Valsartan And Hydrochlorothiazide Tablets Usp
be008c6a-6036-4abf-a3fc-450465c88d55
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Valsartan and hydrochlorothiazide tablet USP is the combination tablet of valsartan, an angiotensin II receptor blocker (ARB) and hydrochlorothiazide (HCTZ), a diuretic. Valsartan and hydrochlorothiazide tablet USP is indicated for the treatment of hypertension, to lower blood pressure: • In patients not adequately controlled with monotherapy ( 1 ) • As initial therapy in patients likely to need multiple drugs to achieve their blood pressure goals ( 1 ) Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions.
Dosage and Administration
Dose once daily. Titrate as needed to a maximum dose of 320/25 mg ( 2 ) • May be used as add-on/switch therapy for patients not adequately controlled on any of the components (valsartan or HCTZ) ( 2 ) • May be substituted for titrated components ( 2.3 )
Contraindications
Anuria; Hypersensitivity to any sulfonamide-derived drugs or any component; Do not coadminister aliskiren with valsartan and hydrochlorothiazide tablets in patients with diabetes ( 4 )
Warnings and Precautions
Hypotension: Correct volume depletion prior to initiation ( 5.2 ) • Observe for signs of fluid or electrolyte imbalance ( 5.9 ) • Monitor renal function and potassium in susceptible patients ( 5.3 , 5.7 ) • Exacerbation or activation of systemic lupus erythematosus ( 5.5 ) • Acute angle-closure glaucoma ( 5.8 )
Adverse Reactions
The most common reasons for discontinuation of therapy with Valsartan and hydrochlorothiazide were headache and dizziness. The only adverse experience that occurred in ≥2% of patients treated with valsartan and hydrochlorothiazide and at a higher incidence than placebo was nasopharyngitis (2.4% vs. 1.9%) ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Lupin Pharmaceuticals, Inc. at 1-800-399-2561 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Antidiabetic drugs: Dosage adjustment of antidiabetic may be required ( 7 ) • Cholestyramine and colestipol: Reduced absorption of thiazides ( 12.3 ) • Lithium: Increased risk of lithium toxicity. Monitor serum lithium concentrations during concurrent use. ( 7 ) • Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): May increase risk of renal impairment. Can reduce diuretic, natriuretic and antihypertensive effects of diuretics. ( 7 ) • Dual inhibition of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia ( 7 )
Description
WARNING: FETAL TOXICITY See full prescribing information for complete boxed warning. • When pregnancy is detected, discontinue valsartan and hydrochlorothiazide tablets as soon as possible. ( 5.1 ) • Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. ( 5.1 )
Medication Information
Recent Major Changes
WARNING: FETAL TOXICITY
See full prescribing information for complete boxed warning.
Warnings and Precautions
Hypotension: Correct volume depletion prior to initiation ( 5.2 ) • Observe for signs of fluid or electrolyte imbalance ( 5.9 ) • Monitor renal function and potassium in susceptible patients ( 5.3 , 5.7 ) • Exacerbation or activation of systemic lupus erythematosus ( 5.5 ) • Acute angle-closure glaucoma ( 5.8 )
Indications and Usage
Valsartan and hydrochlorothiazide tablet USP is the combination tablet of valsartan, an angiotensin II receptor blocker (ARB) and hydrochlorothiazide (HCTZ), a diuretic. Valsartan and hydrochlorothiazide tablet USP is indicated for the treatment of hypertension, to lower blood pressure: • In patients not adequately controlled with monotherapy ( 1 ) • As initial therapy in patients likely to need multiple drugs to achieve their blood pressure goals ( 1 ) Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions.
Dosage and Administration
Dose once daily. Titrate as needed to a maximum dose of 320/25 mg ( 2 ) • May be used as add-on/switch therapy for patients not adequately controlled on any of the components (valsartan or HCTZ) ( 2 ) • May be substituted for titrated components ( 2.3 )
Contraindications
Anuria; Hypersensitivity to any sulfonamide-derived drugs or any component; Do not coadminister aliskiren with valsartan and hydrochlorothiazide tablets in patients with diabetes ( 4 )
Adverse Reactions
The most common reasons for discontinuation of therapy with Valsartan and hydrochlorothiazide were headache and dizziness. The only adverse experience that occurred in ≥2% of patients treated with valsartan and hydrochlorothiazide and at a higher incidence than placebo was nasopharyngitis (2.4% vs. 1.9%) ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Lupin Pharmaceuticals, Inc. at 1-800-399-2561 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Antidiabetic drugs: Dosage adjustment of antidiabetic may be required ( 7 ) • Cholestyramine and colestipol: Reduced absorption of thiazides ( 12.3 ) • Lithium: Increased risk of lithium toxicity. Monitor serum lithium concentrations during concurrent use. ( 7 ) • Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): May increase risk of renal impairment. Can reduce diuretic, natriuretic and antihypertensive effects of diuretics. ( 7 ) • Dual inhibition of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia ( 7 )
Description
WARNING: FETAL TOXICITY See full prescribing information for complete boxed warning. • When pregnancy is detected, discontinue valsartan and hydrochlorothiazide tablets as soon as possible. ( 5.1 ) • Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. ( 5.1 )
Section 42229-5
Section 42230-3
FDA-Approved Patient Labeling
PATIENT INFORMATION
Valsartan and Hydrochlorothiazide Tablets USP
(val-SAR-tan and HYE-droe-KLOR-oh-THYE-a-zide)
Rx only
Read the Patient Information that comes with valsartan and hydrochlorothiazide tablets before you start taking it and each time you get a refill. There may be new information. This leaflet does not take the place of talking with your doctor about your condition and treatment. If you have any questions about valsartan and hydrochlorothiazide tablets, ask your doctor or pharmacist.
8.1 Pregnancy
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue valsartan and hydrochlorothiazide as soon as possible. These adverse outcomes are usually associated with use of these drugs in the second and third trimester of pregnancy. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents. Appropriate management of maternal hypertension during pregnancy is important to optimize outcomes for both mother and fetus.
In the unusual case that there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system for a particular patient, apprise the mother of the potential risk to the fetus. Perform serial ultrasound examinations to assess the intra-amniotic environment. If oligohydramnios is observed, discontinue valsartan and hydrochlorothiazide, unless it is considered lifesaving for the mother. Fetal testing may be appropriate, based on the week of pregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury. Closely observe infants with histories of in utero exposure to valsartan and hydrochlorothiazide for hypotension, oliguria, and hyperkalemia [see USE IN SPECIFIC POPULATIONS (8.4)].
Hydrochlorothiazide:
Thiazides can cross the placenta, and concentrations reached in the umbilical vein approach those in the maternal plasma. Hydrochlorothiazide, like other diuretics, can cause placental hypoperfusion. It accumulates in the amniotic fluid, with reported concentrations up to 19 times higher than in umbilical vein plasma. Use of thiazides during pregnancy is associated with a risk of fetal or neonatal jaundice or thrombocytopenia. Since they do not prevent or alter the course of EPH (Edema, Proteinuria, Hypertension) gestosis (pre-eclampsia), these drugs should not be used to treat hypertension in pregnant women. The use of hydrochlorothiazide for other indications (e.g., heart disease) in pregnancy should be avoided.
