Raloxifene Hydrochloride Tablets, Usp
8152e68b-61a8-4897-8e03-900135b1dbd5
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Raloxifene hydrochloride tablets, USP is an estrogen agonist/antagonist indicated for: Treatment and prevention of osteoporosis in postmenopausal women. ( 1.1 ) Reduction in risk of invasive breast cancer in postmenopausal women with osteoporosis. ( 1.2 ) Reduction in risk of invasive breast cancer in postmenopausal women at high risk for invasive breast cancer. ( 1.3 ) Important Limitations: Raloxifene hydrochloride tablets, USP is not indicated for the treatment of invasive breast cancer, reduction of the risk of recurrence of breast cancer, or reduction of risk of noninvasive breast cancer.
Dosage and Administration
60 mg tablet orally once daily. ( 2.1 )
Contraindications
Active or past history of venous thromboembolism, including deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. ( 4.1 ) Pregnancy. ( 4.2 , 8.1 )
Warnings and Precautions
Venous Thromboembolism : Increased risk of deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. Discontinue use 72 hours prior to and during prolonged immobilization. ( 5.1 , 6.1 ) Death Due to Stroke : Increased risk of death due to stroke occurred in a trial in postmenopausal women with documented coronary heart disease or at increased risk for major coronary events. No increased risk of stroke was seen in this trial. Consider risk-benefit balance in women at risk for stroke. ( 5.2 , 14.5 ) Cardiovascular Disease : Raloxifene should not be used for the primary or secondary prevention of cardiovascular disease. ( 5.3 , 14.5 ) Premenopausal Women : Use is not recommended. ( 5.4 ) Hepatic Impairment : Use with caution. ( 5.5 ) Concomitant Use with Systemic Estrogens : Not recommended. ( 5.6 ) Hypertriglyceridemia : If previous treatment with estrogen resulted in hypertriglyceridemia, monitor serum triglycerides. ( 5.7 )
Adverse Reactions
Adverse reactions (>2% and more common than with placebo) include: hot flashes, leg cramps, peripheral edema, flu syndrome, arthralgia, sweating. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact ScieGen Pharmaeuticals Inc at 1-855-724-3436 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Cholestyramine : Use with raloxifene is not recommended. Reduces the absorption and enterohepatic cycling of raloxifene. ( 7.1 , 12.3 ) Warfarin : Monitor prothrombin time when starting or stopping raloxifene. ( 7.2 , 12.3 ) Highly Protein-Bound Drugs : Use with raloxifene with caution. Highly protein-bound drugs include diazepam, diazoxide, and lidocaine. Raloxifene is more than 95% bound to plasma proteins. ( 7.3 , 12.3 )
How Supplied
Raloxifene hydrochloride tablets, USP 60 mg tablets are white to off-white, oval, biconvex, film coated tablets, debossed with ‘SG’ on one side and ‘306’ on other side. They are available as follows: Bottle (count) NDC Number 30 (unit of use) NDC 50228-306-30 2000 NDC 50228-306-20
Storage and Handling
Store at controlled room temperature, 20° to 25°C (68° to 77°F) [ see USP]. The USP defines controlled room temperature as a temperature maintained thermostatically that encompasses the usual and customary working environment of 20° to 25°C (68° to 77°F); that results in a mean kinetic temperature calculated to be not more than 25°C; and that allows for excursions between 15° and 30°C (59° and 86°F) that are experienced in pharmacies, hospitals, and warehouses.
Description
Contraindications, Pregnancy ( 4.2 ) 06/2018 Warnings and Precautions, Premenopausal Use ( 5.4 ) 06/2018
Medication Information
Warnings and Precautions
Venous Thromboembolism : Increased risk of deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. Discontinue use 72 hours prior to and during prolonged immobilization. ( 5.1 , 6.1 ) Death Due to Stroke : Increased risk of death due to stroke occurred in a trial in postmenopausal women with documented coronary heart disease or at increased risk for major coronary events. No increased risk of stroke was seen in this trial. Consider risk-benefit balance in women at risk for stroke. ( 5.2 , 14.5 ) Cardiovascular Disease : Raloxifene should not be used for the primary or secondary prevention of cardiovascular disease. ( 5.3 , 14.5 ) Premenopausal Women : Use is not recommended. ( 5.4 ) Hepatic Impairment : Use with caution. ( 5.5 ) Concomitant Use with Systemic Estrogens : Not recommended. ( 5.6 ) Hypertriglyceridemia : If previous treatment with estrogen resulted in hypertriglyceridemia, monitor serum triglycerides. ( 5.7 )
Indications and Usage
Raloxifene hydrochloride tablets, USP is an estrogen agonist/antagonist indicated for: Treatment and prevention of osteoporosis in postmenopausal women. ( 1.1 ) Reduction in risk of invasive breast cancer in postmenopausal women with osteoporosis. ( 1.2 ) Reduction in risk of invasive breast cancer in postmenopausal women at high risk for invasive breast cancer. ( 1.3 ) Important Limitations: Raloxifene hydrochloride tablets, USP is not indicated for the treatment of invasive breast cancer, reduction of the risk of recurrence of breast cancer, or reduction of risk of noninvasive breast cancer.
