Emend For Injection
8d66803a-6811-4c29-9c57-e16acfa87f21
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
EMEND ® for injection, in combination with other antiemetic agents, is indicated in adults and pediatric patients 6 months of age and older for the prevention of: acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy (HEC) including high-dose cisplatin. delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic cancer chemotherapy (MEC).
Dosage and Administration
Recommended Adult Dosage ( 2.1 ) EMEND for injection 150 mg on Day 1 as an intravenous infusion over 20 to 30 minutes. ( 2.1 ) Complete the infusion approximately 30 minutes prior to chemotherapy. Recommended Dosage for Pediatric Patients (6 months to 17 years) Weighing at Least 6 kg ( 2.2 ) See Full Prescribing Information for pediatric dosage regimens by age. For single dose chemotherapy regimens : single dose of EMEND for injection on Day 1. For single- or multi-day chemotherapy regimens : 3-day EMEND regimen of EMEND for injection on Days 1, 2, and 3. EMEND capsules or EMEND for oral suspension may be used as an alternative on Days 2 and 3. Administer EMEND for injection through a central venous catheter as an intravenous infusion over 30 minutes (12 years to 17 years) or 60 minutes (6 months to less than 12 years). Complete the infusion approximately 30 minutes prior to chemotherapy. Concomitant Antiemetics See Full Prescribing Information for additional information. ( 2.1 , 2.2 )
Contraindications
EMEND is contraindicated in patients: who are hypersensitive to any component of the product. Hypersensitivity reactions including anaphylactic reactions, flushing, erythema, and dyspnea have been reported [see Warnings and Precautions (5.2) , Adverse Reactions (6.2) ] . taking pimozide. Inhibition of CYP3A4 by aprepitant, the active moiety, could result in elevated plasma concentrations of this drug, which is a CYP3A4 substrate, potentially causing serious or life-threatening reactions, such as QT prolongation, a known adverse reaction of pimozide [see Warnings and Precautions (5.1) ].
Warnings and Precautions
CYP3A4 Interactions: Fosaprepitant is a weak inhibitor of CYP3A4, and aprepitant, the active moiety, is a substrate, inhibitor, and inducer of CYP3A4; see Full Prescribing Information for recommendations regarding contraindications, risk of adverse reactions, and dosage adjustment of EMEND and concomitant drugs. ( 4 , 5.1 , 7.1 , 7.2 ) Hypersensitivity Reactions (including anaphylaxis and anaphylactic shock): May occur during or soon after infusion. If symptoms occur, discontinue the drug. Do not reinitiate EMEND if symptoms occur with previous use. ( 4 , 5.2 ) Infusion Site Reactions (including thrombophlebitis, necrosis, and vasculitis): Majority of reactions reported in patients receiving vesicant chemotherapy. Avoid infusion into small veins. Discontinue infusion and administer treatment if a severe reaction develops. ( 5.3 ) Warfarin (a CYP2C9 substrate): Risk of decreased INR of prothrombin time; monitor INR in 2–week period, particularly at 7 to 10 days, following initiation of EMEND. ( 5.4 , 7.1 ) Hormonal Contraceptives: Efficacy of contraceptives may be reduced during and for 28 days following administration of EMEND. Use effective alternative or back-up methods of contraception. ( 5.5 , 7.1 , 8.3 )
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: Hypersensitivity Reactions [see Warnings and Precautions (5.2) ] Infusion Site Reactions [see Warnings and Precautions (5.3) ]
Drug Interactions
Fosaprepitant, a prodrug of aprepitant, is a weak inhibitor of CYP3A4, and aprepitant is a substrate, inhibitor, and inducer of CYP3A4. Use of EMEND with other drugs that are CYP3A4 substrates, may result in increased plasma concentration of the concomitant drug. Use of pimozide with EMEND is contraindicated due to the risk of significantly increased plasma concentrations of pimozide, potentially resulting in prolongation of the QT interval, a known adverse reaction of pimozide [see Contraindications (4) ]. Use of EMEND with strong or moderate CYP3A4 inhibitors (e.g., ketoconazole, diltiazem) may increase plasma concentrations of aprepitant and result in an increased risk of adverse reactions related to EMEND. Use of EMEND with strong CYP3A4 inducers (e.g., rifampin) may result in a reduction in aprepitant plasma concentrations and decreased efficacy of EMEND. See Table 7 and Table 8 for a listing of potentially significant drug interactions [see Drug Interactions (7.1 , 7.2) ].
How Supplied
Single-dose glass vial containing 150 mg of fosaprepitant as a white to off-white lyophilized powder for reconstitution. Supplied as follows: NDC 0006-3061-00 1 vial per carton.
Storage and Handling
Single-dose glass vial containing 150 mg of fosaprepitant as a white to off-white lyophilized powder for reconstitution. Supplied as follows: NDC 0006-3061-00 1 vial per carton.
Description
EMEND ® for injection, in combination with other antiemetic agents, is indicated in adults and pediatric patients 6 months of age and older for the prevention of: acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy (HEC) including high-dose cisplatin. delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic cancer chemotherapy (MEC).
Medication Information
Warnings and Precautions
CYP3A4 Interactions: Fosaprepitant is a weak inhibitor of CYP3A4, and aprepitant, the active moiety, is a substrate, inhibitor, and inducer of CYP3A4; see Full Prescribing Information for recommendations regarding contraindications, risk of adverse reactions, and dosage adjustment of EMEND and concomitant drugs. ( 4 , 5.1 , 7.1 , 7.2 ) Hypersensitivity Reactions (including anaphylaxis and anaphylactic shock): May occur during or soon after infusion. If symptoms occur, discontinue the drug. Do not reinitiate EMEND if symptoms occur with previous use. ( 4 , 5.2 ) Infusion Site Reactions (including thrombophlebitis, necrosis, and vasculitis): Majority of reactions reported in patients receiving vesicant chemotherapy. Avoid infusion into small veins. Discontinue infusion and administer treatment if a severe reaction develops. ( 5.3 ) Warfarin (a CYP2C9 substrate): Risk of decreased INR of prothrombin time; monitor INR in 2–week period, particularly at 7 to 10 days, following initiation of EMEND. ( 5.4 , 7.1 ) Hormonal Contraceptives: Efficacy of contraceptives may be reduced during and for 28 days following administration of EMEND. Use effective alternative or back-up methods of contraception. ( 5.5 , 7.1 , 8.3 )
Indications and Usage
EMEND ® for injection, in combination with other antiemetic agents, is indicated in adults and pediatric patients 6 months of age and older for the prevention of: acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy (HEC) including high-dose cisplatin. delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic cancer chemotherapy (MEC).
Dosage and Administration
Recommended Adult Dosage ( 2.1 ) EMEND for injection 150 mg on Day 1 as an intravenous infusion over 20 to 30 minutes. ( 2.1 ) Complete the infusion approximately 30 minutes prior to chemotherapy. Recommended Dosage for Pediatric Patients (6 months to 17 years) Weighing at Least 6 kg ( 2.2 ) See Full Prescribing Information for pediatric dosage regimens by age. For single dose chemotherapy regimens : single dose of EMEND for injection on Day 1. For single- or multi-day chemotherapy regimens : 3-day EMEND regimen of EMEND for injection on Days 1, 2, and 3. EMEND capsules or EMEND for oral suspension may be used as an alternative on Days 2 and 3. Administer EMEND for injection through a central venous catheter as an intravenous infusion over 30 minutes (12 years to 17 years) or 60 minutes (6 months to less than 12 years). Complete the infusion approximately 30 minutes prior to chemotherapy. Concomitant Antiemetics See Full Prescribing Information for additional information. ( 2.1 , 2.2 )
Contraindications
EMEND is contraindicated in patients: who are hypersensitive to any component of the product. Hypersensitivity reactions including anaphylactic reactions, flushing, erythema, and dyspnea have been reported [see Warnings and Precautions (5.2) , Adverse Reactions (6.2) ] . taking pimozide. Inhibition of CYP3A4 by aprepitant, the active moiety, could result in elevated plasma concentrations of this drug, which is a CYP3A4 substrate, potentially causing serious or life-threatening reactions, such as QT prolongation, a known adverse reaction of pimozide [see Warnings and Precautions (5.1) ].
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: Hypersensitivity Reactions [see Warnings and Precautions (5.2) ] Infusion Site Reactions [see Warnings and Precautions (5.3) ]
Drug Interactions
Fosaprepitant, a prodrug of aprepitant, is a weak inhibitor of CYP3A4, and aprepitant is a substrate, inhibitor, and inducer of CYP3A4. Use of EMEND with other drugs that are CYP3A4 substrates, may result in increased plasma concentration of the concomitant drug. Use of pimozide with EMEND is contraindicated due to the risk of significantly increased plasma concentrations of pimozide, potentially resulting in prolongation of the QT interval, a known adverse reaction of pimozide [see Contraindications (4) ]. Use of EMEND with strong or moderate CYP3A4 inhibitors (e.g., ketoconazole, diltiazem) may increase plasma concentrations of aprepitant and result in an increased risk of adverse reactions related to EMEND. Use of EMEND with strong CYP3A4 inducers (e.g., rifampin) may result in a reduction in aprepitant plasma concentrations and decreased efficacy of EMEND. See Table 7 and Table 8 for a listing of potentially significant drug interactions [see Drug Interactions (7.1 , 7.2) ].