14.1 Hypertension
Valsartan-Hydrochlorothiazide
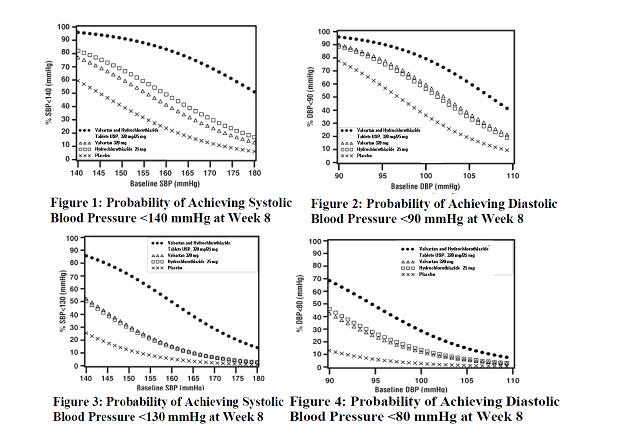
In controlled clinical trials including over 7600 patients, 4372 patients were exposed to valsartan (80, 160, and 320 mg) and concomitant hydrochlorothiazide (12.5 and 25 mg). Two factorial trials compared various combinations of 80/12.5 mg, 80/25 mg, 160/12.5 mg, 160/25 mg, 320/12.5 mg, and 320/25 mg with their respective components and placebo. The combination of valsartan and hydrochlorothiazide resulted in additive placebo-adjusted decreases in systolic and diastolic blood pressure at trough of 14 to 21/8 to 11 mmHg at 80/12.5 mg to 320/25 mg, compared to 7 to 10/4 to 5 mmHg for valsartan 80 mg to 320 mg and 5 to 11/2 to 5 mmHg for hydrochlorothiazide 12.5 mg to 25 mg, alone.
Three other controlled trials investigated the addition of hydrochlorothiazide to patients who did not respond adequately to valsartan 80 mg to valsartan 320 mg, resulted in the additional lowering of systolic and diastolic blood pressure by approximately 4 to 12/2 to 5 mmHg.
The maximal antihypertensive effect was attained 4 weeks after the initiation of therapy, the first time point at which blood pressure was measured in these trials.
In long-term follow-up studies (without placebo control) the effect of the combination of valsartan and hydrochlorothiazide appeared to be maintained for up to 2 years. The antihypertensive effect is independent of age or gender. The overall response to the combination was similar for black and non-black patients.
There was essentially no change in heart rate in patients treated with the combination of valsartan and hydrochlorothiazide in controlled trials.
There are no trials of the valsartan and hydrochlorothiazide combination tablet demonstrating reductions in cardiovascular risk in patients with hypertension, but the hydrochlorothiazide component and several ARBs, which are the same pharmacological class as the valsartan component, have demonstrated such benefits.
Valsartan
The antihypertensive effects of valsartan were demonstrated principally in 7 placebo-controlled, 4- to 12-week trials (1 in patients over 65 years) of dosages from 10 to 320 mg/day in patients with baseline diastolic blood pressures of 95 to 115 mmHg. The studies allowed comparison of once-daily and twice-daily regimens of 160 mg/day; comparison of peak and trough effects; comparison (in pooled data) of response by gender, age, and race; and evaluation of incremental effects of hydrochlorothiazide.
8.4 Pediatric Use
Safety and effectiveness of valsartan and hydrochlorothiazide in pediatric patients have not been established.
Neonates with a history of in utero exposure to valsartan and hydrochlorothiazide
If oliguria or hypotension occurs, direct attention toward support of blood pressure and renal perfusion. Exchange transfusions or dialysis may be required as a means of reversing hypotension and/or substituting for disordered renal function.
8.5 Geriatric Use
In the controlled clinical trials of valsartan and hydrochlorothiazide, 764 (17.5%) patients treated with valsartan-hydrochlorothiazide were ≥65 years and 118 (2.7%) were ≥75 years. No overall difference in the efficacy or safety of valsartan-hydrochlorothiazide was observed between these patients and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
2.2 Add On Therapy
A patient whose blood pressure is not adequately controlled with valsartan (or another ARB) alone or hydrochlorothiazide alone may be switched to combination therapy with valsartan and hydrochlorothiazide tablets USP.
A patient who experiences dose-limiting adverse reactions on either component alone may be switched to valsartan and hydrochlorothiazide tablets USP containing a lower dose of that component in combination with the other to achieve similar blood pressure reductions. The clinical response to valsartan and hydrochlorothiazide tablets USP should be subsequently evaluated and if blood pressure remains uncontrolled after 3 to 4 weeks of therapy, the dose may be titrated up to a maximum of 320/25 mg.
5.1 Fetal Toxicity
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue valsartan and hydrochlorothiazide as soon as possible. [see USE IN SPECIFIC POPULATIONS (8.1)].
Intrauterine exposure to thiazide diuretics is associated with fetal or neonatal jaundice, thrombocytopenia, and possibly other adverse reactions that have occurred in adults.
2.4 Initial Therapy
Valsartan and hydrochlorothiazide tablets USP are not recommended as initial therapy in patients with intravascular volume depletion [see WARNINGS AND PRECAUTIONS (5.2)].
4 Contraindications
Anuria; Hypersensitivity to any sulfonamide-derived drugs or any component;
Do not coadminister aliskiren with valsartan and hydrochlorothiazide tablets in patients with diabetes (4)
6 Adverse Reactions
The most common reasons for discontinuation of therapy with Valsartan and hydrochlorothiazide were headache and dizziness. The only adverse experience that occurred in ≥2% of patients treated with valsartan and hydrochlorothiazide and at a higher incidence than placebo was nasopharyngitis (2.4% vs. 1.9%) (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Lupin Pharmaceuticals, Inc. at 1-800-399-2561 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions
Antidiabetic drugs: Dosage adjustment of antidiabetic may be required (7)
-
•Cholestyramine and colestipol: Reduced absorption of thiazides (12.3)
-
•Lithium: Increased risk of lithium toxicity. Monitor serum lithium concentrations during concurrent use. (7)
-
•Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): May increase risk of renal impairment. Can reduce diuretic, natriuretic and antihypertensive effects of diuretics. (7)
-
•Dual inhibition of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7)
8.3 Nursing Mothers
It is not known whether valsartan is excreted in human milk. Valsartan was excreted into the milk of lactating rats; however, animal breast milk drug levels may not accurately reflect human breast milk levels. Hydrochlorothiazide is excreted in human breast milk. Because many drugs are excreted into human milk and because of the potential for adverse reactions in nursing infants from valsartan and hydrochlorothiazide, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
8.6 Renal Impairment
Safety and effectiveness of valsartan and hydrochlorothiazide in patients with severe renal impairment (CrCl ≤ 30 mL/min) have not been established. No dose adjustment is required in patients with mild (CrCl 60 to 90 mL/min) or moderate (CrCl 30 to 60 mL/min) renal impairment.
12.2 Pharmacodynamics
Valsartan
Valsartan inhibits the pressor effect of angiotensin II infusions. An oral dose of 80 mg inhibits the pressor effect by about 80% at peak with approximately 30% inhibition persisting for 24 hours. No information on the effect of larger doses is available.
Removal of the negative feedback of angiotensin II causes a 2- to 3-fold rise in plasma renin and consequent rise in angiotensin II plasma concentration in hypertensive patients. Minimal decreases in plasma aldosterone were observed after administration of valsartan; very little effect on serum potassium was observed.
Hydrochlorothiazide
After oral administration of hydrochlorothiazide, diuresis begins within 2 hours, peaks in about 4 hours and lasts about 6 to 12 hours.
Drug Interactions
Hydrochlorothiazide:
Alcohol, Barbiturates, or Narcotics: Potentiation of orthostatic hypotension may occur.
Skeletal Muscle Relaxants: Possible increased responsiveness to muscle relaxants such as curare derivatives.