Dosage and Administration
60 mg tablet orally once daily. ( 2.1 )
Contraindications
Active or past history of venous thromboembolism, including deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. ( 4.1 ) Pregnancy. ( 4.2 , 8.1 )
Adverse Reactions
Adverse reactions (>2% and more common than with placebo) include: hot flashes, leg cramps, peripheral edema, flu syndrome, arthralgia, sweating. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact ScieGen Pharmaeuticals Inc at 1-855-724-3436 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Cholestyramine : Use with raloxifene is not recommended. Reduces the absorption and enterohepatic cycling of raloxifene. ( 7.1 , 12.3 ) Warfarin : Monitor prothrombin time when starting or stopping raloxifene. ( 7.2 , 12.3 ) Highly Protein-Bound Drugs : Use with raloxifene with caution. Highly protein-bound drugs include diazepam, diazoxide, and lidocaine. Raloxifene is more than 95% bound to plasma proteins. ( 7.3 , 12.3 )
Storage and Handling
Store at controlled room temperature, 20° to 25°C (68° to 77°F) [ see USP]. The USP defines controlled room temperature as a temperature maintained thermostatically that encompasses the usual and customary working environment of 20° to 25°C (68° to 77°F); that results in a mean kinetic temperature calculated to be not more than 25°C; and that allows for excursions between 15° and 30°C (59° and 86°F) that are experienced in pharmacies, hospitals, and warehouses.
How Supplied
Raloxifene hydrochloride tablets, USP 60 mg tablets are white to off-white, oval, biconvex, film coated tablets, debossed with ‘SG’ on one side and ‘306’ on other side. They are available as follows: Bottle (count) NDC Number 30 (unit of use) NDC 50228-306-30 2000 NDC 50228-306-20
Description
Contraindications, Pregnancy ( 4.2 ) 06/2018 Warnings and Precautions, Premenopausal Use ( 5.4 ) 06/2018
Principal Display Panel
NDC 50228-306-30
Raloxifene Hydrochloride Tablets, USP 60mg
PHARMACIST: Dispense the accompanying Medication Guide to each patient.
30 Tablets Rx Only
NDC 50228-306-20
Raloxifene Hydrochloride Tablets, USP 60mg
PHARMACIST: Dispense the accompanying Medication Guide to each patient.
2,000 Tablets Rx Only
Section 42229-5
Osteoporosis Treatment Clinical Trial (MORE) — The safety of raloxifene in the treatment of osteoporosis was assessed in a large (7705 patients) multinational, placebo- controlled trial. Duration of treatment was 36 months, and 5129 postmenopausal women were exposed to raloxifene (2557 received 60 mg/day, and 2572 received 120 mg/day). The incidence of all-cause mortality was similar among groups: 23 (0.9%) placebo, 13 (0.5%) raloxifene-treated (raloxifene HCL 60mg), and 28 (1.1%) raloxifene HCL 120 mg women died. Therapy was discontinued due to an adverse reaction in 10.9% of raloxifene-treated women and 8.8% of placebo-treated women.
Venous Thromboembolism: The most serious adverse reaction related to raloxifene was VTE (deep venous thrombosis, pulmonary embolism, and retinal vein thrombosis). During an average of study-drug exposure of 2.6 years, VTE occurred in about 1 out of 100 patients treated with raloxifene. Twenty-six raloxifene-treated women had a VTE compared to 11 placebo-treated women, the hazard ratio was 2.4 (95% confidence interval, 1.2, 4.5), and the highest VTE risk was during the initial months of treatment.
Common adverse reactions considered to be related to raloxifene therapy were hot flashes and leg cramps. Hot flashes occurred in about one in 10 patients on raloxifene and were most commonly reported during the first 6 months of treatment and were not different from placebo thereafter. Leg cramps occurred in about one in 14 patients on raloxifene.
Section 42231-1
Medication Guide
RALOXIFENE (ral.ox.i.fene) Hydrochloride Tablets, USP 60 mg for oral use
Read the Medication Guide that comes with raloxifene hydrochloride tablets before you start taking it and each time you refill your prescription. The information may have changed. This Medication Guide does not take the place of talking with your doctor about your medical condition or treatment. Talk with your doctor about raloxifene hydrochloride tablets when you start taking it and at regular checkups.
What is the most important information I should know about raloxifene hydrochloride tablets?
Serious and life-threatening side effects can occur while taking raloxifene hydrochloride tablets. These include blood clots and dying from stroke:
- Increased risk of blood clots in the legs (deep vein thrombosis) and lungs (pulmonary embolism) have been reported with raloxifene hydrochloride tablets. Women who have or have had blood clots in the legs, lungs, or eyes should not take raloxifene hydrochloride tablets.