Storage and Handling
Single-dose glass vial containing 150 mg of fosaprepitant as a white to off-white lyophilized powder for reconstitution. Supplied as follows: NDC 0006-3061-00 1 vial per carton.
How Supplied
Single-dose glass vial containing 150 mg of fosaprepitant as a white to off-white lyophilized powder for reconstitution. Supplied as follows: NDC 0006-3061-00 1 vial per carton.
Description
EMEND ® for injection, in combination with other antiemetic agents, is indicated in adults and pediatric patients 6 months of age and older for the prevention of: acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy (HEC) including high-dose cisplatin. delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic cancer chemotherapy (MEC).
Section 42229-5
Limitations of Use
- EMEND has not been studied for the treatment of established nausea and vomiting.
Section 42230-3
| This Patient Information has been approved by the U.S. Food and Drug Administration. | Revised: May 2022 |
|
Patient Information |
|
|
Read this Patient Information before you start receiving EMEND for injection and each time you are scheduled to receive EMEND for injection. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or treatment. |
|
|
What is EMEND for injection? EMEND for injection is a prescription medicine used with other medicines that treat nausea and vomiting in patients 6 months of age and older to prevent nausea and vomiting caused by certain anti-cancer (chemotherapy) medicines.
|
|
|
Who should not receive EMEND for injection? Do not receive EMEND for injection if you:
|
|
|
What should I tell my healthcare provider before receiving EMEND for injection? Before receiving EMEND for injection, tell your healthcare provider if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. EMEND for injection may affect the way other medicines work, and other medicines may affect the way EMEND for injection works, causing serious side effects. Know the medicines you take. Keep a list of them to show your healthcare provider or pharmacist when you get a new medicine. |
|
|
How will I receive EMEND for injection? Adults 18 years of age and older: EMEND for injection will be given on Day 1 of chemotherapy treatment. It will be given to you by intravenous (IV) infusion in your vein about 50 to 60 minutes before you start your chemotherapy treatment. Children 6 months to 17 years of age: EMEND for injection will be given to your child by intravenous (IV) infusion into a large vein through a type of IV line called a central venous catheter, about 1 hour to 1 ½ hours before the start of their chemotherapy treatment. Depending on the chemotherapy treatment, there are 2 ways that EMEND for injection may be given:
If you take the blood thinner medicine warfarin sodium (COUMADIN®, JANTOVEN®), your healthcare provider may do blood tests after you receive EMEND for injection to check your blood clotting. |
|
|
What are the possible side effects of EMEND for injection? EMEND for injection may cause serious side effects, including:
In adults, the most common side effects of EMEND for injection include: |
|
|
|
|
In children 6 months to 17 years of age, the most common side effects of EMEND for injection include: |
|
|
|
|
Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all of the possible side effects of EMEND for injection. For more information ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
General information about the safe and effective use of EMEND for injection. If you would like more information about EMEND for injection, talk with your healthcare provider. You can ask your healthcare provider or pharmacist for information about EMEND for injection that is written for health professionals. For more information about EMEND for injection call 1-800-622-4477 or go to www.emend.com. |
|
|
What are the ingredients in EMEND for injection? Active ingredient: fosaprepitant Inactive ingredients: edetate disodium, polysorbate 80, lactose anhydrous, sodium hydroxide and/or hydrochloric acid (for pH adjustment) Manufactured for: Merck Sharp & Dohme LLC, Rahway, NJ 07065, USA |
Section 44425-7
Storage
Emend for injection vials must be refrigerated, store at 2°C-8°C (36°F-46°F).
The reconstituted final drug solution is stable for 24 hours at ambient room temperature [at or below 25°C (77°F)]. Discard unused portion.
10 Overdosage
There is no specific information on the treatment of overdosage with fosaprepitant or aprepitant.
In the event of overdose, EMEND should be discontinued and general supportive treatment and monitoring should be provided. Because of the antiemetic activity of EMEND, drug-induced emesis may not be effective in cases of EMEND overdosage.
Aprepitant is not removed by hemodialysis.
11 Description
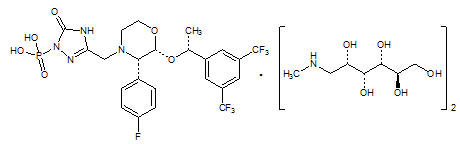
EMEND (fosaprepitant) for injection is a sterile, lyophilized formulation containing fosaprepitant dimeglumine, a prodrug of aprepitant, a substance P/neurokinin-1 (NK1) receptor antagonist, an antiemetic agent, chemically described as 1-Deoxy-1-(methylamino)-D-glucitol[3-[[(2R,3S)-2-[(1R)-1-[3,5-bis(trifluoromethyl)phenyl]ethoxy]-3-(4-fluorophenyl)-4-morpholinyl]methyl]-2,5-dihydro-5-oxo-1H-1,2,4-triazol-1-yl]phosphonate (2:1) (salt).
Its empirical formula is C23H22F7N4O6P ∙ 2(C7H17NO5) and its structural formula is:
Fosaprepitant dimeglumine is a white to off-white amorphous powder with a molecular weight of 1004.83. It is freely soluble in water.
Each vial of EMEND for injection for administration as an intravenous infusion contains 150 mg of fosaprepitant (equivalent to 245.3 mg of fosaprepitant dimeglumine) and the following inactive ingredients: edetate disodium (5.4 mg), polysorbate 80 (75 mg), lactose anhydrous (375 mg), sodium hydroxide and/or hydrochloric acid (for pH adjustment).
8.4 Pediatric Use
The safety and effectiveness of a single dose and a 3-day regimen of EMEND have been established in pediatric patients 6 months to 17 years for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of HEC and MEC.
Use of EMEND in this age group is supported by evidence from adequate and well-controlled studies of EMEND for injection in adults, with additional safety, efficacy and pharmacokinetic data in pediatric patients 6 months to 17 years. Efficacy and safety were also supported by data from an adequate and well-controlled study of a 3-day oral aprepitant regimen in pediatric patients 6 months to 17 years. The safety of the 3-day EMEND for injection regimen in pediatric patients 6 months to 17 years of age was supported by an open-label study in 100 patients receiving HEC or MEC. See the full prescribing information for EMEND capsules for complete clinical information regarding studies performed with oral aprepitant. Adverse reactions were similar to those reported in adult patients [see Dosage and Administration (2.2), Adverse Reactions (6.1), Clinical Pharmacology (12.3)].
The safety and effectiveness of EMEND for the prevention of nausea and vomiting associated with HEC or MEC have not been established in patients less than 6 months of age.
8.5 Geriatric Use
Of the 1649 adult cancer patients treated with intravenous EMEND in HEC and MEC clinical studies, 27% were aged 65 and over, while 5% were aged 75 and over. Other reported clinical experience with EMEND has not identified differences in responses between elderly and younger patients. In general, use caution when dosing elderly patients as they have a greater frequency of decreased hepatic, renal or cardiac function and concomitant disease or other drug therapy [see Clinical Pharmacology (12.3)].
4 Contraindications
EMEND is contraindicated in patients:
- who are hypersensitive to any component of the product. Hypersensitivity reactions including anaphylactic reactions, flushing, erythema, and dyspnea have been reported [see Warnings and Precautions (5.2), Adverse Reactions (6.2)].
- taking pimozide. Inhibition of CYP3A4 by aprepitant, the active moiety, could result in elevated plasma concentrations of this drug, which is a CYP3A4 substrate, potentially causing serious or life-threatening reactions, such as QT prolongation, a known adverse reaction of pimozide [see Warnings and Precautions (5.1)].
6 Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hypersensitivity Reactions [see Warnings and Precautions (5.2)]
- Infusion Site Reactions [see Warnings and Precautions (5.3)]
7 Drug Interactions
1 Indications and Usage
EMEND® for injection, in combination with other antiemetic agents, is indicated in adults and pediatric patients 6 months of age and older for the prevention of:
- acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy (HEC) including high-dose cisplatin.
- delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic cancer chemotherapy (MEC).
12.1 Mechanism of Action
Fosaprepitant is a prodrug of aprepitant and accordingly, its antiemetic effects are attributable to aprepitant.
Aprepitant is a selective high-affinity antagonist of human substance P/neurokinin 1 (NK1) receptors. Aprepitant has little or no affinity for serotonin (5-HT3), dopamine, and corticosteroid receptors, the targets of existing therapies for chemotherapy-induced nausea and vomiting (CINV). Aprepitant has been shown in animal models to inhibit emesis induced by cytotoxic chemotherapeutic agents, such as cisplatin, via central actions. Animal and human Positron Emission Tomography (PET) studies with aprepitant have shown that it crosses the blood brain barrier and occupies brain NK1 receptors. Animal and human studies have shown that aprepitant augments the antiemetic activity of the 5-HT3-receptor antagonist ondansetron and the corticosteroid dexamethasone and inhibits both the acute and delayed phases of cisplatin-induced emesis.