Digitalis Glycosides: Thiazide-induced hypokalemia or hypomagnesemia may predispose the patient to digoxin toxicity.
12.3 Pharmacokinetics
Valsartan
Valsartan peak plasma concentration is reached 2 to 4 hours after dosing. Valsartan shows bi-exponential decay kinetics following intravenous administration, with an average elimination half-life of about 6 hours. Absolute bioavailability for the capsule formulation is about 25% (range 10% to 35%). Food decreases the exposure (as measured by AUC) to valsartan by about 40% and peak plasma concentration (Cmax) by about 50%. AUC and Cmax values of valsartan increase approximately linearly with increasing dose over the clinical dosing range. Valsartan does not accumulate appreciably in plasma following repeated administration.
Hydrochlorothiazide
The estimated absolute bioavailability of hydrochlorothiazide after oral administration is about 70%. Peak plasma hydrochlorothiazide concentrations (Cmax) are reached within 2 to 5 hours after oral administration. There is no clinically significant effect of food on the bioavailability of hydrochlorothiazide.
Hydrochlorothiazide binds to albumin (40% to 70%) and distributes into erythrocytes. Following oral administration, plasma hydrochlorothiazide concentrations decline bi-exponentially, with a mean distribution half-life of about 2 hours and an elimination half-life of about 10 hours.
Valsartan and Hydrochlorothiazide Tablets
Valsartan and hydrochlorothiazide tablets may be administered with or without food.
8.7 Hepatic Impairment
Valsartan
No dose adjustment is necessary for patients with mild-to-moderate liver disease. No dosing recommendations can be provided for patients with severe liver disease.
Hydrochlorothiazide
Minor alterations of fluid and electrolyte balance may precipitate hepatic coma in patients with impaired hepatic function or progressive liver disease.
1 Indications and Usage
Valsartan and hydrochlorothiazide tablet USP is the combination tablet of valsartan, an angiotensin II receptor blocker (ARB) and hydrochlorothiazide (HCTZ), a diuretic.
Valsartan and hydrochlorothiazide tablet USP is indicated for the treatment of hypertension, to lower blood pressure:
-
•In patients not adequately controlled with monotherapy (1)
-
•As initial therapy in patients likely to need multiple drugs to achieve their blood pressure goals (1)
Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions.
2.3 Replacement Therapy
Valsartan and hydrochlorothiazide tablets USP may be substituted for the titrated components.
5.6 Lithium Interaction
Increases in serum lithium concentrations and lithium toxicity have been reported with concomitant use of valsartan or thiazide diuretics. Monitor lithium levels in patients receiving valsartan and hydrochlorothiazide and lithium [see DRUG INTERACTIONS (7)].
12.1 Mechanism of Action
Angiotensin II is formed from angiotensin I in a reaction catalyzed by angiotensin-converting enzyme (ACE, kininase II). Angiotensin II is the principal pressor agent of the renin-angiotensin system, with effects that include vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac stimulation, and renal reabsorption of sodium. Valsartan blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in many tissues, such as vascular smooth muscle and the adrenal gland. Its action is therefore independent of the pathways for angiotensin II synthesis.
There is also an AT2 receptor found in many tissues, but AT2 is not known to be associated with cardiovascular homeostasis. Valsartan has much greater affinity (about 20000-fold) for the AT1 receptor than for the AT2 receptor. The primary metabolite of valsartan is essentially inactive with an affinity for the AT1 receptor about one 200th that of valsartan itself.
2.1 General Considerations
The usual starting dose is valsartan and hydrochlorothiazide tablets USP, 160/12.5 mg once daily. The dosage can be increased after 1 to 2 weeks of therapy to a maximum of one 320/25 tablet once daily as needed to control blood pressure [see CLINICAL STUDIES (14.2)]. Maximum antihypertensive effects are attained within 2 to 4 weeks after a change in dose.
5 Warnings and Precautions
5.9 Metabolic Disturbances
Hydrochlorothiazide
Hydrochlorothiazide may alter glucose tolerance and raise serum levels of cholesterol and triglycerides.
Hydrochlorothiazide may raise the serum uric acid level due to reduced clearance of uric acid and may cause or exacerbate hyperuricemia and precipitate gout in susceptible patients.
Hydrochlorothiazide decreases urinary calcium excretion and may cause elevations of serum calcium. Monitor calcium levels in patients with hypercalcemia receiving valsartan and hydrochlorothiazide.
2 Dosage and Administration
5.3 Impaired Renal Function
Changes in renal function including acute renal failure can be caused by drugs that inhibit the renin-angiotensin system and by diuretics. Patients whose renal function may depend in part on the activity of the renin-angiotensin system (e.g. patients with renal artery stenosis, chronic kidney disease, severe congestive heart failure, or volume depletion) may be at particular risk of developing acute renal failure on valsartan and hydrochlorothiazide. Monitor renal function periodically in these patients. Consider withholding or discontinuing therapy in patients who develop a clinically significant decrease in renal function on valsartan and hydrochlorothiazide [see DRUG INTERACTIONS (7)].
5.7 Potassium Abnormalities
Valsartan-Hydrochlorothiazide
In the controlled trials of various doses of valsartan and hydrochlorothiazide the incidence of hypertensive patients who developed hypokalemia (serum potassium <3.5 mEq/L) was 3%; the incidence of hyperkalemia (serum potassium >5.7 mEq/L) was 0.4%.
Hydrochlorothiazide can cause hypokalemia and hyponatremia. Hypomagnesemia can result in hypokalemia which appears difficult to treat despite potassium repletion. Drugs that inhibit the renin-angiotensin system can cause hyperkalemia. Monitor serum electrolytes periodically.
If hypokalemia is accompanied by clinical signs (e.g., muscular weakness, paresis, or ECG alterations), valsartan and hydrochlorothiazide should be discontinued. Correction of hypokalemia and any coexisting hypomagnesemia is recommended prior to the initiation of thiazides.
Some patients with heart failure have developed increases in potassium with valsartan therapy. These effects are usually minor and transient, and they are more likely to occur in patients with pre-existing renal impairment. Dosage reduction and/or discontinuation of the diuretic and/or valsartan may be required [see ADVERSE REACTIONS (6.1)].
3 Dosage Forms and Strengths
Tablets (valsartan/HCTZ mg): 80/12.5, 160/12.5, 160/25, 320/12.5, 320/25 (3)
6.2 Postmarketing Experience
The following additional adverse reactions have been reported in valsartan or valsartan/hydrochlorothiazide postmarketing experience. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Hypersensitivity
There are rare reports of angioedema. Some of these patients previously experienced angioedema with other drugs including ACE inhibitors. Valsartan and hydrochlorothiazide tablets should not be re-administered to patients who have had angioedema.
Digestive
Elevated liver enzymes and very rare reports of hepatitis
Renal
Impaired renal function
Clinical Laboratory Tests
Hyperkalemia
Dermatologic
Alopecia, bullous dermatitis
Vascular
Vasculitis
Nervous System
Syncope
Rare cases of rhabdomyolysis have been reported in patients receiving angiotensin II receptor blockers.
Hydrochlorothiazide:
The following additional adverse reactions have been reported in postmarketing experience with hydrochlorothiazide:
Acute renal failure, renal disorder, aplastic anemia, erythema multiforme, pyrexia, muscle spasm, asthenia, acute angle-closure glaucoma, bone marrow failure, worsening of diabetes control, hypokalemia, blood lipids increased, hyponatremia, hypomagnesemia, hypercalcemia, hypochloremic alkalosis, impotence, and visual impairment.