- Women who have had a heart attack or are at risk for a heart attack may have an increased risk of dying from stroke when taking raloxifene hydrochloride tablets.
- Before starting raloxifene hydrochloride tablets, tell your doctor if you have had blood clots in your legs, lungs, or eyes, a stroke, mini-stroke (transient ischemic attack), or have an irregular heartbeat.
- Stop taking raloxifene hydrochloride tablets and call your doctor if you have:
- leg pain or a feeling of warmth in the lower leg (calf).
- swelling of the legs, hands, or feet.
- sudden chest pain, shortness of breath, or coughing up blood.
- sudden change in your vision, such as loss of vision or blurred vision.
- Being still for a long time (such as sitting still during a long car or airplane trip or being in bed after surgery) can increase your risk of blood clots. (See “ What should I avoid if I am taking raloxifene hydrochloride tablets?” )
What is raloxifene hydrochloride?
Raloxifene hydrochloride is a type of prescription medicine called a Selective Estrogen Receptor Modulator (SERM). Raloxifene hydrochloride tablets are for women after menopause, and has more than one use:
- Osteoporosis: Raloxifene hydrochloride tablets treats and prevents osteoporosis by helping make your bones stronger and less likely to break.
- Invasive Breast Cancer: If you have osteoporosis or are at high risk for breast cancer, raloxifene hydrochloride tablets can be used to lower your chance of getting invasive breast cancer. Raloxifene hydrochloride tablets will not totally get rid of your chance of getting breast cancer. Your doctor can estimate your risk of breast cancer by asking you about risk factors, including:
- your age (getting older).
- family history of breast cancer in your mother, sister, or daughter.
- a history of any breast biopsy, especially an abnormal biopsy.
You and your doctor should talk about whether the possible benefit of raloxifene hydrochloride tablets in lowering your chance of getting invasive breast cancer is greater than its possible risks.
Raloxifene hydrochloride tablets are not for use in premenopausal women (women who have not passed menopause).
Who should not take raloxifene hydrochloride tablets?
Do not take raloxifene hydrochloride tablets if you:
- have or have had blood clots in your legs, lungs, or eyes. Taking raloxifene hydrochloride tablets may increase the risk of getting blood clots.
- are pregnant or could become pregnant. Raloxifene hydrochloride tablets could harm your unborn child.
- are nursing a baby. It is not known if raloxifene passes into breast milk or what effect it might have on the baby.
What should I tell my doctor before taking raloxifene hydrochloride tablets?
Raloxifene hydrochloride tablets may not be right for you. Before taking raloxifene hydrochloride tablets, tell your doctor about all your medical conditions, including if you:
- have had blood clots in your legs, lungs, or eyes, a stroke, mini-stroke (TIA/transient ischemic attack), or a type of irregular heartbeat (atrial fibrillation).
- have had breast cancer. Raloxifene hydrochloride tablets have not been fully studied in women who have a history of breast cancer.
- have liver or kidney problems.
- have taken estrogen in the past and had a high increase of triglycerides (a kind of fat in the blood).
- are pregnant, planning to become pregnant, or breast-feeding (see “ Who should not take raloxifene hydrochloride tablets?” ).
Tell your doctor about all medicines you take, including prescription and non-prescription medicines, vitamins, and herbal supplements. Know the medicines you take. Keep a list of them and show it to your doctor and pharmacist each time you get a new medicine. Especially tell your doctor if you take*:
- warfarin (Coumadin
®, Jantoven
®)
If you are taking warfarin or other coumarin blood thinners, your doctor may need to do a blood test when you first start or if you need to stop taking raloxifene hydrochloride tablets. Names for this test include “prothrombin time,” “pro-time,” or “INR.” Your doctor may need to adjust the dose of your warfarin or other coumarin blood thinner. - cholestyramine
- estrogens
Raloxifene hydrochloride tablets should not be taken with cholestyramine or estrogens.
How should I take raloxifene hydrochloride tablets?
- Take raloxifene hydrochloride tablets exactly how your doctor tells you to.
- Keep taking raloxifene hydrochloride tablets for as long as your doctor prescribes it for you. It is not known how long you should keep taking raloxifene hydrochloride tablets to lower your chance of getting invasive breast cancers.
- It is important to get your refills on time so you do not run out of the medicine.
- Take one raloxifene hydrochloride tablets each day.
- Take raloxifene hydrochloride tablets at any time of the day, with or without food.
- To help you remember to take raloxifene hydrochloride tablets, it may be best to take it at about the same time each day.
- Calcium and vitamin D may be taken at the same time as raloxifene hydrochloride tablets. It is important to take calcium and vitamin D, as directed by your physician, to prevent or treat osteoporosis.
