50 mg/kg (approximately 25 times the maximum recommended daily oral dose for adults on an mg/m2 basis).
Studies in pregnant rats with tritiated albuterol demonstrated that approximately 10% of the circulating maternal drug is transferred to the fetus. Disposition in the fetal lungs is comparable to maternal lungs, but fetal liver disposition is 1% of the maternal liver levels.
There are no adequate and well-controlled studies in pregnant women. Because animal
reproduction studies are not always predictive of human response, albuterol should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
During worldwide marketing experience, various congenital anomalies, including cleft palate and limb defects, have been reported in the offspring of patients being treated with albuterol. Some of the mothers were taking multiple medications during their pregnancies. Because no consistent pattern of defects can be discerned, a relationship between albuterol use and congenital anomalies has not been established.
Tocolysis
Albuterol has not been approved for the management of preterm labor. The benefit/risk ratio when albuterol is administered for tocolysis has not been established. Serious adverse reactions, including maternal pulmonary edema, have been reported during or following treatment of premature labor with beta2-agonists, including albuterol.
Preclinical
Intravenous studies in rats with albuterol sulfate have demonstrated that albuterol crosses the blood-brain barrier and reaches brain concentrations amounting to approximately 5% of the plasma concentrations. In structures outside the blood-brain barrier (pineal and pituitary glands), albuterol concentrations were found to be 100 times those in the whole brain.
Studies in laboratory animals (minipigs, rodents, and dogs) have demonstrated the occurrence of cardiac arrhythmias and sudden death (with histologic evidence of myocardial necrosis) when beta-agonists and methylxanthines are administered concurrently. The clinical significance of these findings is unknown.
Usual Dosage
Pediatric Patients 6 to 12 Years of Age:
For pediatric patients 6 to 12 years of age, the usual dosage is 2 mg three or four times a day.
Adults and Pediatric Patients Over 12 Years of Age:
For adults and pediatric patients over 12 years of age, the usual starting dosage is 2 or 4 mg three or four times a day.
Beta Blockers (Beta-Blockers)
Beta-adrenergic receptor blocking agents not only block the pulmonary effect of beta-agonists, such as albuterol tablets, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances, e.g., as prophylaxis after myocardial infarction, there may be no acceptable alternatives to the use of beta-adrenergic blocking agents in patients with asthma. In this setting, cardioselective beta-blockers could be considered, although they should be administered with caution.
Pediatric Use
Safety and effectiveness of albuterol tablets have been established in pediatric patients 6 years of age and older.
Safety and effectiveness in pediatric patients below the age of 6 years for albuterol tablets have not been established.
Clinical Trials
In controlled clinical trials in patients with asthma, the onset of improvement in pulmonary function, as measured by maximum midexpiratory flow rate (MMEF), was noted within 30 minutes after a dose of albuterol tablets, with peak improvement occurring between 2 and 3 hours. In controlled clinical trials in which measurements were conducted for 6 hours, significant clinical improvement in pulmonary function (defined as maintaining a 15% or more increase in FEV1 and a 20% or more increase in MMEF over baseline values) was observed in 60% of patients at 4 hours and in 40% at 6 hours. In other single-dose, controlled clinical trials, clinically significant improvement was observed in at least 40% of the patients at 8 hours with the 4 mg albuterol tablet. No decrease in the effectiveness of albuterol tablets has been reported in patients who received long-term treatment with the drug in uncontrolled studies for periods up to 6 months.
In another controlled clinical study in asthmatic patients, it has been demonstrated that the initiation of therapy with either the 4 mg albuterol extended-release tablets dosed every 12 hours or the 2 mg albuterol tablet dosed every 6 hours, achieve therapeutically comparable effects.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because of the potential for tumorigenicity shown for albuterol in some animal studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pharmacokinetics
Albuterol is rapidly and well absorbed following oral administration.
In studies involving normal volunteers, the mean steady-state peak and trough plasma levels of albuterol were 6.7 and 3.8 ng/mL, respectively, following dosing with a 2 mg albuterol tablet every 6 hours and 14.8 and 8.6 ng/mL, respectively following dosing with a 4 mg albuterol tablet every 6 hours. Maximum albuterol plasma levels are usually obtained between 2 and 3 hours after dosing, and the elimination half-life is 5 to 6 hours. These data indicate that albuterol administered orally is dose proportional and exhibits dose independent pharmacokinetics.
It has been shown that administration of a 4 mg albuterol extended-release tablets every 12 hours and 2 mg albuterol tablets every 6 hours for 5 days gave comparable peak albuterol levels and similar extent of absorption at steady state.