Pathological changes in the parathyroid gland of patients with hypercalcemia and hypophosphatemia have been observed in a few patients on prolonged thiazide therapy. If hypercalcemia occurs, further diagnostic evaluation is necessary.
5.4 Hypersensitivity Reaction
Hydrochlorothiazide
Hypersensitivity reactions to hydrochlorothiazide may occur in patients with or without a history of allergy or bronchial asthma, but are more likely in patients with such a history.
8 Use in Specific Populations
Nursing Mothers: Nursing or drug should be discontinued (8.3)
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reactions rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice. The adverse reaction information from clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
Hypertension
Valsartan and hydrochlorothiazide has been evaluated for safety in more than 5700 patients, including over 990 treated for over 6 months, and over 370 for over 1 year. Adverse experiences have generally been mild and transient in nature and have only infrequently required discontinuation of therapy. The overall incidence of adverse reactions with valsartan and hydrochlorothiazide was comparable to placebo.
The overall frequency of adverse reactions was neither dose-related nor related to gender, age, or race. In controlled clinical trials, discontinuation of therapy due to side effects was required in 2.3% of valsartan-hydrochlorothiazide patients and 3.1% of placebo patients. The most common reasons for discontinuation of therapy with valsartan and hydrochlorothiazide were headache and dizziness.
The only adverse reaction that occurred in controlled clinical trials in at least 2% of patients treated with valsartan and hydrochlorothiazide and at a higher incidence in valsartan-hydrochlorothiazide (n=4372) than placebo (n=262) patients was nasopharyngitis (2.4% vs. 1.9%).
5.5 Systemic Lupus Erythematosus
Hydrochlorothiazide
Thiazide diuretics have been reported to cause exacerbation or activation of systemic lupus erythematosus.
13.3 Developmental Toxicity Studies
Valsartan-Hydrochlorothiazide
There was no evidence of teratogenicity in mice, rats, or rabbits treated orally with valsartan at doses up to 600, 100, and 10 mg/kg/day, respectively, in combination with hydrochlorothiazide at doses up to 188, 31, and 3 mg/kg/day. These non-teratogenic doses in mice, rats and rabbits, respectively, represent 9, 3.5, and 0.5 times the MRHD of valsartan and 38, 13, and 2 times the MRHD of hydrochlorothiazide on a mg/m2 basis. (Calculations assume an oral dose of 320 mg/day valsartan in combination with 25 mg/day hydrochlorothiazide and a 60-kg patient.)
Fetotoxicity was observed in association with maternal toxicity in rats and rabbits at valsartan doses of ≥200 and 10 mg/kg/day, respectively, in combination with hydrochlorothiazide doses of ≥63 and 3 mg/kg/day. Fetotoxicity in rats was considered to be related to decreased fetal weights and included fetal variations of sternebrae, vertebrae, ribs and/or renal papillae. Fetotoxicity in rabbits included increased numbers of late resorptions with resultant increases in total resorptions, postimplantation losses and decreased number of live fetuses. The no observed adverse effect doses in mice, rats and rabbits for valsartan were 600, 100, and 3 mg/kg/day, respectively, in combination with hydrochlorothiazide doses of 188, 31, and 1 mg/kg/day. These no adverse effect doses in mice, rats and rabbits, respectively, represent 9, 3, and 0.18 times the MRHD of valsartan and 38, 13, and 0.5 times the MRHD of hydrochlorothiazide on a mg/m2 basis. (Calculations assume an oral dose of 320 mg/day valsartan in combination with 25 mg/day hydrochlorothiazide and a 60-kg patient.)
Valsartan
No teratogenic effects were observed when valsartan was administered to pregnant mice and rats at oral doses up to 600 mg/kg/day and to pregnant rabbits at oral doses up to 10 mg/kg/day. However, significant decreases in fetal weight, pup birth weight, pup survival rate, and slight delays in developmental milestones were observed in studies in which parental rats were treated with valsartan at oral, maternally toxic (reduction in body weight gain and food consumption) doses of 600 mg/kg/day during organogenesis or late gestation and lactation. In rabbits, fetotoxicity (i.e., resorptions, litter loss, abortions, and low body weight) associated with maternal toxicity (mortality) was observed at doses of 5 and 10 mg/kg/day. The no observed adverse effect doses of 600, 200 and 2 mg/kg/day in mice, rats and rabbits represent 9, 6 and 0.1 times, respectively, the MRHD on a mg/m2 basis. (Calculations assume an oral dose of 320 mg/day and a 60-kg patient.)
Hydrochlorothiazide
Under the auspices of the National Toxicology Program, pregnant mice and rats that received hydrochlorothiazide via gavage at doses up to 3000 and 1000 mg/kg/day, respectively, on gestation days 6 through 15 showed no evidence of teratogenicity. These doses of hydrochlorothiazide in mice and rats represent 608 and 405 times, respectively, the MRHD on a mg/m2 basis. (Calculations assume an oral dose of 25 mg/day and a 60-kg patient.)
14.2 Initial Therapy Hypertension
The safety and efficacy of valsartan and hydrochlorothiazide as initial therapy for patients with severe hypertension (defined as a sitting diastolic blood pressure ≥110 mmHg and systolic blood pressure ≥140 mmHg off all antihypertensive therapy) was studied in a 6-week multicenter, randomized, double-blind study. Patients were randomized to either valsartan and hydrochlorothiazide (valsartan and hydrochlorothiazide 160/12.5 mg once daily) or to valsartan (160 mg once daily) and followed for blood pressure response. Patients were force-titrated at 2-week intervals. Patients on combination therapy were subsequently titrated to 160/25 mg followed by 320/25 mg valsartan/hydrochlorothiazide. Patients on monotherapy were subsequently titrated to 320 mg valsartan followed by a titration to 320 mg valsartan to maintain the blind.
The study randomized 608 patients, including 261 (43%) females, 147 (24%) blacks, and 75 (12%) ≥ 65 years of age. The mean blood pressure at baseline for the total population was 168/112 mmHg. The mean age was 52 years. After 4 weeks of therapy, reductions in systolic and diastolic blood pressure were 9/5 mmHg greater in the group treated with valsartan and hydrochlorothiazide compared to valsartan. Similar trends were seen when the patients were grouped according to gender, race, or age.
Package Label.principal Display Panel
NDC 71205-249-30
VALSARTAN AND HYDROCHLOROTHIAZIDE TABLETS USP
80 mg/12.5 mg
Rx only
Bottle of 30 Tablets
2.5 Use With Other Antihypertensive Drugs
Valsartan and hydrochlorothiazide tablets USP may be administered with other antihypertensive agents.
5.8 Acute Myopia and Secondary Angle Closure Glaucoma
Hydrochlorothiazide, a sulfonamide, can cause an idiosyncratic reaction, resulting in acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy.
5.2 Hypotension in Volume And/or Salt Depleted Patients
Excessive reduction of blood pressure was rarely seen (0.7%) in patients with uncomplicated hypertension treated with valsartan and hydrochlorothiazide in controlled trials. In patients with an activated renin-angiotensin system, such as volume- and/or salt-depleted patients receiving high doses of diuretics, symptomatic hypotension may occur. This condition should be corrected prior to administration of valsartan and hydrochlorothiazide, or the treatment should start under close medical supervision.
If hypotension occurs, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. A transient hypotensive response is not a contraindication to further treatment, which usually can be continued without difficulty once the blood pressure has stabilized.
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Valsartan-Hydrochlorothiazide
No carcinogenicity, mutagenicity, or fertility studies have been conducted with the combination of valsartan and hydrochlorothiazide. However, these studies have been conducted for valsartan as well as hydrochlorothiazide alone. Based on the preclinical safety and human pharmacokinetic studies, there is no indication of any adverse interaction between valsartan and hydrochlorothiazide.