- If you miss a dose, take it as soon as you remember. However, if it is almost time for your next dose, skip the missed dose and take only your next regularly scheduled dose. Do not take two doses at the same time.
What should I avoid while taking raloxifene hydrochloride tablets?
- Being still for a long time (such as during long trips or being in bed after surgery) can increase the risk of blood clots. Raloxifene hydrochloride tablets may add to this risk. If you will need to be still for a long time, talk with your doctor about ways to reduce the risk of blood clots. On long trips, move around periodically. Stop taking raloxifene hydrochloride tablets at least 3 days before a planned surgery or before you plan on being still for a long time. You should start taking raloxifene hydrochloride tablets again when you return to your normal activities.
- Some medicines should not be taken with raloxifene hydrochloride tablets (see “ What should I tell my doctor before taking raloxifene hydrochloride tablets?” ).
What are the possible side effects of raloxifene hydrochloride tablets?
Serious and life-threatening side effects can occur while taking raloxifene hydrochloride tablets. These include blood clots and dying from stroke:
- Increased risk of blood clots in the legs (deep vein thrombosis) and lungs (pulmonary embolism) have been reported with raloxifene hydrochloride tablets. Women who have or have had blood clots in the legs, lungs, or eyes should not take raloxifene hydrochloride tablets.
- Women who have had a heart attack or are at risk for a heart attack may have an increased risk of dying from stroke when taking raloxifene hydrochloride tablets .
See “ What is the most important information I should know about raloxifene hydrochloride tablets?”
The most common side effects of raloxifene hydrochloride tablets are hot flashes, leg cramps, swelling of the feet, ankles, and legs, flu syndrome, joint pain, and sweating. Hot flashes are more common during the first 6 months after starting treatment.
These are not all the side effects of raloxifene hydrochloride tablets. Tell your doctor about any side effect that bothers you or that does not go away. If you have any problems or questions that concern you while taking raloxifene hydrochloride tablets? ask your doctor or pharmacist for more information.
What else should I know about raloxifene hydrochloride tablets?
- Do not use raloxifene hydrochloride tablets to prevent heart disease, heart attack, or strokes.
- To get the calcium and vitamin D you need, your doctor may advise you to change your diet and/or take supplemental calcium and vitamin D. Your doctor may suggest other ways to help treat or prevent osteoporosis, in addition to taking raloxifene hydrochloride tablets and getting the calcium and vitamin D you need. These may include regular exercise, stopping smoking, and drinking less alcohol.
- Women who have hot flashes can take raloxifene hydrochloride. Raloxifene hydrochloride tablets do not treat hot flashes, and it may cause hot flashes in some women. (See “ What are the possible side effects of raloxifene hydrochloride?” )
- Raloxifene hydrochloride tablets have not been found to cause breast tenderness or enlargement. If you notice any changes in your breasts, call your doctor to find out the cause. Before starting and while taking raloxifene hydrochloride tablets you should have breast exams and mammograms, as directed by your doctor. Because raloxifene hydrochloride tablets does not eliminate the chance of developing breast cancers, you need these examinations to find any breast cancers as early as possible.
- Raloxifene hydrochloride tablets should not cause spotting or menstrual-type bleeding. If you have any vaginal bleeding, call your doctor to find out the cause. Raloxifene hydrochloride tablets have not been found to increase the risk for cancer of the lining of the uterus.
- Women in clinical trials have taken raloxifene hydrochloride tablets for up to eight years.
How should I store raloxifene hydrochloride tablets?
- Store raloxifene hydrochloride tablets at 68°F to 77°F (20°C to 25°C).
- Keep raloxifene hydrochloride tablets and all medicines out of the reach of children.
General Information about the safe and effective use of raloxifene hydrochloride tablets
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use raloxifene hydrochloride tablets for a condition for which it was not prescribed. Do not give your raloxifene hydrochloride tablets to other people, even if they have the same symptoms you have. It may harm them.
This Medication Guide is a summary of the most important information about raloxifene hydrochloride tablets. If you would like more information about raloxifene hydrochloride tablets, talk with your doctor. You can ask your doctor or pharmacist for information about raloxifene hydrochloride tablets that is written for health professionals. For more information, call 1-855-724-3436 (toll-free).
What are the ingredients in raloxifene hydrochloride tablets, USP?
Active Ingredient: raloxifene hydrochloride USP
Inactive Ingredients: citric acid monohydrate, crospovidone, hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate 80, povidone and titanium dioxide.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
*The brands listed are trademarks of their respective owners and are not trademarks of ScieGen Pharmaceuticals Inc. The makers of these brands are not affiliated with and do not endorse ScieGen Pharmaceuticals Inc and company or its products.
Manufactured by:
ScieGen Pharmaceuticals, Inc.
Huappauge, NY 11788, USA
Revision: 6/18
Section 43683-2
7.2 Warfarin
If raloxifene is given concomitantly with warfarin or other warfarin derivatives, prothrombin time should be monitored more closely when starting or stopping therapy with raloxifene [see Clinical Pharmacology ( 12.3)] .