5 Warnings and Precautions
- CYP3A4 Interactions: Fosaprepitant is a weak inhibitor of CYP3A4, and aprepitant, the active moiety, is a substrate, inhibitor, and inducer of CYP3A4; see Full Prescribing Information for recommendations regarding contraindications, risk of adverse reactions, and dosage adjustment of EMEND and concomitant drugs. (4, 5.1, 7.1, 7.2)
- Hypersensitivity Reactions (including anaphylaxis and anaphylactic shock): May occur during or soon after infusion. If symptoms occur, discontinue the drug. Do not reinitiate EMEND if symptoms occur with previous use. (4, 5.2)
- Infusion Site Reactions (including thrombophlebitis, necrosis, and vasculitis): Majority of reactions reported in patients receiving vesicant chemotherapy. Avoid infusion into small veins. Discontinue infusion and administer treatment if a severe reaction develops. (5.3)
- Warfarin (a CYP2C9 substrate): Risk of decreased INR of prothrombin time; monitor INR in 2–week period, particularly at 7 to 10 days, following initiation of EMEND. (5.4, 7.1)
- Hormonal Contraceptives: Efficacy of contraceptives may be reduced during and for 28 days following administration of EMEND. Use effective alternative or back-up methods of contraception. (5.5, 7.1, 8.3)
2 Dosage and Administration
Recommended Adult Dosage (2.1)
- EMEND for injection 150 mg on Day 1 as an intravenous infusion over 20 to 30 minutes. (2.1)
- Complete the infusion approximately 30 minutes prior to chemotherapy.
Recommended Dosage for Pediatric Patients (6 months to 17 years) Weighing at Least 6 kg (2.2)
- See Full Prescribing Information for pediatric dosage regimens by age.
- For single dose chemotherapy regimens: single dose of EMEND for injection on Day 1.
- For single- or multi-day chemotherapy regimens: 3-day EMEND regimen of EMEND for injection on Days 1, 2, and 3. EMEND capsules or EMEND for oral suspension may be used as an alternative on Days 2 and 3.
- Administer EMEND for injection through a central venous catheter as an intravenous infusion over 30 minutes (12 years to 17 years) or 60 minutes (6 months to less than 12 years).
- Complete the infusion approximately 30 minutes prior to chemotherapy.
Concomitant Antiemetics
5.3 Infusion Site Reactions
Infusion site reactions (ISRs) have been reported with the use of EMEND for injection [see Adverse Reactions (6.1)]. The majority of severe ISRs, including thrombophlebitis and vasculitis, were reported with concomitant vesicant (anthracycline-based) chemotherapy administration, particularly when associated with extravasation. Necrosis was also reported in some patients with concomitant vesicant chemotherapy. Most ISRs occurred with the first, second or third exposure to single doses of EMEND for injection and in some cases, reactions persisted for two weeks or longer. Treatment of severe ISRs consisted of medical, and in some cases surgical, intervention.
Avoid infusion of EMEND for injection into small veins or through a butterfly catheter. If a severe ISR develops during infusion, discontinue the infusion and administer appropriate medical treatment.
3 Dosage Forms and Strengths
EMEND for injection: 150 mg fosaprepitant, white to off-white lyophilized powder in single-dose glass vial for reconstitution
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of EMEND. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and subcutaneous tissue disorders: pruritus, rash, urticaria, Stevens-Johnson syndrome/toxic epidermal necrolysis [see Warnings and Precautions (5.2)].
Immune system disorders: hypersensitivity reactions including anaphylaxis and anaphylactic shock [see Contraindications (4), Warnings and Precautions (5.2)].
Nervous system disorders: ifosfamide-induced neurotoxicity reported after EMEND and ifosfamide coadministration.
5.2 Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis and anaphylactic shock, during or soon after infusion of fosaprepitant have occurred. Symptoms including flushing, erythema, dyspnea, hypotension and syncope have been reported [see Adverse Reactions (6.2)].
Monitor patients during and after infusion. If hypersensitivity reactions occur, discontinue the infusion and administer appropriate medical therapy. Do not reinitiate EMEND in patients who experience these symptoms with previous use [see Contraindications (4)].
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The overall safety of EMEND for injection was evaluated in approximately 1800 adult and pediatric patients.
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
16 How Supplied/storage and Handling
Single-dose glass vial containing 150 mg of fosaprepitant as a white to off-white lyophilized powder for reconstitution. Supplied as follows:
| NDC 0006-3061-00 | 1 vial per carton. |
8.6 Patients With Hepatic Impairment
The pharmacokinetics of aprepitant in patients with mild and moderate hepatic impairment were similar to those of healthy subjects with normal hepatic function. No dosage adjustment is necessary for patients with mild to moderate hepatic impairment (Child-Pugh score 5 to 9). There are no clinical or pharmacokinetic data in patients with severe hepatic impairment (Child-Pugh score greater than 9). Therefore, additional monitoring for adverse reactions in these patients may be warranted when EMEND is administered [see Clinical Pharmacology (12.3)].
2.3 Preparation of Emend for Injection
| The recommended dose of EMEND for injection is based on the patient's age and weight. | |
| Step 1 | Aseptically inject 5 mL 0.9% Sodium Chloride Injection, USP into the vial. Assure that 0.9% Sodium Chloride Injection, USP is added to the vial along the vial wall in order to prevent foaming. Swirl the vial gently. Avoid shaking and jetting 0.9% Sodium Chloride Injection, USP into the vial. |
| Step 2 | Aseptically prepare an infusion bag filled with 145 mL of 0.9% Sodium Chloride Injection, USP. |
| Step 3 | Aseptically withdraw the entire volume from the vial and transfer it into the infusion bag containing 145 mL of 0.9% Sodium Chloride Injection, USP to yield a total volume of 150 mL and a final concentration of 1 mg/mL. |
| Step 4 | Gently invert the bag 2 to 3 times. |
| Step 5 | Determine the volume to be administered from this prepared infusion bag, based on the recommended dose [see Dosage and Administration (2.1, 2.2)]. Adults The entire volume of the prepared infusion bag (150 mL) should be administered. Pediatrics In patients 12 years and older, the volume to be administered is calculated as follows:
|
| Step 6 | If necessary, for volumes less than 150 mL, the calculated volume can be transferred to an appropriate size bag or syringe prior to administration by infusion. |
| Step 7 | Before administration, inspect the bag for particulate matter and discoloration. Discard the bag if particulate and/or discoloration are observed. |
Caution: Do not mix or reconstitute EMEND for injection with solutions for which physical and chemical compatibility have not been established. EMEND for injection is incompatible with any solutions containing divalent cations (e.g., Ca2+, Mg2+), including Lactated Ringer's Solution and Hartmann's Solution.
Principal Display Panel 150 Mg Vial Carton
NDC 0006-3061-00
Emend®
(fosaprepitant)
for Injection
150 mg per vial
Reconstitute with 5 mL of 0.9% Sodium
Chloride for Injection.
STERILE LYOPHILIZED POWDER
FOR INTRAVENOUS USE ONLY AFTER
RECONSTITUTION AND DILUTION
DO NOT USE WITH SOLUTIONS
CONTAINING DIVALENT CATIONS
(e.g., Ca2+, Mg2+) INCLUDING
LACTATED RINGER'S SOLUTION
AND HARTMANN'S SOLUTION.
Rx only
Single-Dose Vial –
Discard Unused Portion
5.4 Decrease in Inr With Concomitant Warfarin
Coadministration of EMEND with warfarin, a CYP2C9 substrate, may result in a clinically significant decrease in the International Normalized Ratio (INR) of prothrombin time [see Clinical Pharmacology (12.3)]. Monitor the INR in patients on chronic warfarin therapy in the 2-week period, particularly at 7 to 10 days, following initiation of EMEND with each chemotherapy cycle [see Drug Interactions (7.1)].
5.1 Clinically Significant Cyp3a4 Drug Interactions
Fosaprepitant, a prodrug of aprepitant, is a weak inhibitor of CYP3A4, and aprepitant is a substrate, inhibitor, and inducer of CYP3A4.
- Use of EMEND with other drugs that are CYP3A4 substrates, may result in increased plasma concentration of the concomitant drug.
- Use of pimozide with EMEND is contraindicated due to the risk of significantly increased plasma concentrations of pimozide, potentially resulting in prolongation of the QT interval, a known adverse reaction of pimozide [see Contraindications (4)].
- Use of EMEND with strong or moderate CYP3A4 inhibitors (e.g., ketoconazole, diltiazem) may increase plasma concentrations of aprepitant and result in an increased risk of adverse reactions related to EMEND.
- Use of EMEND with strong CYP3A4 inducers (e.g., rifampin) may result in a reduction in aprepitant plasma concentrations and decreased efficacy of EMEND.
See Table 7 and Table 8 for a listing of potentially significant drug interactions [see Drug Interactions (7.1, 7.2)].
5.5 Risk of Reduced Efficacy of Hormonal Contraceptives
Upon coadministration with EMEND, the efficacy of hormonal contraceptives may be reduced during administration of and for 28 days following the last dose of EMEND [see Clinical Pharmacology (12.3)]. Advise patients to use effective alternative or back-up methods of contraception during treatment with EMEND and for 1 month following administration of EMEND [see Drug Interactions (7.1), Use in Specific Populations (8.3)].