Valsartan
There was no evidence of carcinogenicity when valsartan was administered in the diet to mice and rats for up to 2 years at doses up to 160 and 200 mg/kg/day, respectively. These doses in mice and rats are about 2.6 and 6 times, respectively, the MRHD on a mg/m2basis. (Calculations assume an oral dose of 320 mg/day and a 60-kg patient.)
Mutagenicity assays did not reveal any valsartan-related effects at either the gene or chromosome level. These assays included bacterial mutagenicity tests with Salmonella (Ames) and E. coli; a gene mutation test with Chinese hamster V79 cells; a cytogenetic test with Chinese hamster ovary cells; and a rat micronucleus test.
Valsartan had no adverse effects on the reproductive performance of male or female rats at oral doses up to 200 mg/kg/day. This dose is about 6 times the MRHD on a mg/m2basis. (Calculations assume an oral dose of 320 mg/day and a 60-kg patient.)
Hydrochlorothiazide
Two-year feeding studies in mice and rats conducted under the auspices of the National Toxicology Program (NTP) uncovered no evidence of a carcinogenic potential of hydrochlorothiazide in female mice (at doses of up to approximately 600 mg/kg/day) or in male and female rats (at doses of up to approximately 100 mg/kg/day). The NTP, however, found equivocal evidence for hepatocarcinogenicity in male mice.
Hydrochlorothiazide was not genotoxic in vitro in the Ames mutagenicity assay of Salmonella Typhimurium strains TA 98, TA 100, TA 1535, TA 1537, and TA 1538 and in the Chinese Hamster Ovary (CHO) test for chromosomal aberrations, or in vivo in assays using mouse germinal cell chromosomes, Chinese hamster bone marrow chromosomes, and the Drosophila sex-linked recessive lethal trait gene. Positive test results were obtained only in the in vitro CHO Sister Chromatid Exchange (clastogenicity) and in the Mouse Lymphoma Cell (mutagenicity) assays, using concentrations of hydrochlorothiazide from 43 to 1300 mcg/mL, and in the Aspergillus Nidulans non-disjunction assay at an unspecified concentration.
Hydrochlorothiazide had no adverse effects on the fertility of mice and rats of either sex in studies wherein these species were exposed, via their diet, to doses of up to 100 and 4 mg/kg, respectively, prior to mating and throughout gestation. These doses of hydrochlorothiazide in mice and rats represent 19 and 1.5 times, respectively, the MRHD on a mg/m2basis. (Calculations assume an oral dose of 25 mg/day and a 60-kg patient.)
Structured Label Content
Recent Major Changes (34066-1)
WARNING: FETAL TOXICITY
See full prescribing information for complete boxed warning.
Section 42229-5 (42229-5)
Section 42230-3 (42230-3)
FDA-Approved Patient Labeling
PATIENT INFORMATION
Valsartan and Hydrochlorothiazide Tablets USP
(val-SAR-tan and HYE-droe-KLOR-oh-THYE-a-zide)
Rx only
Read the Patient Information that comes with valsartan and hydrochlorothiazide tablets before you start taking it and each time you get a refill. There may be new information. This leaflet does not take the place of talking with your doctor about your condition and treatment. If you have any questions about valsartan and hydrochlorothiazide tablets, ask your doctor or pharmacist.
8.1 Pregnancy
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue valsartan and hydrochlorothiazide as soon as possible. These adverse outcomes are usually associated with use of these drugs in the second and third trimester of pregnancy. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents. Appropriate management of maternal hypertension during pregnancy is important to optimize outcomes for both mother and fetus.
In the unusual case that there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system for a particular patient, apprise the mother of the potential risk to the fetus. Perform serial ultrasound examinations to assess the intra-amniotic environment. If oligohydramnios is observed, discontinue valsartan and hydrochlorothiazide, unless it is considered lifesaving for the mother. Fetal testing may be appropriate, based on the week of pregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury. Closely observe infants with histories of in utero exposure to valsartan and hydrochlorothiazide for hypotension, oliguria, and hyperkalemia [see USE IN SPECIFIC POPULATIONS (8.4)].
Hydrochlorothiazide:
Thiazides can cross the placenta, and concentrations reached in the umbilical vein approach those in the maternal plasma. Hydrochlorothiazide, like other diuretics, can cause placental hypoperfusion. It accumulates in the amniotic fluid, with reported concentrations up to 19 times higher than in umbilical vein plasma. Use of thiazides during pregnancy is associated with a risk of fetal or neonatal jaundice or thrombocytopenia. Since they do not prevent or alter the course of EPH (Edema, Proteinuria, Hypertension) gestosis (pre-eclampsia), these drugs should not be used to treat hypertension in pregnant women. The use of hydrochlorothiazide for other indications (e.g., heart disease) in pregnancy should be avoided.
14.1 Hypertension
Valsartan-Hydrochlorothiazide
In controlled clinical trials including over 7600 patients, 4372 patients were exposed to valsartan (80, 160, and 320 mg) and concomitant hydrochlorothiazide (12.5 and 25 mg). Two factorial trials compared various combinations of 80/12.5 mg, 80/25 mg, 160/12.5 mg, 160/25 mg, 320/12.5 mg, and 320/25 mg with their respective components and placebo. The combination of valsartan and hydrochlorothiazide resulted in additive placebo-adjusted decreases in systolic and diastolic blood pressure at trough of 14 to 21/8 to 11 mmHg at 80/12.5 mg to 320/25 mg, compared to 7 to 10/4 to 5 mmHg for valsartan 80 mg to 320 mg and 5 to 11/2 to 5 mmHg for hydrochlorothiazide 12.5 mg to 25 mg, alone.
Three other controlled trials investigated the addition of hydrochlorothiazide to patients who did not respond adequately to valsartan 80 mg to valsartan 320 mg, resulted in the additional lowering of systolic and diastolic blood pressure by approximately 4 to 12/2 to 5 mmHg.
The maximal antihypertensive effect was attained 4 weeks after the initiation of therapy, the first time point at which blood pressure was measured in these trials.
In long-term follow-up studies (without placebo control) the effect of the combination of valsartan and hydrochlorothiazide appeared to be maintained for up to 2 years. The antihypertensive effect is independent of age or gender. The overall response to the combination was similar for black and non-black patients.
There was essentially no change in heart rate in patients treated with the combination of valsartan and hydrochlorothiazide in controlled trials.
There are no trials of the valsartan and hydrochlorothiazide combination tablet demonstrating reductions in cardiovascular risk in patients with hypertension, but the hydrochlorothiazide component and several ARBs, which are the same pharmacological class as the valsartan component, have demonstrated such benefits.
Valsartan
The antihypertensive effects of valsartan were demonstrated principally in 7 placebo-controlled, 4- to 12-week trials (1 in patients over 65 years) of dosages from 10 to 320 mg/day in patients with baseline diastolic blood pressures of 95 to 115 mmHg. The studies allowed comparison of once-daily and twice-daily regimens of 160 mg/day; comparison of peak and trough effects; comparison (in pooled data) of response by gender, age, and race; and evaluation of incremental effects of hydrochlorothiazide.
8.4 Pediatric Use
Safety and effectiveness of valsartan and hydrochlorothiazide in pediatric patients have not been established.
Neonates with a history of in utero exposure to valsartan and hydrochlorothiazide
If oliguria or hypotension occurs, direct attention toward support of blood pressure and renal perfusion. Exchange transfusions or dialysis may be required as a means of reversing hypotension and/or substituting for disordered renal function.