10 Overdosage
In an 8-week study of 63 postmenopausal women, a dose of raloxifene hydrochloride (HCL) 600 mg/day was safely tolerated. In clinical trials, no raloxifene overdose has been reported.
In postmarketing spontaneous reports, raloxifene overdose has been reported very rarely (less than 1 out of 10,000 [<0.01%] patients treated). The highest overdose has been approximately 1.5 grams. No fatalities associated with raloxifene overdose have been reported. Adverse reactions were reported in approximately half of the adults who took ≥180 mg raloxifene HCL and included leg cramps and dizziness.
Two 18-month-old children each ingested raloxifene HCL 180 mg. In these two children, symptoms reported included ataxia, dizziness, vomiting, rash, diarrhea, tremor, and flushing, as well as elevation in alkaline phosphatase.
There is no specific antidote for raloxifene.
No mortality was seen after a single oral dose in rats or mice at 5000 mg/kg (810 times the human dose for rats and 405 times the human dose for mice based on surface area, mg/m 2) or in monkeys at 1000 mg/kg (80 times the AUC in humans).
4.2 Pregnancy
Raloxifene hydrochloride tablets, USP is contraindicated for use in pregnancy, as it may cause fetal harm [see Use in Specific Populations ( 8.1)] .
11 Description
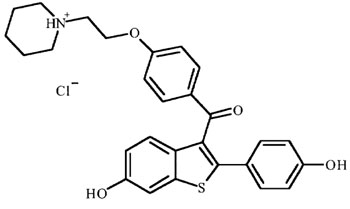
Raloxifene Hydrochloride is an estrogen agonist/antagonist, commonly referred to as a selective estrogen receptor modulator (SERM) that belongs to the benzothiophene class of compounds. The chemical structure is:
The chemical designation is methanone, [6-hydroxy-2-(4-hydroxyphenyl)benzo[ b ]thien-3-yl]-[4-[2-(1-piperidinyl)ethoxy]phenyl]-, hydrochloride. Raloxifene hydrochloride (HCl) has the empirical formula C 28H 27NO 4S•HCl, which corresponds to a molecular weight of 510.04. Raloxifene Hydrochloride USP is an Almost white to pale yellow powder that freely soluble in dimethyl sulfoxide, practically insoluble in ether and in ethyl acetate.
Raloxifene hydrochloride tablets USP, 60 mg is supplied in a tablet dosage form for oral administration. Each raloxifene hydrochloride tablets USP, 60 mg contains 60 mg of raloxifene HCl, which is the molar equivalent of 55.71 mg of free base. Inactive ingredients include citric acid monohydrate, crospovidone, hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate 80, povidone and titanium dioxide.
USP Dissolution Test is pending.
5.10 Use in Men
There is no indication for the use of raloxifene in men. Raloxifene has not been adequately studied in men and its use is not recommended.
16.1 How Supplied
Raloxifene hydrochloride tablets, USP 60 mg tablets are white to off-white, oval, biconvex, film coated tablets, debossed with ‘SG’ on one side and ‘306’ on other side. They are available as follows:
Bottle (count)
NDC Number
30 (unit of use) NDC 50228-306-30
2000
NDC 50228-306-20
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
Of the total number of patients in placebo-controlled clinical studies of raloxifene, 61% were 65 and over, while 15.5% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. Based on clinical trials, there is no need for dose adjustment for geriatric patients [see Clinical Pharmacology ( 12.3)] .
7.1 Cholestyramine
Concomitant administration of cholestyramine with raloxifene is not recommended. Although not specifically studied, it is anticipated that other anion exchange resins would have a similar effect. Raloxifene should not be co-administered with other anion exchange resins [see Clinical Pharmacology ( 12.3)] .
4 Contraindications
6 Adverse Reactions
Adverse reactions (>2% and more common than with placebo) include: hot flashes, leg cramps, peripheral edema, flu syndrome, arthralgia, sweating. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ScieGen Pharmaeuticals Inc at 1-855-724-3436 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions
- Cholestyramine: Use with raloxifene is not recommended. Reduces the absorption and enterohepatic cycling of raloxifene. ( 7.1, 12.3)
- Warfarin: Monitor prothrombin time when starting or stopping raloxifene. ( 7.2, 12.3)
- Highly Protein-Bound Drugs: Use with raloxifene with caution. Highly protein-bound drugs include diazepam, diazoxide, and lidocaine. Raloxifene is more than 95% bound to plasma proteins. ( 7.3, 12.3)
5.8 Renal Impairment
Raloxifene should be used with caution in patients with moderate or severe renal impairment. Safety and efficacy have not been established in patients with moderate or severe renal impairment [see Clinical Pharmacology ( 12.3)] .