In other studies, the analysis of urine samples of patients given tritiated albuterol (4 to 10 mg) orally showed that 65% to 90% of the dose was excreted over 3 days, with the majority of the dose being excreted within the first 24 hours. Sixty percent of this radioactivity was shown to be the metabolite. Feces collected over this period contained 4% of the administered dose.
Dosage Adjustment
Pediatric Patients 6 to 12 Years of Age Who Fail to Res pond to the Initial Starting
Dosage of 2 mg Four Times a Day:
For pediatric patients from 6 to 12 years of age who fail to respond to the initial starting dosage of 2 mg four times a day, the dosage may be cautiously increased stepwise, but not to exceed 24 mg/day (given in divided doses).
Adults and Pediatric Patients Over 12 Years of Age:
For adults and pediatric patients over 12 years of age, a dosage above 4 mg four times a day should be used only when the patient fails to respond to lower dose. The dosage should be cautiously increased stepwise up to a maximum of 8 mg four times a day as tolerated if a favorable response does not occur with the 4 mg initial dosage.
Elderly Patients and Those Sensitive to Beta-adrenergic Stimulators:
An initial dosage of 2 mg three or four times a day is recommended for elderly patients and for those with a history of unusual sensitivity to beta-adrenergic stimulators. If adequate bronchodilation is not obtained, dosage may be increased gradually as tolerated to as much as 8 mg three or four times a day.
The total daily dose should not exceed 24 mg per day in pediatric patients from 6 to 12 years of age and 32 mg in adults and pediatric patients over 12 years of age.
Information for Patients
Patients being treated with albuterol tablets should receive the following information and instructions. This information is intended to aid in the safe and effective use of this medication. It is not a disclosure of all possible adverse or intended effects.
The action of albuterol tablets may last up to 6 to 8 hours or longer. Albuterol tablets should not be taken more frequently than recommended. Do not increase the dose or frequency of albuterol tablets without consulting your physician. If you find that treatment with albuterol tablets becomes less effective for symptomatic relief, your symptoms get worse, and/or you need to take the product more frequently than usual, you should seek medical attention immediately. While you are taking albuterol tablets, other inhaled drugs and asthma medications should be taken only as directed by your physician. Common adverse effects include palpitations, chest pain, rapid heart rate, and tremor or nervousness. If you are pregnant or nursing, contact your physician about use of albuterol tablets. Effective and safe use of albuterol tablets includes an understanding of the way that it should be administered.
Labor and Delivery Use in Labor (Labor and Delivery-Use in Labor)
Because of the potential for beta-agonist interference with uterine contractility, use of albuterol tablets for relief of bronchospasm during labor should be restricted to those patients in whom the benefits clearly outweigh the risk.
Package Label.principal Display Panel (PACKAGE LABEL.PRINCIPAL DISPLAY PANEL)
NDC 70710-1061-1 in bottle of 100 tablets
Albuterol tablets USP, 2 mg
Rx only
100 Tablets
ZYDUS
NDC 70710-1062-1 in bottle of 100 tablets
Albuterol tablets USP, 4 mg
Rx only
100 Tablets
ZYDUS
Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 2-year study in Sprague-Dawley rats, albuterol sulfate caused a significant dose-related increase in the incidence of benign leiomyomas of the mesovarium at and above dietary doses of 2 mg/kg (corresponding to less than the maximum recommended daily oral dose for adults and children on an mg/m2 basis). In another study this effect was blocked by the coadministration of propranolol, a non-selective beta-adrenergic antagonist.
In an 18-month study in CD-1 mice albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 500 mg/kg, (approximately 65 times the maximum recommended daily oral dose for adults on an mg/m2 basis, or, approximately 50 times the maximum recommended daily oral dose for children on an mg/m2 basis). In a 22-month study in the Golden hamster, albuterol sulfate showed no evidence of tumorigenicity at dietary doses of up to 50 mg/kg, (approximately 8 times the maximum recommended daily oral dose for adults and children on an mg/m2 basis).
Albuterol sulfate was not mutagenic in the Ames test with or without metabolic activation using tester strains S. typhimurium TA1537, TA1538, and TA98 or E. Coli WP2, WP2uvrA, and WP67. No forward mutation was seen in yeast strain S. cerevisiae S9 nor any mitotic gene conversion in yeast strain S. cerevisiae JD1 with or without metabolic activation. Fluctuation assays in S. typhimurium TA98 and E. Coli WP2, both with metabolic activation, were negative. Albuterol sulfate was not clastogenic in a human peripheral lymphocyte assay or in an AH1 strain mouse micronucleus assay.
Reproduction studies in rats demonstrated no evidence of impaired fertility at oral doses up to 50 mg/kg (approximately 15 times the maximum recommended daily oral dose for adults on an mg/m2 basis).
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:38:51.794923 · Updated: 2026-03-14T21:55:56.047430