8.5 Geriatric Use
In the controlled clinical trials of valsartan and hydrochlorothiazide, 764 (17.5%) patients treated with valsartan-hydrochlorothiazide were ≥65 years and 118 (2.7%) were ≥75 years. No overall difference in the efficacy or safety of valsartan-hydrochlorothiazide was observed between these patients and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
2.2 Add On Therapy (2.2 Add-On Therapy)
A patient whose blood pressure is not adequately controlled with valsartan (or another ARB) alone or hydrochlorothiazide alone may be switched to combination therapy with valsartan and hydrochlorothiazide tablets USP.
A patient who experiences dose-limiting adverse reactions on either component alone may be switched to valsartan and hydrochlorothiazide tablets USP containing a lower dose of that component in combination with the other to achieve similar blood pressure reductions. The clinical response to valsartan and hydrochlorothiazide tablets USP should be subsequently evaluated and if blood pressure remains uncontrolled after 3 to 4 weeks of therapy, the dose may be titrated up to a maximum of 320/25 mg.
5.1 Fetal Toxicity
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue valsartan and hydrochlorothiazide as soon as possible. [see USE IN SPECIFIC POPULATIONS (8.1)].
Intrauterine exposure to thiazide diuretics is associated with fetal or neonatal jaundice, thrombocytopenia, and possibly other adverse reactions that have occurred in adults.
2.4 Initial Therapy
Valsartan and hydrochlorothiazide tablets USP are not recommended as initial therapy in patients with intravascular volume depletion [see WARNINGS AND PRECAUTIONS (5.2)].
4 Contraindications (4 CONTRAINDICATIONS)
Anuria; Hypersensitivity to any sulfonamide-derived drugs or any component;
Do not coadminister aliskiren with valsartan and hydrochlorothiazide tablets in patients with diabetes (4)
6 Adverse Reactions (6 ADVERSE REACTIONS)
The most common reasons for discontinuation of therapy with Valsartan and hydrochlorothiazide were headache and dizziness. The only adverse experience that occurred in ≥2% of patients treated with valsartan and hydrochlorothiazide and at a higher incidence than placebo was nasopharyngitis (2.4% vs. 1.9%) (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Lupin Pharmaceuticals, Inc. at 1-800-399-2561 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions (7 DRUG INTERACTIONS)
Antidiabetic drugs: Dosage adjustment of antidiabetic may be required (7)
-
•Cholestyramine and colestipol: Reduced absorption of thiazides (12.3)
-
•Lithium: Increased risk of lithium toxicity. Monitor serum lithium concentrations during concurrent use. (7)
-
•Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): May increase risk of renal impairment. Can reduce diuretic, natriuretic and antihypertensive effects of diuretics. (7)
-
•Dual inhibition of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7)
8.3 Nursing Mothers
It is not known whether valsartan is excreted in human milk. Valsartan was excreted into the milk of lactating rats; however, animal breast milk drug levels may not accurately reflect human breast milk levels. Hydrochlorothiazide is excreted in human breast milk. Because many drugs are excreted into human milk and because of the potential for adverse reactions in nursing infants from valsartan and hydrochlorothiazide, a decision should be made whether to discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.
8.6 Renal Impairment
Safety and effectiveness of valsartan and hydrochlorothiazide in patients with severe renal impairment (CrCl ≤ 30 mL/min) have not been established. No dose adjustment is required in patients with mild (CrCl 60 to 90 mL/min) or moderate (CrCl 30 to 60 mL/min) renal impairment.
12.2 Pharmacodynamics
Valsartan
Valsartan inhibits the pressor effect of angiotensin II infusions. An oral dose of 80 mg inhibits the pressor effect by about 80% at peak with approximately 30% inhibition persisting for 24 hours. No information on the effect of larger doses is available.
Removal of the negative feedback of angiotensin II causes a 2- to 3-fold rise in plasma renin and consequent rise in angiotensin II plasma concentration in hypertensive patients. Minimal decreases in plasma aldosterone were observed after administration of valsartan; very little effect on serum potassium was observed.
Hydrochlorothiazide
After oral administration of hydrochlorothiazide, diuresis begins within 2 hours, peaks in about 4 hours and lasts about 6 to 12 hours.
Drug Interactions
Hydrochlorothiazide:
Alcohol, Barbiturates, or Narcotics: Potentiation of orthostatic hypotension may occur.
Skeletal Muscle Relaxants: Possible increased responsiveness to muscle relaxants such as curare derivatives.
Digitalis Glycosides: Thiazide-induced hypokalemia or hypomagnesemia may predispose the patient to digoxin toxicity.
12.3 Pharmacokinetics
Valsartan
Valsartan peak plasma concentration is reached 2 to 4 hours after dosing. Valsartan shows bi-exponential decay kinetics following intravenous administration, with an average elimination half-life of about 6 hours. Absolute bioavailability for the capsule formulation is about 25% (range 10% to 35%). Food decreases the exposure (as measured by AUC) to valsartan by about 40% and peak plasma concentration (Cmax) by about 50%. AUC and Cmax values of valsartan increase approximately linearly with increasing dose over the clinical dosing range. Valsartan does not accumulate appreciably in plasma following repeated administration.
Hydrochlorothiazide
The estimated absolute bioavailability of hydrochlorothiazide after oral administration is about 70%. Peak plasma hydrochlorothiazide concentrations (Cmax) are reached within 2 to 5 hours after oral administration. There is no clinically significant effect of food on the bioavailability of hydrochlorothiazide.
Hydrochlorothiazide binds to albumin (40% to 70%) and distributes into erythrocytes. Following oral administration, plasma hydrochlorothiazide concentrations decline bi-exponentially, with a mean distribution half-life of about 2 hours and an elimination half-life of about 10 hours.
Valsartan and Hydrochlorothiazide Tablets
Valsartan and hydrochlorothiazide tablets may be administered with or without food.
8.7 Hepatic Impairment
Valsartan
No dose adjustment is necessary for patients with mild-to-moderate liver disease. No dosing recommendations can be provided for patients with severe liver disease.
Hydrochlorothiazide
Minor alterations of fluid and electrolyte balance may precipitate hepatic coma in patients with impaired hepatic function or progressive liver disease.
1 Indications and Usage (1 INDICATIONS AND USAGE)
Valsartan and hydrochlorothiazide tablet USP is the combination tablet of valsartan, an angiotensin II receptor blocker (ARB) and hydrochlorothiazide (HCTZ), a diuretic.
Valsartan and hydrochlorothiazide tablet USP is indicated for the treatment of hypertension, to lower blood pressure:
-
•In patients not adequately controlled with monotherapy (1)
-
•As initial therapy in patients likely to need multiple drugs to achieve their blood pressure goals (1)
Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions.
2.3 Replacement Therapy
Valsartan and hydrochlorothiazide tablets USP may be substituted for the titrated components.
5.6 Lithium Interaction
Increases in serum lithium concentrations and lithium toxicity have been reported with concomitant use of valsartan or thiazide diuretics. Monitor lithium levels in patients receiving valsartan and hydrochlorothiazide and lithium [see DRUG INTERACTIONS (7)].
12.1 Mechanism of Action
Angiotensin II is formed from angiotensin I in a reaction catalyzed by angiotensin-converting enzyme (ACE, kininase II). Angiotensin II is the principal pressor agent of the renin-angiotensin system, with effects that include vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac stimulation, and renal reabsorption of sodium. Valsartan blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in many tissues, such as vascular smooth muscle and the adrenal gland. Its action is therefore independent of the pathways for angiotensin II synthesis.