8.6 Renal Impairment
12.2 Pharmacodynamics
Decreases in estrogen levels after oophorectomy or menopause lead to increases in bone resorption and accelerated bone loss. Bone is initially lost rapidly because the compensatory increase in bone formation is inadequate to offset resorptive losses. In addition to loss of estrogen, this imbalance between resorption and formation may be due to age-related impairment of osteoblasts or their precursors. In some women, these changes will eventually lead to decreased bone mass, osteoporosis, and increased risk for fractures, particularly of the spine, hip, and wrist. Vertebral fractures are the most common type of osteoporotic fracture in postmenopausal women.
In both the osteoporosis treatment and prevention trials, raloxifene resulted in consistent, statistically significant suppression of bone resorption and bone formation, as reflected by changes in serum and urine markers of bone turnover (e.g., bone-specific alkaline phosphatase, osteocalcin, and collagen breakdown products). The suppression of bone turnover markers was evident by 3 months and persisted throughout the 36-month and 24-month observation periods.
In a 31-week, open-label, radiocalcium kinetics study, 33 early postmenopausal women were randomized to treatment with once-daily raloxifene hydrochloride 60 mg, cyclic estrogen/progestin (0.625 mg conjugated estrogens daily with 5 mg medroxyprogesterone acetate daily for the first 2 weeks of each month [hormone therapy]), or no treatment. Treatment with either raloxifene or hormone therapy was associated with reduced bone resorption and a positive shift in calcium balance (-82 mg Ca/day and +60 mg Ca/day, respectively, for raloxifene and -162 mg Ca/day and +91 mg Ca/day, respectively, for hormone therapy). There were small decreases in serum total calcium, inorganic phosphate, total protein, and albumin, which were generally of lesser magnitude than decreases observed during estrogen or hormone therapy. Platelet count was also decreased slightly and was not different from estrogen therapy.
12.3 Pharmacokinetics
The disposition of raloxifene has been evaluated in more than 3000 postmenopausal women in selected raloxifene osteoporosis treatment and prevention clinical trials, using a population approach. Pharmacokinetic data also were obtained in conventional pharmacology studies in 292 postmenopausal women. Raloxifene exhibits high within-subject variability (approximately 30% coefficient of variation) of most pharmacokinetic parameters. Table 3 summarizes the pharmacokinetic parameters of raloxifene.
Absorption — Raloxifene is absorbed rapidly after oral administration. Approximately 60% of an oral dose is absorbed, but presystemic glucuronide conjugation is extensive. Absolute bioavailability of raloxifene is 2%. The time to reach average maximum plasma concentration and bioavailability are functions of systemic interconversion and enterohepatic cycling of raloxifene and its glucuronide metabolites. Administration of raloxifene HCl with a standardized, high-fat meal increases the absorption of raloxifene (C max 28% and AUC 16%), but does not lead to clinically meaningful changes in systemic exposure. Raloxifene can be administered without regard to meals.
Distribution — Following oral administration of single doses ranging from 30 to 150 mg of raloxifene HCl, the apparent volume of distribution is 2348 L/kg and is not dose dependent. Raloxifene and the monoglucuronide conjugates are highly (95%) bound to plasma proteins. Raloxifene binds to both albumin and α1-acid glycoprotein, but not to sex-steroid binding globulin.
Metabolism — Biotransformation and disposition of raloxifene in humans have been determined following oral administration of 14C-labeled raloxifene. Raloxifene undergoes extensive first-pass metabolism to the glucuronide conjugates: raloxifene-4′-glucuronide, raloxifene-6-glucuronide, and raloxifene-6,4′-diglucuronide. No other metabolites have been detected, providing strong evidence that raloxifene is not metabolized by cytochrome P450 pathways. Unconjugated raloxifene comprises less than 1% of the total radiolabeled material in plasma. The terminal log-linear portions of the plasma concentration curves for raloxifene and the glucuronides are generally parallel. This is consistent with interconversion of raloxifene and the glucuronide metabolites. Following intravenous administration, raloxifene is cleared at a rate approximating hepatic blood flow. Apparent oral clearance is 44.1 L/kg•hr. Raloxifene and its glucuronide conjugates are interconverted by reversible systemic metabolism and enterohepatic cycling, thereby prolonging its plasma elimination half-life to 27.7 hours after oral dosing. Results from single oral doses of raloxifene predict multiple-dose pharmacokinetics. Following chronic dosing, clearance ranges from 40 to 60 L/kg•hr. Increasing doses of raloxifene HCl (ranging from 30 to 150 mg) result in slightly less than a proportional increase in the area under the plasma time concentration curve (AUC).