14.1 Prevention of Nausea and Vomiting Associated With Hec in Adults
In a randomized, parallel, double-blind, active-controlled study, EMEND for injection 150 mg as a single intravenous infusion (N=1147) was compared to a 3-day oral EMEND regimen (N=1175) in patients receiving a HEC regimen that included cisplatin (≥70 mg/m2). All patients in both groups received dexamethasone and ondansetron (see Table 12). Patient demographics were similar between the two treatment groups. Of the total 2322 patients, 63% were men, 56% White, 26% Asian, 3% American Indian/Alaska Native, 2% Black, 13% Multi-Racial, and 33% Hispanic/Latino ethnicity. Patient ages ranged from 19 to 86 years of age, with a mean age of 56 years. Other concomitant chemotherapy agents commonly administered were fluorouracil (17%), gemcitabine (16%), paclitaxel (15%), and etoposide (12%).
| Day 1 | Day 2 | Day 3 | Day 4 | |
|---|---|---|---|---|
| EMEND Regimen | ||||
| EMEND for injection | 150 mg intravenously over 20 to 30 minutes approximately 30 minutes prior to chemotherapy | none | none | none |
| Oral dexamethasone Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1 and in the morning on Days 2 through 4. Dexamethasone was also administered in the evenings on Days 3 and 4. The 12 mg dose of dexamethasone on Day 1 and the 8 mg once daily dose on Day 2 reflects a dosage adjustment to account for a drug interaction with the EMEND for injection regimen [see Clinical Pharmacology (12.3)].
|
12 mg | 8 mg | 8 mg twice daily | 8 mg twice daily |
| Ondansetron | Ondansetron Ondansetron 32 mg intravenous was used in the clinical trials of EMEND. Although this dose was used in clinical trials, this is no longer the currently recommended dose. Refer to the ondansetron prescribing information for the current recommended dose.
|
none | none | none |
| Oral EMEND Regimen | ||||
| EMEND capsules | 125 mg | 80 mg | 80 mg | none |
| Oral dexamethasone Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1 and in the morning on Days 2 through 4. The 12 mg dose of dexamethasone on Day 1 and the 8 mg once daily dose on Days 2 through 4 reflects a dosage adjustment to account for a drug interaction with the oral EMEND regimen [see Clinical Pharmacology (12.3)].
|
12 mg | 8 mg | 8 mg | 8 mg |
| Ondansetron | Ondansetron | none | none | none |
The efficacy of EMEND for injection was evaluated based on the primary and secondary endpoints listed in Table 13 and was shown to be non-inferior to that of the 3-day oral aprepitant regimen with regard to complete response in each of the evaluated phases. The pre-specified non-inferiority margin for complete response in the overall phase was 7%. The pre-specified non-inferiority margin for complete response in the delayed phase was 7.3%. The pre-specified non-inferiority margin for no vomiting in the overall phase was 8.2%.
| ENDPOINTS | EMEND for Injection Regimen (N = 1106) N: Number of patients included in the primary analysis of complete response.
% |
Oral EMEND Regimen (N = 1134) % |
Difference Difference and Confidence interval (CI) were calculated using the method proposed by Miettinen and Nurminen and adjusted for Gender.
(95% CI) |
|---|---|---|---|
| PRIMARY ENDPOINT | |||
| Complete Response Complete Response = no vomiting and no use of rescue therapy.
|
|||
| Overall Overall = 0 to 120 hours post-initiation of cisplatin chemotherapy.
|
71.9 | 72.3 | -0.4 (-4.1, 3.3) |
| SECONDARY ENDPOINTS | |||
| Complete Response | |||
| Delayed phase Delayed phase = 25 to 120 hours post-initiation of cisplatin chemotherapy.
|
74.3 | 74.2 | 0.1 (-3.5, 3.7) |
| No Vomiting | |||
| Overall | 72.9 | 74.6 | -1.7 (-5.3, 2.0) |
14.2 Prevention of Nausea and Vomiting Associated With Mec in Adults
In a randomized, parallel, double-blind, active comparator-controlled study, EMEND for injection 150 mg as a single intravenous infusion (N=502) in combination with ondansetron and dexamethasone (EMEND regimen) was compared with ondansetron and dexamethasone alone (standard therapy) (N=498) (see Table 14) in patients receiving a MEC regimen. Patient demographics were similar between the two treatment groups. Of the total 1,000 patients included in the efficacy analysis, 41% were men, 84% White, 4% Asian, 1% American Indian/Alaska Native, 2% Black, 10% Multi-Racial, and 19% Hispanic/Latino ethnicity. Patient ages ranged from 23 to 88 years of age, with a mean age of 60 years. The most commonly administered MEC chemotherapeutic agents were carboplatin (51%), oxaliplatin (24%), and cyclophosphamide (12%).
| Day 1 | Day 2 | Day 3 | |
|---|---|---|---|
| EMEND Regimen | |||
| EMEND for Injection | 150 mg intravenously over 20 to 30 minutes approximately 30 minutes prior to chemotherapy | none | none |
| Oral Dexamethasone Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1. The 12 mg dose reflects a dosage adjustment to account for a drug interaction with the EMEND for injection regimen [see Clinical Pharmacology (12.3)].
|
12 mg | none | none |
| Oral Ondansetron The first ondansetron dose was administered 30 to 60 minutes prior to chemotherapy treatment on Day 1 and the second dose was administered 8 hours after first ondansetron dose.
|
8 mg for 2 doses | none | none |
| Standard Therapy | |||
| Oral Dexamethasone | 20 mg | none | none |
| Oral Ondansetron | 8 mg for 2 doses | 8 mg twice daily | 8 mg twice daily |
The primary endpoint was complete response (defined as no vomiting and no rescue therapy) in the delayed phase (25 to 120 hours) of chemotherapy-induced nausea and vomiting. The results by treatment group are shown in Table 15.
| ENDPOINTS | EMEND for Injection Regimen (N = 502) N: Number of patients included in the intention to treat population.
% |
Standard Therapy Regimen (N = 498) % |
P-Value | Treatment Difference (95% CI) |
|---|---|---|---|---|
| PRIMARY ENDPOINT | ||||
| Complete Response Complete Response = no vomiting and no use of rescue therapy.
|
||||
| Delayed phase Delayed phase = 25 to 120 hours post-initiation of chemotherapy.
|
78.9 | 68.5 | <0.001 | 10.4 (5.1, 15.9) |
7.1 Effect of Fosaprepitant/aprepitant On the Pharmacokinetics of Other Drugs
When administered intravenously, fosaprepitant, a prodrug of aprepitant, is converted to aprepitant within 30 minutes. Therefore, drug interactions following administration of EMEND for injection are likely to occur with drugs that interact with oral aprepitant.
Fosaprepitant, given as a single 150-mg dose, is a weak inhibitor of CYP3A4, and the weak inhibition of CYP3A4 continues for 2 days after single dose administration. Single dose fosaprepitant does not induce CYP3A4. Aprepitant is a substrate, an inhibitor, and an inducer of CYP3A4. Aprepitant is also an inducer of CYP2C9 [see Clinical Pharmacology (12.3)].
Some substrates of CYP3A4 are contraindicated with EMEND [see Contraindications (4)]. Dosage adjustment of some CYP3A4 and CYP2C9 substrates may be warranted, as shown in Table 7.
| CYP3A4 Substrates | |
| Pimozide | |
| Clinical Impact | Increased pimozide exposure |
| Intervention | EMEND is contraindicated [see Contraindications (4)]. |
| Benzodiazepines | |
| Clinical Impact | Increased exposure to midazolam or other benzodiazepines metabolized via CYP3A4 (alprazolam, triazolam) may increase the risk of adverse reactions [see Clinical Pharmacology (12.3)]. |
| Intervention | Monitor for benzodiazepine-related adverse reactions. |
| Dexamethasone | |
| Clinical Impact | Increased dexamethasone exposure [see Clinical Pharmacology (12.3)]. |
| Intervention | Reduce the dose of oral dexamethasone by approximately 50% [see Dosage and Administration (2.1)]. |
| Methylprednisolone | |
| Clinical Impact | Increased methylprednisolone exposure [see Clinical Pharmacology (12.3)]. |
| Intervention | Reduce the dose of oral methylprednisolone by approximately 50% on Days 1 and 2 for patients receiving HEC and on Day 1 for patients receiving MEC. Reduce the dose of intravenous methylprednisolone by 25% on Days 1 and 2 for patients receiving HEC and on Day 1 for patients receiving MEC. |
| Chemotherapeutic agents that are metabolized by CYP3A4 | |
| Clinical Impact | Increased exposure of the chemotherapeutic agent may increase the risk of adverse reactions [see Clinical Pharmacology (12.3)]. |
| Intervention |
Vinblastine, vincristine, or ifosfamide or other chemotherapeutic agents
|
| Hormonal Contraceptives | |
| Clinical Impact | Decreased hormonal exposure during administration of and for 28 days after administration of the last dose of EMEND [see Warnings and Precautions (5.5), Use in Specific Populations (8.3), and Clinical Pharmacology (12.3)]. |
| Intervention | Effective alternative or back-up methods of contraception (such as condoms and spermicides) should be used during treatment with EMEND and for 1 month following administration of EMEND. |
| Examples | birth control pills, skin patches, implants, and certain IUDs |
| CYP2C9 Substrates | |
| Warfarin | |
| Clinical Impact | Decreased warfarin exposure and decreased prothrombin time (INR) [see Warnings and Precautions (5.4), Clinical Pharmacology (12.3)]. |
| Intervention | In patients on chronic warfarin therapy, monitor the prothrombin time (INR) in the 2-week period, particularly at 7 to 10 days, following administration of EMEND with each chemotherapy cycle. |
| Other | |
| 5-HT3 Antagonists | |
| Clinical Impact | No change in the exposure of the 5-HT3 antagonist [see Clinical Pharmacology (12.3)]. |
| Intervention | No dosage adjustment needed |
| Examples | ondansetron, granisetron, dolasetron |
7.2 Effect of Other Drugs On the Pharmacokinetics of Fosaprepitant/aprepitant
Aprepitant is a CYP3A4 substrate [see Clinical Pharmacology (12.3)]. Co-administration of EMEND with drugs that are inhibitors or inducers of CYP3A4 may result in increased or decreased plasma concentrations of aprepitant, respectively, as shown in Table 8.