There is also an AT2 receptor found in many tissues, but AT2 is not known to be associated with cardiovascular homeostasis. Valsartan has much greater affinity (about 20000-fold) for the AT1 receptor than for the AT2 receptor. The primary metabolite of valsartan is essentially inactive with an affinity for the AT1 receptor about one 200th that of valsartan itself.
2.1 General Considerations
The usual starting dose is valsartan and hydrochlorothiazide tablets USP, 160/12.5 mg once daily. The dosage can be increased after 1 to 2 weeks of therapy to a maximum of one 320/25 tablet once daily as needed to control blood pressure [see CLINICAL STUDIES (14.2)]. Maximum antihypertensive effects are attained within 2 to 4 weeks after a change in dose.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
5.9 Metabolic Disturbances
Hydrochlorothiazide
Hydrochlorothiazide may alter glucose tolerance and raise serum levels of cholesterol and triglycerides.
Hydrochlorothiazide may raise the serum uric acid level due to reduced clearance of uric acid and may cause or exacerbate hyperuricemia and precipitate gout in susceptible patients.
Hydrochlorothiazide decreases urinary calcium excretion and may cause elevations of serum calcium. Monitor calcium levels in patients with hypercalcemia receiving valsartan and hydrochlorothiazide.
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
5.3 Impaired Renal Function
Changes in renal function including acute renal failure can be caused by drugs that inhibit the renin-angiotensin system and by diuretics. Patients whose renal function may depend in part on the activity of the renin-angiotensin system (e.g. patients with renal artery stenosis, chronic kidney disease, severe congestive heart failure, or volume depletion) may be at particular risk of developing acute renal failure on valsartan and hydrochlorothiazide. Monitor renal function periodically in these patients. Consider withholding or discontinuing therapy in patients who develop a clinically significant decrease in renal function on valsartan and hydrochlorothiazide [see DRUG INTERACTIONS (7)].
5.7 Potassium Abnormalities
Valsartan-Hydrochlorothiazide
In the controlled trials of various doses of valsartan and hydrochlorothiazide the incidence of hypertensive patients who developed hypokalemia (serum potassium <3.5 mEq/L) was 3%; the incidence of hyperkalemia (serum potassium >5.7 mEq/L) was 0.4%.
Hydrochlorothiazide can cause hypokalemia and hyponatremia. Hypomagnesemia can result in hypokalemia which appears difficult to treat despite potassium repletion. Drugs that inhibit the renin-angiotensin system can cause hyperkalemia. Monitor serum electrolytes periodically.
If hypokalemia is accompanied by clinical signs (e.g., muscular weakness, paresis, or ECG alterations), valsartan and hydrochlorothiazide should be discontinued. Correction of hypokalemia and any coexisting hypomagnesemia is recommended prior to the initiation of thiazides.
Some patients with heart failure have developed increases in potassium with valsartan therapy. These effects are usually minor and transient, and they are more likely to occur in patients with pre-existing renal impairment. Dosage reduction and/or discontinuation of the diuretic and/or valsartan may be required [see ADVERSE REACTIONS (6.1)].
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Tablets (valsartan/HCTZ mg): 80/12.5, 160/12.5, 160/25, 320/12.5, 320/25 (3)
6.2 Postmarketing Experience
The following additional adverse reactions have been reported in valsartan or valsartan/hydrochlorothiazide postmarketing experience. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Hypersensitivity
There are rare reports of angioedema. Some of these patients previously experienced angioedema with other drugs including ACE inhibitors. Valsartan and hydrochlorothiazide tablets should not be re-administered to patients who have had angioedema.
Digestive
Elevated liver enzymes and very rare reports of hepatitis
Renal
Impaired renal function
Clinical Laboratory Tests
Hyperkalemia
Dermatologic
Alopecia, bullous dermatitis
Vascular
Vasculitis
Nervous System
Syncope
Rare cases of rhabdomyolysis have been reported in patients receiving angiotensin II receptor blockers.
Hydrochlorothiazide:
The following additional adverse reactions have been reported in postmarketing experience with hydrochlorothiazide:
Acute renal failure, renal disorder, aplastic anemia, erythema multiforme, pyrexia, muscle spasm, asthenia, acute angle-closure glaucoma, bone marrow failure, worsening of diabetes control, hypokalemia, blood lipids increased, hyponatremia, hypomagnesemia, hypercalcemia, hypochloremic alkalosis, impotence, and visual impairment.
Pathological changes in the parathyroid gland of patients with hypercalcemia and hypophosphatemia have been observed in a few patients on prolonged thiazide therapy. If hypercalcemia occurs, further diagnostic evaluation is necessary.
5.4 Hypersensitivity Reaction
Hydrochlorothiazide
Hypersensitivity reactions to hydrochlorothiazide may occur in patients with or without a history of allergy or bronchial asthma, but are more likely in patients with such a history.
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
Nursing Mothers: Nursing or drug should be discontinued (8.3)
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reactions rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice. The adverse reaction information from clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
Hypertension
Valsartan and hydrochlorothiazide has been evaluated for safety in more than 5700 patients, including over 990 treated for over 6 months, and over 370 for over 1 year. Adverse experiences have generally been mild and transient in nature and have only infrequently required discontinuation of therapy. The overall incidence of adverse reactions with valsartan and hydrochlorothiazide was comparable to placebo.
The overall frequency of adverse reactions was neither dose-related nor related to gender, age, or race. In controlled clinical trials, discontinuation of therapy due to side effects was required in 2.3% of valsartan-hydrochlorothiazide patients and 3.1% of placebo patients. The most common reasons for discontinuation of therapy with valsartan and hydrochlorothiazide were headache and dizziness.
The only adverse reaction that occurred in controlled clinical trials in at least 2% of patients treated with valsartan and hydrochlorothiazide and at a higher incidence in valsartan-hydrochlorothiazide (n=4372) than placebo (n=262) patients was nasopharyngitis (2.4% vs. 1.9%).
5.5 Systemic Lupus Erythematosus
Hydrochlorothiazide
Thiazide diuretics have been reported to cause exacerbation or activation of systemic lupus erythematosus.
13.3 Developmental Toxicity Studies
Valsartan-Hydrochlorothiazide
There was no evidence of teratogenicity in mice, rats, or rabbits treated orally with valsartan at doses up to 600, 100, and 10 mg/kg/day, respectively, in combination with hydrochlorothiazide at doses up to 188, 31, and 3 mg/kg/day. These non-teratogenic doses in mice, rats and rabbits, respectively, represent 9, 3.5, and 0.5 times the MRHD of valsartan and 38, 13, and 2 times the MRHD of hydrochlorothiazide on a mg/m2 basis. (Calculations assume an oral dose of 320 mg/day valsartan in combination with 25 mg/day hydrochlorothiazide and a 60-kg patient.)
Fetotoxicity was observed in association with maternal toxicity in rats and rabbits at valsartan doses of ≥200 and 10 mg/kg/day, respectively, in combination with hydrochlorothiazide doses of ≥63 and 3 mg/kg/day. Fetotoxicity in rats was considered to be related to decreased fetal weights and included fetal variations of sternebrae, vertebrae, ribs and/or renal papillae. Fetotoxicity in rabbits included increased numbers of late resorptions with resultant increases in total resorptions, postimplantation losses and decreased number of live fetuses. The no observed adverse effect doses in mice, rats and rabbits for valsartan were 600, 100, and 3 mg/kg/day, respectively, in combination with hydrochlorothiazide doses of 188, 31, and 1 mg/kg/day. These no adverse effect doses in mice, rats and rabbits, respectively, represent 9, 3, and 0.18 times the MRHD of valsartan and 38, 13, and 0.5 times the MRHD of hydrochlorothiazide on a mg/m2 basis. (Calculations assume an oral dose of 320 mg/day valsartan in combination with 25 mg/day hydrochlorothiazide and a 60-kg patient.)