Excretion — Raloxifene is primarily excreted in feces, and less than 0.2% is excreted unchanged in urine. Less than 6% of the raloxifene dose is eliminated in urine as glucuronide conjugates.
|
a Abbreviations: C max = maximum plasma concentration, t 1/2 = half-life, AUC = area under the curve, CL = clearance, V = volume of distribution, F = bioavailability, CV = coefficient of variation. |
|||||
|
b Data normalized for dose in mg and body weight in kg. |
|||||
|
c Range of observed half-life. |
|||||
|
C
max
a, b
(ng/mL)/ (mg/kg) |
t 1/2 (hr) a |
AUC
0-
∞
a, b
(ng•hr/mL)/ (mg/kg) |
CL/F
a
(L/kg•hr) |
V/F
a
(L/kg) |
|
|
Single Dose
Mean |
0.50 | 27.7 | 27.2 | 44.1 | 2348 |
| CV a (%) | 52 | 10.7 to 273 c | 44 | 46 | 52 |
|
Multiple Dose
Mean |
1.36 | 32.5 | 24.2 | 47.4 | 2853 |
| CV a (%) | 37 | 15.8 to 86.6 c | 36 | 41 | 56 |
Special Populations
Pediatric — The pharmacokinetics of raloxifene has not been evaluated in a pediatric population [see Use in Specific Populations ( 8.4)] .
Geriatric — No differences in raloxifene pharmacokinetics were detected with regard to age (range 42 to 84 years) [see Use in Specific Populations ( 8.5)] .
Gender — Total extent of exposure and oral clearance, normalized for lean body weight, are not significantly different between age-matched female and male volunteers.
Race — Pharmacokinetic differences due to race have been studied in 1712 women, including 97.5% White, 1.0% Asian, 0.7% Hispanic, and 0.5% Black in the osteoporosis treatment trial and in 1053 women, including 93.5% White, 4.3% Hispanic, 1.2% Asian, and 0.5% Black in the osteoporosis prevention trials. There were no discernible differences in raloxifene plasma concentrations among these groups; however, the influence of race cannot be conclusively determined.
5.4 Premenopausal Use
There is no indication for premenopausal use of raloxifene. Safety of raloxifene in premenopausal women has not been established and its use is not recommended.
Additionally, there is concern regarding inadvertent drug exposure in pregnancy in women of reproductive potential who become pregnant, due to risk of fetal harm [see Use in Specific Populations ( 8.1)] .
2.1 Recommended Dosing
The recommended dosage is one raloxifene hydrochloride tablets, USP 60 mg daily, which may be administered any time of day without regard to meals [see Clinical Pharmacology ( 12.3)] .
For the indications in risk of invasive breast cancer the optimum duration of treatment is not known [see Clinical Studies ( 14.3, 14.4)] .
5.5 Hepatic Impairment
Raloxifene should be used with caution in patients with hepatic impairment. Safety and efficacy have not been established in patients with hepatic impairment [see Clinical Pharmacology ( 12.3)] .
7.4 Systemic Estrogens
The safety of concomitant use of raloxifene with systemic estrogens has not been established and its use is not recommended.
8.7 Hepatic Impairment
1 Indications and Usage
Raloxifene hydrochloride tablets, USP is an estrogen agonist/antagonist indicated for:
- Treatment and prevention of osteoporosis in postmenopausal women. ( 1.1)
- Reduction in risk of invasive breast cancer in postmenopausal women with osteoporosis. ( 1.2)
- Reduction in risk of invasive breast cancer in postmenopausal women at high risk for invasive breast cancer. ( 1.3)
Important Limitations: Raloxifene hydrochloride tablets, USP is not indicated for the treatment of invasive breast cancer, reduction of the risk of recurrence of breast cancer, or reduction of risk of noninvasive breast cancer.
5.2 Death Due to Stroke
In a clinical trial of postmenopausal women with documented coronary heart disease or at increased risk for coronary events, an increased risk of death due to stroke was observed after treatment with raloxifene. During an average follow-up of 5.6 years, 59 (1.2%) raloxifene-treated women died due to a stroke compared to 39 (0.8%) placebo-treated women (22 versus 15 per 10,000 women-years; hazard ratio 1.49; 95% confidence interval, 1.00 to 2.24; p=0.0499). There was no statistically significant difference between treatment groups in the incidence of stroke (249 in raloxifene [4.9%] versus 224 placebo [4.4%]). Raloxifene had no significant effect on all-cause mortality. The risk-benefit balance should be considered in women at risk for stroke, such as prior stroke or transient ischemic attack (TIA), atrial fibrillation, hypertension, or cigarette smoking [see Clinical Studies ( 14.5)] .
12.1 Mechanism of Action
Raloxifene is an estrogen agonist/antagonist, commonly referred to as a selective estrogen receptor modulator (SERM). The biological actions of raloxifene are largely mediated through binding to estrogen receptors. This binding results in activation of estrogenic pathways in some tissues (agonism) and blockade of estrogenic pathways in others (antagonism). The agonistic or antagonistic action of raloxifene depends on the extent of recruitment of coactivators and corepressors to estrogen receptor (ER) target gene promoters.