| Moderate to Strong CYP3A4 Inhibitors | |
| Clinical Impact | Significantly increased exposure of aprepitant may increase the risk of adverse reactions associated with EMEND [see Adverse Reactions (6.1), Clinical Pharmacology (12.3)]. |
| Intervention | Avoid concomitant use of EMEND |
| Examples |
Moderate inhibitor:
diltiazem Strong inhibitors: ketoconazole, itraconazole, nefazodone, troleandomycin, clarithromycin, ritonavir, nelfinavir |
| Strong CYP3A4 Inducers | |
| Clinical Impact | Substantially decreased exposure of aprepitant in patients chronically taking a strong CYP3A4 inducer may decrease the efficacy of EMEND [see Clinical Pharmacology (12.3)]. |
| Intervention | Avoid concomitant use of EMEND |
| Examples | rifampin, carbamazepine, phenytoin |
2.1 Prevention of Nausea and Vomiting Associated With Hec and Mec in Adult Patients
The recommended dosage of EMEND for injection, dexamethasone, and a 5-HT3 antagonist for the prevention of nausea and vomiting associated with administration of HEC or MEC in adults is shown in Table 1 or Table 2, respectively. Administer EMEND for injection as an intravenous infusion on Day 1 over 20 to 30 minutes, completing the infusion approximately 30 minutes prior to chemotherapy.
| Day 1 | Day 2 | Day 3 | Day 4 | |
|---|---|---|---|---|
| EMEND for injection | 150 mg intravenously over 20 to 30 minutes | none | none | none |
| Dexamethasone Administer dexamethasone 30 minutes prior to chemotherapy treatment on Day 1 and in the morning on Days 2 through 4. Also administer dexamethasone in the evenings on Days 3 and 4. A 50% dosage reduction of dexamethasone on Days 1 and 2 is recommended to account for a drug interaction with EMEND [see Clinical Pharmacology (12.3)].
|
12 mg orally | 8 mg orally | 8 mg orally twice daily | 8 mg orally twice daily |
| 5-HT3 antagonist | See selected 5-HT3 antagonist prescribing information for the recommended dosage | none | none | none |
| Day 1 | |
|---|---|
| EMEND for injection | 150 mg intravenously over 20 to 30 minutes |
| Dexamethasone Administer dexamethasone 30 minutes prior to chemotherapy treatment on Day 1. A 50% dosage reduction of dexamethasone is recommended to account for a drug interaction with EMEND [see Clinical Pharmacology (12.3)].
|
12 mg orally |
| 5-HT3 antagonist | See selected 5-HT3 antagonist prescribing information for the recommended dosage |
2.2 Prevention of Nausea and Vomiting Associated With Hec and Mec in Pediatric Patients
The recommended pediatric dosage regimens of EMEND, to be administered with a 5-HT3 antagonist, with or without a corticosteroid, for the prevention of nausea and vomiting associated with administration of single or multi-day chemotherapy regimens of HEC or MEC, are shown in Tables 3 and 4. Single-day chemotherapy regimens include regimens in which HEC or MEC is administered for a single day only. Multi-day chemotherapy regimens include chemotherapy regimens in which HEC or MEC is administered for 2 or more days.
Structured Label Content
Section 42229-5 (42229-5)
Limitations of Use
- EMEND has not been studied for the treatment of established nausea and vomiting.
Section 42230-3 (42230-3)
| This Patient Information has been approved by the U.S. Food and Drug Administration. | Revised: May 2022 |
|
Patient Information |
|
|
Read this Patient Information before you start receiving EMEND for injection and each time you are scheduled to receive EMEND for injection. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or treatment. |
|
|
What is EMEND for injection? EMEND for injection is a prescription medicine used with other medicines that treat nausea and vomiting in patients 6 months of age and older to prevent nausea and vomiting caused by certain anti-cancer (chemotherapy) medicines.
|
|
|
Who should not receive EMEND for injection? Do not receive EMEND for injection if you:
|
|
|
What should I tell my healthcare provider before receiving EMEND for injection? Before receiving EMEND for injection, tell your healthcare provider if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. EMEND for injection may affect the way other medicines work, and other medicines may affect the way EMEND for injection works, causing serious side effects. Know the medicines you take. Keep a list of them to show your healthcare provider or pharmacist when you get a new medicine. |
|
|
How will I receive EMEND for injection? Adults 18 years of age and older: EMEND for injection will be given on Day 1 of chemotherapy treatment. It will be given to you by intravenous (IV) infusion in your vein about 50 to 60 minutes before you start your chemotherapy treatment. Children 6 months to 17 years of age: EMEND for injection will be given to your child by intravenous (IV) infusion into a large vein through a type of IV line called a central venous catheter, about 1 hour to 1 ½ hours before the start of their chemotherapy treatment. Depending on the chemotherapy treatment, there are 2 ways that EMEND for injection may be given:
If you take the blood thinner medicine warfarin sodium (COUMADIN®, JANTOVEN®), your healthcare provider may do blood tests after you receive EMEND for injection to check your blood clotting. |
|
|
What are the possible side effects of EMEND for injection? EMEND for injection may cause serious side effects, including:
In adults, the most common side effects of EMEND for injection include: |
|
|
|
|
In children 6 months to 17 years of age, the most common side effects of EMEND for injection include: |
|
|
|
|
Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all of the possible side effects of EMEND for injection. For more information ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
General information about the safe and effective use of EMEND for injection. If you would like more information about EMEND for injection, talk with your healthcare provider. You can ask your healthcare provider or pharmacist for information about EMEND for injection that is written for health professionals. For more information about EMEND for injection call 1-800-622-4477 or go to www.emend.com. |
|
|
What are the ingredients in EMEND for injection? Active ingredient: fosaprepitant Inactive ingredients: edetate disodium, polysorbate 80, lactose anhydrous, sodium hydroxide and/or hydrochloric acid (for pH adjustment) Manufactured for: Merck Sharp & Dohme LLC, Rahway, NJ 07065, USA |
Section 44425-7 (44425-7)
Storage
Emend for injection vials must be refrigerated, store at 2°C-8°C (36°F-46°F).
The reconstituted final drug solution is stable for 24 hours at ambient room temperature [at or below 25°C (77°F)]. Discard unused portion.
10 Overdosage (10 OVERDOSAGE)
There is no specific information on the treatment of overdosage with fosaprepitant or aprepitant.
In the event of overdose, EMEND should be discontinued and general supportive treatment and monitoring should be provided. Because of the antiemetic activity of EMEND, drug-induced emesis may not be effective in cases of EMEND overdosage.
Aprepitant is not removed by hemodialysis.
11 Description (11 DESCRIPTION)
EMEND (fosaprepitant) for injection is a sterile, lyophilized formulation containing fosaprepitant dimeglumine, a prodrug of aprepitant, a substance P/neurokinin-1 (NK1) receptor antagonist, an antiemetic agent, chemically described as 1-Deoxy-1-(methylamino)-D-glucitol[3-[[(2R,3S)-2-[(1R)-1-[3,5-bis(trifluoromethyl)phenyl]ethoxy]-3-(4-fluorophenyl)-4-morpholinyl]methyl]-2,5-dihydro-5-oxo-1H-1,2,4-triazol-1-yl]phosphonate (2:1) (salt).
Its empirical formula is C23H22F7N4O6P ∙ 2(C7H17NO5) and its structural formula is:
Fosaprepitant dimeglumine is a white to off-white amorphous powder with a molecular weight of 1004.83. It is freely soluble in water.
Each vial of EMEND for injection for administration as an intravenous infusion contains 150 mg of fosaprepitant (equivalent to 245.3 mg of fosaprepitant dimeglumine) and the following inactive ingredients: edetate disodium (5.4 mg), polysorbate 80 (75 mg), lactose anhydrous (375 mg), sodium hydroxide and/or hydrochloric acid (for pH adjustment).