Valsartan
No teratogenic effects were observed when valsartan was administered to pregnant mice and rats at oral doses up to 600 mg/kg/day and to pregnant rabbits at oral doses up to 10 mg/kg/day. However, significant decreases in fetal weight, pup birth weight, pup survival rate, and slight delays in developmental milestones were observed in studies in which parental rats were treated with valsartan at oral, maternally toxic (reduction in body weight gain and food consumption) doses of 600 mg/kg/day during organogenesis or late gestation and lactation. In rabbits, fetotoxicity (i.e., resorptions, litter loss, abortions, and low body weight) associated with maternal toxicity (mortality) was observed at doses of 5 and 10 mg/kg/day. The no observed adverse effect doses of 600, 200 and 2 mg/kg/day in mice, rats and rabbits represent 9, 6 and 0.1 times, respectively, the MRHD on a mg/m2 basis. (Calculations assume an oral dose of 320 mg/day and a 60-kg patient.)
Hydrochlorothiazide
Under the auspices of the National Toxicology Program, pregnant mice and rats that received hydrochlorothiazide via gavage at doses up to 3000 and 1000 mg/kg/day, respectively, on gestation days 6 through 15 showed no evidence of teratogenicity. These doses of hydrochlorothiazide in mice and rats represent 608 and 405 times, respectively, the MRHD on a mg/m2 basis. (Calculations assume an oral dose of 25 mg/day and a 60-kg patient.)
14.2 Initial Therapy Hypertension (14.2 Initial Therapy - Hypertension)
The safety and efficacy of valsartan and hydrochlorothiazide as initial therapy for patients with severe hypertension (defined as a sitting diastolic blood pressure ≥110 mmHg and systolic blood pressure ≥140 mmHg off all antihypertensive therapy) was studied in a 6-week multicenter, randomized, double-blind study. Patients were randomized to either valsartan and hydrochlorothiazide (valsartan and hydrochlorothiazide 160/12.5 mg once daily) or to valsartan (160 mg once daily) and followed for blood pressure response. Patients were force-titrated at 2-week intervals. Patients on combination therapy were subsequently titrated to 160/25 mg followed by 320/25 mg valsartan/hydrochlorothiazide. Patients on monotherapy were subsequently titrated to 320 mg valsartan followed by a titration to 320 mg valsartan to maintain the blind.
The study randomized 608 patients, including 261 (43%) females, 147 (24%) blacks, and 75 (12%) ≥ 65 years of age. The mean blood pressure at baseline for the total population was 168/112 mmHg. The mean age was 52 years. After 4 weeks of therapy, reductions in systolic and diastolic blood pressure were 9/5 mmHg greater in the group treated with valsartan and hydrochlorothiazide compared to valsartan. Similar trends were seen when the patients were grouped according to gender, race, or age.
Package Label.principal Display Panel (PACKAGE LABEL.PRINCIPAL DISPLAY PANEL)
NDC 71205-249-30
VALSARTAN AND HYDROCHLOROTHIAZIDE TABLETS USP
80 mg/12.5 mg
Rx only
Bottle of 30 Tablets
2.5 Use With Other Antihypertensive Drugs (2.5 Use with Other Antihypertensive Drugs)
Valsartan and hydrochlorothiazide tablets USP may be administered with other antihypertensive agents.
5.8 Acute Myopia and Secondary Angle Closure Glaucoma (5.8 Acute Myopia and Secondary Angle-Closure Glaucoma)
Hydrochlorothiazide, a sulfonamide, can cause an idiosyncratic reaction, resulting in acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy.
5.2 Hypotension in Volume And/or Salt Depleted Patients (5.2 Hypotension in Volume- and/or Salt-Depleted Patients)
Excessive reduction of blood pressure was rarely seen (0.7%) in patients with uncomplicated hypertension treated with valsartan and hydrochlorothiazide in controlled trials. In patients with an activated renin-angiotensin system, such as volume- and/or salt-depleted patients receiving high doses of diuretics, symptomatic hypotension may occur. This condition should be corrected prior to administration of valsartan and hydrochlorothiazide, or the treatment should start under close medical supervision.
If hypotension occurs, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. A transient hypotensive response is not a contraindication to further treatment, which usually can be continued without difficulty once the blood pressure has stabilized.
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Valsartan-Hydrochlorothiazide
No carcinogenicity, mutagenicity, or fertility studies have been conducted with the combination of valsartan and hydrochlorothiazide. However, these studies have been conducted for valsartan as well as hydrochlorothiazide alone. Based on the preclinical safety and human pharmacokinetic studies, there is no indication of any adverse interaction between valsartan and hydrochlorothiazide.
Valsartan
There was no evidence of carcinogenicity when valsartan was administered in the diet to mice and rats for up to 2 years at doses up to 160 and 200 mg/kg/day, respectively. These doses in mice and rats are about 2.6 and 6 times, respectively, the MRHD on a mg/m2basis. (Calculations assume an oral dose of 320 mg/day and a 60-kg patient.)
Mutagenicity assays did not reveal any valsartan-related effects at either the gene or chromosome level. These assays included bacterial mutagenicity tests with Salmonella (Ames) and E. coli; a gene mutation test with Chinese hamster V79 cells; a cytogenetic test with Chinese hamster ovary cells; and a rat micronucleus test.
Valsartan had no adverse effects on the reproductive performance of male or female rats at oral doses up to 200 mg/kg/day. This dose is about 6 times the MRHD on a mg/m2basis. (Calculations assume an oral dose of 320 mg/day and a 60-kg patient.)
Hydrochlorothiazide
Two-year feeding studies in mice and rats conducted under the auspices of the National Toxicology Program (NTP) uncovered no evidence of a carcinogenic potential of hydrochlorothiazide in female mice (at doses of up to approximately 600 mg/kg/day) or in male and female rats (at doses of up to approximately 100 mg/kg/day). The NTP, however, found equivocal evidence for hepatocarcinogenicity in male mice.
Hydrochlorothiazide was not genotoxic in vitro in the Ames mutagenicity assay of Salmonella Typhimurium strains TA 98, TA 100, TA 1535, TA 1537, and TA 1538 and in the Chinese Hamster Ovary (CHO) test for chromosomal aberrations, or in vivo in assays using mouse germinal cell chromosomes, Chinese hamster bone marrow chromosomes, and the Drosophila sex-linked recessive lethal trait gene. Positive test results were obtained only in the in vitro CHO Sister Chromatid Exchange (clastogenicity) and in the Mouse Lymphoma Cell (mutagenicity) assays, using concentrations of hydrochlorothiazide from 43 to 1300 mcg/mL, and in the Aspergillus Nidulans non-disjunction assay at an unspecified concentration.
Hydrochlorothiazide had no adverse effects on the fertility of mice and rats of either sex in studies wherein these species were exposed, via their diet, to doses of up to 100 and 4 mg/kg, respectively, prior to mating and throughout gestation. These doses of hydrochlorothiazide in mice and rats represent 19 and 1.5 times, respectively, the MRHD on a mg/m2basis. (Calculations assume an oral dose of 25 mg/day and a 60-kg patient.)
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:34:54.038288 · Updated: 2026-03-14T21:41:42.903926