8.4 Pediatric Use
The safety and effectiveness of a single dose and a 3-day regimen of EMEND have been established in pediatric patients 6 months to 17 years for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of HEC and MEC.
Use of EMEND in this age group is supported by evidence from adequate and well-controlled studies of EMEND for injection in adults, with additional safety, efficacy and pharmacokinetic data in pediatric patients 6 months to 17 years. Efficacy and safety were also supported by data from an adequate and well-controlled study of a 3-day oral aprepitant regimen in pediatric patients 6 months to 17 years. The safety of the 3-day EMEND for injection regimen in pediatric patients 6 months to 17 years of age was supported by an open-label study in 100 patients receiving HEC or MEC. See the full prescribing information for EMEND capsules for complete clinical information regarding studies performed with oral aprepitant. Adverse reactions were similar to those reported in adult patients [see Dosage and Administration (2.2), Adverse Reactions (6.1), Clinical Pharmacology (12.3)].
The safety and effectiveness of EMEND for the prevention of nausea and vomiting associated with HEC or MEC have not been established in patients less than 6 months of age.
8.5 Geriatric Use
Of the 1649 adult cancer patients treated with intravenous EMEND in HEC and MEC clinical studies, 27% were aged 65 and over, while 5% were aged 75 and over. Other reported clinical experience with EMEND has not identified differences in responses between elderly and younger patients. In general, use caution when dosing elderly patients as they have a greater frequency of decreased hepatic, renal or cardiac function and concomitant disease or other drug therapy [see Clinical Pharmacology (12.3)].
4 Contraindications (4 CONTRAINDICATIONS)
EMEND is contraindicated in patients:
- who are hypersensitive to any component of the product. Hypersensitivity reactions including anaphylactic reactions, flushing, erythema, and dyspnea have been reported [see Warnings and Precautions (5.2), Adverse Reactions (6.2)].
- taking pimozide. Inhibition of CYP3A4 by aprepitant, the active moiety, could result in elevated plasma concentrations of this drug, which is a CYP3A4 substrate, potentially causing serious or life-threatening reactions, such as QT prolongation, a known adverse reaction of pimozide [see Warnings and Precautions (5.1)].
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hypersensitivity Reactions [see Warnings and Precautions (5.2)]
- Infusion Site Reactions [see Warnings and Precautions (5.3)]
7 Drug Interactions (7 DRUG INTERACTIONS)
1 Indications and Usage (1 INDICATIONS AND USAGE)
EMEND® for injection, in combination with other antiemetic agents, is indicated in adults and pediatric patients 6 months of age and older for the prevention of:
- acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic cancer chemotherapy (HEC) including high-dose cisplatin.
- delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic cancer chemotherapy (MEC).
12.1 Mechanism of Action
Fosaprepitant is a prodrug of aprepitant and accordingly, its antiemetic effects are attributable to aprepitant.
Aprepitant is a selective high-affinity antagonist of human substance P/neurokinin 1 (NK1) receptors. Aprepitant has little or no affinity for serotonin (5-HT3), dopamine, and corticosteroid receptors, the targets of existing therapies for chemotherapy-induced nausea and vomiting (CINV). Aprepitant has been shown in animal models to inhibit emesis induced by cytotoxic chemotherapeutic agents, such as cisplatin, via central actions. Animal and human Positron Emission Tomography (PET) studies with aprepitant have shown that it crosses the blood brain barrier and occupies brain NK1 receptors. Animal and human studies have shown that aprepitant augments the antiemetic activity of the 5-HT3-receptor antagonist ondansetron and the corticosteroid dexamethasone and inhibits both the acute and delayed phases of cisplatin-induced emesis.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- CYP3A4 Interactions: Fosaprepitant is a weak inhibitor of CYP3A4, and aprepitant, the active moiety, is a substrate, inhibitor, and inducer of CYP3A4; see Full Prescribing Information for recommendations regarding contraindications, risk of adverse reactions, and dosage adjustment of EMEND and concomitant drugs. (4, 5.1, 7.1, 7.2)
- Hypersensitivity Reactions (including anaphylaxis and anaphylactic shock): May occur during or soon after infusion. If symptoms occur, discontinue the drug. Do not reinitiate EMEND if symptoms occur with previous use. (4, 5.2)
- Infusion Site Reactions (including thrombophlebitis, necrosis, and vasculitis): Majority of reactions reported in patients receiving vesicant chemotherapy. Avoid infusion into small veins. Discontinue infusion and administer treatment if a severe reaction develops. (5.3)
- Warfarin (a CYP2C9 substrate): Risk of decreased INR of prothrombin time; monitor INR in 2–week period, particularly at 7 to 10 days, following initiation of EMEND. (5.4, 7.1)
- Hormonal Contraceptives: Efficacy of contraceptives may be reduced during and for 28 days following administration of EMEND. Use effective alternative or back-up methods of contraception. (5.5, 7.1, 8.3)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
Recommended Adult Dosage (2.1)
- EMEND for injection 150 mg on Day 1 as an intravenous infusion over 20 to 30 minutes. (2.1)
- Complete the infusion approximately 30 minutes prior to chemotherapy.
Recommended Dosage for Pediatric Patients (6 months to 17 years) Weighing at Least 6 kg (2.2)
- See Full Prescribing Information for pediatric dosage regimens by age.
- For single dose chemotherapy regimens: single dose of EMEND for injection on Day 1.
- For single- or multi-day chemotherapy regimens: 3-day EMEND regimen of EMEND for injection on Days 1, 2, and 3. EMEND capsules or EMEND for oral suspension may be used as an alternative on Days 2 and 3.
- Administer EMEND for injection through a central venous catheter as an intravenous infusion over 30 minutes (12 years to 17 years) or 60 minutes (6 months to less than 12 years).
- Complete the infusion approximately 30 minutes prior to chemotherapy.
Concomitant Antiemetics
5.3 Infusion Site Reactions
Infusion site reactions (ISRs) have been reported with the use of EMEND for injection [see Adverse Reactions (6.1)]. The majority of severe ISRs, including thrombophlebitis and vasculitis, were reported with concomitant vesicant (anthracycline-based) chemotherapy administration, particularly when associated with extravasation. Necrosis was also reported in some patients with concomitant vesicant chemotherapy. Most ISRs occurred with the first, second or third exposure to single doses of EMEND for injection and in some cases, reactions persisted for two weeks or longer. Treatment of severe ISRs consisted of medical, and in some cases surgical, intervention.
Avoid infusion of EMEND for injection into small veins or through a butterfly catheter. If a severe ISR develops during infusion, discontinue the infusion and administer appropriate medical treatment.
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
EMEND for injection: 150 mg fosaprepitant, white to off-white lyophilized powder in single-dose glass vial for reconstitution
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of EMEND. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and subcutaneous tissue disorders: pruritus, rash, urticaria, Stevens-Johnson syndrome/toxic epidermal necrolysis [see Warnings and Precautions (5.2)].
Immune system disorders: hypersensitivity reactions including anaphylaxis and anaphylactic shock [see Contraindications (4), Warnings and Precautions (5.2)].
Nervous system disorders: ifosfamide-induced neurotoxicity reported after EMEND and ifosfamide coadministration.
5.2 Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis and anaphylactic shock, during or soon after infusion of fosaprepitant have occurred. Symptoms including flushing, erythema, dyspnea, hypotension and syncope have been reported [see Adverse Reactions (6.2)].
Monitor patients during and after infusion. If hypersensitivity reactions occur, discontinue the infusion and administer appropriate medical therapy. Do not reinitiate EMEND in patients who experience these symptoms with previous use [see Contraindications (4)].
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The overall safety of EMEND for injection was evaluated in approximately 1800 adult and pediatric patients.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise the patient to read the FDA-approved patient labeling (Patient Information).
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
Single-dose glass vial containing 150 mg of fosaprepitant as a white to off-white lyophilized powder for reconstitution. Supplied as follows:
| NDC 0006-3061-00 | 1 vial per carton. |
8.6 Patients With Hepatic Impairment (8.6 Patients with Hepatic Impairment)
The pharmacokinetics of aprepitant in patients with mild and moderate hepatic impairment were similar to those of healthy subjects with normal hepatic function. No dosage adjustment is necessary for patients with mild to moderate hepatic impairment (Child-Pugh score 5 to 9). There are no clinical or pharmacokinetic data in patients with severe hepatic impairment (Child-Pugh score greater than 9). Therefore, additional monitoring for adverse reactions in these patients may be warranted when EMEND is administered [see Clinical Pharmacology (12.3)].
2.3 Preparation of Emend for Injection (2.3 Preparation of EMEND for injection)
| The recommended dose of EMEND for injection is based on the patient's age and weight. | |
| Step 1 | Aseptically inject 5 mL 0.9% Sodium Chloride Injection, USP into the vial. Assure that 0.9% Sodium Chloride Injection, USP is added to the vial along the vial wall in order to prevent foaming. Swirl the vial gently. Avoid shaking and jetting 0.9% Sodium Chloride Injection, USP into the vial. |
| Step 2 | Aseptically prepare an infusion bag filled with 145 mL of 0.9% Sodium Chloride Injection, USP. |
| Step 3 | Aseptically withdraw the entire volume from the vial and transfer it into the infusion bag containing 145 mL of 0.9% Sodium Chloride Injection, USP to yield a total volume of 150 mL and a final concentration of 1 mg/mL. |
| Step 4 | Gently invert the bag 2 to 3 times. |
| Step 5 | Determine the volume to be administered from this prepared infusion bag, based on the recommended dose [see Dosage and Administration (2.1, 2.2)]. Adults The entire volume of the prepared infusion bag (150 mL) should be administered. Pediatrics In patients 12 years and older, the volume to be administered is calculated as follows:
|
| Step 6 | If necessary, for volumes less than 150 mL, the calculated volume can be transferred to an appropriate size bag or syringe prior to administration by infusion. |
| Step 7 | Before administration, inspect the bag for particulate matter and discoloration. Discard the bag if particulate and/or discoloration are observed. |
Caution: Do not mix or reconstitute EMEND for injection with solutions for which physical and chemical compatibility have not been established. EMEND for injection is incompatible with any solutions containing divalent cations (e.g., Ca2+, Mg2+), including Lactated Ringer's Solution and Hartmann's Solution.
Principal Display Panel 150 Mg Vial Carton (PRINCIPAL DISPLAY PANEL - 150 mg Vial Carton)
NDC 0006-3061-00
Emend®
(fosaprepitant)
for Injection
150 mg per vial
Reconstitute with 5 mL of 0.9% Sodium
Chloride for Injection.
STERILE LYOPHILIZED POWDER
FOR INTRAVENOUS USE ONLY AFTER
RECONSTITUTION AND DILUTION
DO NOT USE WITH SOLUTIONS
CONTAINING DIVALENT CATIONS
(e.g., Ca2+, Mg2+) INCLUDING
LACTATED RINGER'S SOLUTION
AND HARTMANN'S SOLUTION.
Rx only
Single-Dose Vial –
Discard Unused Portion
5.4 Decrease in Inr With Concomitant Warfarin (5.4 Decrease in INR with Concomitant Warfarin)
Coadministration of EMEND with warfarin, a CYP2C9 substrate, may result in a clinically significant decrease in the International Normalized Ratio (INR) of prothrombin time [see Clinical Pharmacology (12.3)]. Monitor the INR in patients on chronic warfarin therapy in the 2-week period, particularly at 7 to 10 days, following initiation of EMEND with each chemotherapy cycle [see Drug Interactions (7.1)].
5.1 Clinically Significant Cyp3a4 Drug Interactions (5.1 Clinically Significant CYP3A4 Drug Interactions)
Fosaprepitant, a prodrug of aprepitant, is a weak inhibitor of CYP3A4, and aprepitant is a substrate, inhibitor, and inducer of CYP3A4.
- Use of EMEND with other drugs that are CYP3A4 substrates, may result in increased plasma concentration of the concomitant drug.
- Use of pimozide with EMEND is contraindicated due to the risk of significantly increased plasma concentrations of pimozide, potentially resulting in prolongation of the QT interval, a known adverse reaction of pimozide [see Contraindications (4)].
- Use of EMEND with strong or moderate CYP3A4 inhibitors (e.g., ketoconazole, diltiazem) may increase plasma concentrations of aprepitant and result in an increased risk of adverse reactions related to EMEND.
- Use of EMEND with strong CYP3A4 inducers (e.g., rifampin) may result in a reduction in aprepitant plasma concentrations and decreased efficacy of EMEND.
See Table 7 and Table 8 for a listing of potentially significant drug interactions [see Drug Interactions (7.1, 7.2)].
5.5 Risk of Reduced Efficacy of Hormonal Contraceptives
Upon coadministration with EMEND, the efficacy of hormonal contraceptives may be reduced during administration of and for 28 days following the last dose of EMEND [see Clinical Pharmacology (12.3)]. Advise patients to use effective alternative or back-up methods of contraception during treatment with EMEND and for 1 month following administration of EMEND [see Drug Interactions (7.1), Use in Specific Populations (8.3)].
14.1 Prevention of Nausea and Vomiting Associated With Hec in Adults (14.1 Prevention of Nausea and Vomiting Associated with HEC in Adults)
In a randomized, parallel, double-blind, active-controlled study, EMEND for injection 150 mg as a single intravenous infusion (N=1147) was compared to a 3-day oral EMEND regimen (N=1175) in patients receiving a HEC regimen that included cisplatin (≥70 mg/m2). All patients in both groups received dexamethasone and ondansetron (see Table 12). Patient demographics were similar between the two treatment groups. Of the total 2322 patients, 63% were men, 56% White, 26% Asian, 3% American Indian/Alaska Native, 2% Black, 13% Multi-Racial, and 33% Hispanic/Latino ethnicity. Patient ages ranged from 19 to 86 years of age, with a mean age of 56 years. Other concomitant chemotherapy agents commonly administered were fluorouracil (17%), gemcitabine (16%), paclitaxel (15%), and etoposide (12%).
| Day 1 | Day 2 | Day 3 | Day 4 | |
|---|---|---|---|---|
| EMEND Regimen | ||||
| EMEND for injection | 150 mg intravenously over 20 to 30 minutes approximately 30 minutes prior to chemotherapy | none | none | none |
| Oral dexamethasone Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1 and in the morning on Days 2 through 4. Dexamethasone was also administered in the evenings on Days 3 and 4. The 12 mg dose of dexamethasone on Day 1 and the 8 mg once daily dose on Day 2 reflects a dosage adjustment to account for a drug interaction with the EMEND for injection regimen [see Clinical Pharmacology (12.3)].
|
12 mg | 8 mg | 8 mg twice daily | 8 mg twice daily |
| Ondansetron | Ondansetron Ondansetron 32 mg intravenous was used in the clinical trials of EMEND. Although this dose was used in clinical trials, this is no longer the currently recommended dose. Refer to the ondansetron prescribing information for the current recommended dose.
|
none | none | none |
| Oral EMEND Regimen | ||||
| EMEND capsules | 125 mg | 80 mg | 80 mg | none |
| Oral dexamethasone Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1 and in the morning on Days 2 through 4. The 12 mg dose of dexamethasone on Day 1 and the 8 mg once daily dose on Days 2 through 4 reflects a dosage adjustment to account for a drug interaction with the oral EMEND regimen [see Clinical Pharmacology (12.3)].
|
12 mg | 8 mg | 8 mg | 8 mg |
| Ondansetron | Ondansetron | none | none | none |
The efficacy of EMEND for injection was evaluated based on the primary and secondary endpoints listed in Table 13 and was shown to be non-inferior to that of the 3-day oral aprepitant regimen with regard to complete response in each of the evaluated phases. The pre-specified non-inferiority margin for complete response in the overall phase was 7%. The pre-specified non-inferiority margin for complete response in the delayed phase was 7.3%. The pre-specified non-inferiority margin for no vomiting in the overall phase was 8.2%.
| ENDPOINTS | EMEND for Injection Regimen (N = 1106) N: Number of patients included in the primary analysis of complete response.
% |
Oral EMEND Regimen (N = 1134) % |
Difference Difference and Confidence interval (CI) were calculated using the method proposed by Miettinen and Nurminen and adjusted for Gender.
(95% CI) |
|---|---|---|---|
| PRIMARY ENDPOINT | |||
| Complete Response Complete Response = no vomiting and no use of rescue therapy.
|
|||
| Overall Overall = 0 to 120 hours post-initiation of cisplatin chemotherapy.
|
71.9 | 72.3 | -0.4 (-4.1, 3.3) |
| SECONDARY ENDPOINTS | |||
| Complete Response | |||
| Delayed phase Delayed phase = 25 to 120 hours post-initiation of cisplatin chemotherapy.
|
74.3 | 74.2 | 0.1 (-3.5, 3.7) |
| No Vomiting | |||
| Overall | 72.9 | 74.6 | -1.7 (-5.3, 2.0) |
14.2 Prevention of Nausea and Vomiting Associated With Mec in Adults (14.2 Prevention of Nausea and Vomiting Associated with MEC in Adults)
In a randomized, parallel, double-blind, active comparator-controlled study, EMEND for injection 150 mg as a single intravenous infusion (N=502) in combination with ondansetron and dexamethasone (EMEND regimen) was compared with ondansetron and dexamethasone alone (standard therapy) (N=498) (see Table 14) in patients receiving a MEC regimen. Patient demographics were similar between the two treatment groups. Of the total 1,000 patients included in the efficacy analysis, 41% were men, 84% White, 4% Asian, 1% American Indian/Alaska Native, 2% Black, 10% Multi-Racial, and 19% Hispanic/Latino ethnicity. Patient ages ranged from 23 to 88 years of age, with a mean age of 60 years. The most commonly administered MEC chemotherapeutic agents were carboplatin (51%), oxaliplatin (24%), and cyclophosphamide (12%).
| Day 1 | Day 2 | Day 3 | |
|---|---|---|---|
| EMEND Regimen | |||
| EMEND for Injection | 150 mg intravenously over 20 to 30 minutes approximately 30 minutes prior to chemotherapy | none | none |
| Oral Dexamethasone Dexamethasone was administered 30 minutes prior to chemotherapy treatment on Day 1. The 12 mg dose reflects a dosage adjustment to account for a drug interaction with the EMEND for injection regimen [see Clinical Pharmacology (12.3)].
|
12 mg | none | none |
| Oral Ondansetron The first ondansetron dose was administered 30 to 60 minutes prior to chemotherapy treatment on Day 1 and the second dose was administered 8 hours after first ondansetron dose.
|
8 mg for 2 doses | none | none |
| Standard Therapy | |||
| Oral Dexamethasone | 20 mg | none | none |
| Oral Ondansetron | 8 mg for 2 doses | 8 mg twice daily | 8 mg twice daily |
The primary endpoint was complete response (defined as no vomiting and no rescue therapy) in the delayed phase (25 to 120 hours) of chemotherapy-induced nausea and vomiting. The results by treatment group are shown in Table 15.
| ENDPOINTS | EMEND for Injection Regimen (N = 502) N: Number of patients included in the intention to treat population.
% |
Standard Therapy Regimen (N = 498) % |
P-Value | Treatment Difference (95% CI) |
|---|---|---|---|---|
| PRIMARY ENDPOINT | ||||
| Complete Response Complete Response = no vomiting and no use of rescue therapy.
|
||||
| Delayed phase Delayed phase = 25 to 120 hours post-initiation of chemotherapy.
|
78.9 | 68.5 | <0.001 | 10.4 (5.1, 15.9) |
7.1 Effect of Fosaprepitant/aprepitant On the Pharmacokinetics of Other Drugs (7.1 Effect of Fosaprepitant/Aprepitant on the Pharmacokinetics of Other Drugs)
When administered intravenously, fosaprepitant, a prodrug of aprepitant, is converted to aprepitant within 30 minutes. Therefore, drug interactions following administration of EMEND for injection are likely to occur with drugs that interact with oral aprepitant.
Fosaprepitant, given as a single 150-mg dose, is a weak inhibitor of CYP3A4, and the weak inhibition of CYP3A4 continues for 2 days after single dose administration. Single dose fosaprepitant does not induce CYP3A4. Aprepitant is a substrate, an inhibitor, and an inducer of CYP3A4. Aprepitant is also an inducer of CYP2C9 [see Clinical Pharmacology (12.3)].
Some substrates of CYP3A4 are contraindicated with EMEND [see Contraindications (4)]. Dosage adjustment of some CYP3A4 and CYP2C9 substrates may be warranted, as shown in Table 7.
| CYP3A4 Substrates | |
| Pimozide | |
| Clinical Impact | Increased pimozide exposure |
| Intervention | EMEND is contraindicated [see Contraindications (4)]. |
| Benzodiazepines | |
| Clinical Impact | Increased exposure to midazolam or other benzodiazepines metabolized via CYP3A4 (alprazolam, triazolam) may increase the risk of adverse reactions [see Clinical Pharmacology (12.3)]. |
| Intervention | Monitor for benzodiazepine-related adverse reactions. |
| Dexamethasone | |
| Clinical Impact | Increased dexamethasone exposure [see Clinical Pharmacology (12.3)]. |
| Intervention | Reduce the dose of oral dexamethasone by approximately 50% [see Dosage and Administration (2.1)]. |
| Methylprednisolone | |
| Clinical Impact | Increased methylprednisolone exposure [see Clinical Pharmacology (12.3)]. |
| Intervention | Reduce the dose of oral methylprednisolone by approximately 50% on Days 1 and 2 for patients receiving HEC and on Day 1 for patients receiving MEC. Reduce the dose of intravenous methylprednisolone by 25% on Days 1 and 2 for patients receiving HEC and on Day 1 for patients receiving MEC. |
| Chemotherapeutic agents that are metabolized by CYP3A4 | |
| Clinical Impact | Increased exposure of the chemotherapeutic agent may increase the risk of adverse reactions [see Clinical Pharmacology (12.3)]. |
| Intervention |
Vinblastine, vincristine, or ifosfamide or other chemotherapeutic agents
|
| Hormonal Contraceptives | |
| Clinical Impact | Decreased hormonal exposure during administration of and for 28 days after administration of the last dose of EMEND [see Warnings and Precautions (5.5), Use in Specific Populations (8.3), and Clinical Pharmacology (12.3)]. |
| Intervention | Effective alternative or back-up methods of contraception (such as condoms and spermicides) should be used during treatment with EMEND and for 1 month following administration of EMEND. |
| Examples | birth control pills, skin patches, implants, and certain IUDs |
| CYP2C9 Substrates | |
| Warfarin | |
| Clinical Impact | Decreased warfarin exposure and decreased prothrombin time (INR) [see Warnings and Precautions (5.4), Clinical Pharmacology (12.3)]. |
| Intervention | In patients on chronic warfarin therapy, monitor the prothrombin time (INR) in the 2-week period, particularly at 7 to 10 days, following administration of EMEND with each chemotherapy cycle. |
| Other | |
| 5-HT3 Antagonists | |
| Clinical Impact | No change in the exposure of the 5-HT3 antagonist [see Clinical Pharmacology (12.3)]. |
| Intervention | No dosage adjustment needed |
| Examples | ondansetron, granisetron, dolasetron |
7.2 Effect of Other Drugs On the Pharmacokinetics of Fosaprepitant/aprepitant (7.2 Effect of Other Drugs on the Pharmacokinetics of Fosaprepitant/Aprepitant)
Aprepitant is a CYP3A4 substrate [see Clinical Pharmacology (12.3)]. Co-administration of EMEND with drugs that are inhibitors or inducers of CYP3A4 may result in increased or decreased plasma concentrations of aprepitant, respectively, as shown in Table 8.
| Moderate to Strong CYP3A4 Inhibitors | |
| Clinical Impact | Significantly increased exposure of aprepitant may increase the risk of adverse reactions associated with EMEND [see Adverse Reactions (6.1), Clinical Pharmacology (12.3)]. |
| Intervention | Avoid concomitant use of EMEND |
| Examples |
Moderate inhibitor:
diltiazem Strong inhibitors: ketoconazole, itraconazole, nefazodone, troleandomycin, clarithromycin, ritonavir, nelfinavir |
| Strong CYP3A4 Inducers | |
| Clinical Impact | Substantially decreased exposure of aprepitant in patients chronically taking a strong CYP3A4 inducer may decrease the efficacy of EMEND [see Clinical Pharmacology (12.3)]. |
| Intervention | Avoid concomitant use of EMEND |
| Examples | rifampin, carbamazepine, phenytoin |
2.1 Prevention of Nausea and Vomiting Associated With Hec and Mec in Adult Patients (2.1 Prevention of Nausea and Vomiting Associated with HEC and MEC in Adult Patients)
The recommended dosage of EMEND for injection, dexamethasone, and a 5-HT3 antagonist for the prevention of nausea and vomiting associated with administration of HEC or MEC in adults is shown in Table 1 or Table 2, respectively. Administer EMEND for injection as an intravenous infusion on Day 1 over 20 to 30 minutes, completing the infusion approximately 30 minutes prior to chemotherapy.
| Day 1 | Day 2 | Day 3 | Day 4 | |
|---|---|---|---|---|
| EMEND for injection | 150 mg intravenously over 20 to 30 minutes | none | none | none |
| Dexamethasone Administer dexamethasone 30 minutes prior to chemotherapy treatment on Day 1 and in the morning on Days 2 through 4. Also administer dexamethasone in the evenings on Days 3 and 4. A 50% dosage reduction of dexamethasone on Days 1 and 2 is recommended to account for a drug interaction with EMEND [see Clinical Pharmacology (12.3)].
|
12 mg orally | 8 mg orally | 8 mg orally twice daily | 8 mg orally twice daily |
| 5-HT3 antagonist | See selected 5-HT3 antagonist prescribing information for the recommended dosage | none | none | none |
| Day 1 | |
|---|---|
| EMEND for injection | 150 mg intravenously over 20 to 30 minutes |
| Dexamethasone Administer dexamethasone 30 minutes prior to chemotherapy treatment on Day 1. A 50% dosage reduction of dexamethasone is recommended to account for a drug interaction with EMEND [see Clinical Pharmacology (12.3)].
|
12 mg orally |
| 5-HT3 antagonist | See selected 5-HT3 antagonist prescribing information for the recommended dosage |
2.2 Prevention of Nausea and Vomiting Associated With Hec and Mec in Pediatric Patients (2.2 Prevention of Nausea and Vomiting Associated with HEC and MEC in Pediatric Patients)
The recommended pediatric dosage regimens of EMEND, to be administered with a 5-HT3 antagonist, with or without a corticosteroid, for the prevention of nausea and vomiting associated with administration of single or multi-day chemotherapy regimens of HEC or MEC, are shown in Tables 3 and 4. Single-day chemotherapy regimens include regimens in which HEC or MEC is administered for a single day only. Multi-day chemotherapy regimens include chemotherapy regimens in which HEC or MEC is administered for 2 or more days.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:39:52.070581 · Updated: 2026-03-14T22:51:19.879041