Raloxifene appears to act as an estrogen agonist in bone. It decreases bone resorption and bone turnover, increases bone mineral density (BMD) and decreases fracture incidence. Preclinical data demonstrate that raloxifene is an estrogen antagonist in uterine and breast tissues. These results are consistent with findings in clinical trials, which suggest that raloxifene lacks estrogen-like effects on the uterus and breast tissue.
16.2 Storage and Handling
Store at controlled room temperature, 20° to 25°C (68° to 77°F) [ see USP]. The USP defines controlled room temperature as a temperature maintained thermostatically that encompasses the usual and customary working environment of 20° to 25°C (68° to 77°F); that results in a mean kinetic temperature calculated to be not more than 25°C; and that allows for excursions between 15° and 30°C (59° and 86°F) that are experienced in pharmacies, hospitals, and warehouses.
5.12 Breast Abnormalities
Any unexplained breast abnormality occurring during raloxifene therapy should be investigated. Raloxifene does not eliminate the risk of breast cancer [see Clinical Studies ( 14.4)] .
4.1 Venous Thromboembolism
Raloxifene is contraindicated in women with active or past history of venous thromboembolism (VTE), including deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis [see Warnings and Precautions ( 5.1)] .
5 Warnings and Precautions
- Venous Thromboembolism: Increased risk of deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. Discontinue use 72 hours prior to and during prolonged immobilization. ( 5.1, 6.1)
- Death Due to Stroke: Increased risk of death due to stroke occurred in a trial in postmenopausal women with documented coronary heart disease or at increased risk for major coronary events. No increased risk of stroke was seen in this trial. Consider risk-benefit balance in women at risk for stroke. ( 5.2, 14.5)
- Cardiovascular Disease: Raloxifene should not be used for the primary or secondary prevention of cardiovascular disease. ( 5.3, 14.5)
- Premenopausal Women: Use is not recommended. ( 5.4)
- Hepatic Impairment: Use with caution. ( 5.5)
- Concomitant Use with Systemic Estrogens: Not recommended. ( 5.6)
- Hypertriglyceridemia: If previous treatment with estrogen resulted in hypertriglyceridemia, monitor serum triglycerides. ( 5.7)
5.1 Venous Thromboembolism
In clinical trials, raloxifene-treated women had an increased risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism). Other venous thromboembolic events also could occur. A less serious event, superficial thrombophlebitis, also has been reported more frequently with raloxifene than with placebo. The greatest risk for deep vein thrombosis and pulmonary embolism occurs during the first 4 months of treatment, and the magnitude of risk appears to be similar to the reported risk associated with use of hormone therapy. Because immobilization increases the risk for venous thromboembolic events independent of therapy, raloxifene should be discontinued at least 72 hours prior to and during prolonged immobilization (e.g., post-surgical recovery, prolonged bed rest), and raloxifene therapy should be resumed only after the patient is fully ambulatory. In addition, women taking raloxifene should be advised to move about periodically during prolonged travel. The risk-benefit balance should be considered in women at risk of thromboembolic disease for other reasons, such as congestive heart failure, superficial thrombophlebitis, and active malignancy [see Contraindications ( 4.1) and Adverse Reactions ( 6.1)] .
5.3 Cardiovascular Disease
Raloxifene should not be used for the primary or secondary prevention of cardiovascular disease. In a clinical trial of postmenopausal women with documented coronary heart disease or at increased risk for coronary events, no cardiovascular benefit was demonstrated after treatment with raloxifene for 5 years [see Clinical Studies ( 14.5)] .
17.2 Patient Immobilization
Raloxifene hydrochloride tablets should be discontinued at least 72 hours prior to and during prolonged immobilization (e.g., post-surgical recovery, prolonged bed rest), and patients should be advised to avoid prolonged restrictions of movement during travel because of the increased risk of venous thromboembolic events [see Warnings and Precautions ( 5.1)] .
17.3 Hot Flashes Or Flushes
Raloxifene hydrochloride tablets may increase the incidence of hot flashes and is not effective in reducing hot flashes or flushes associated with estrogen deficiency. In some asymptomatic patients, hot flashes may occur upon beginning raloxifene hydrochloride tablets therapy.
2 Dosage and Administration
60 mg tablet orally once daily. ( 2.1)
3 Dosage Forms and Strengths
60 mg, white to off-white, oval, biconvex, film coated tablets (not scored). They are debossed with ‘SG’ on one side and ‘306’ on other side.
5.9 History of Breast Cancer
Raloxifene has not been adequately studied in women with a prior history of breast cancer.
6.2 Postmarketing Experience
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Adverse reactions reported very rarely since market introduction include retinal vein occlusion, stroke, and death associated with venous thromboembolism (VTE).
8 Use in Specific Populations
- Pediatric Use: Safety and effectiveness not established. ( 8.4)
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described below reflect exposure to raloxifene in 8429 patients who were enrolled in placebo-controlled trials, including 6666 exposed for 1 year and 5685 for at least 3 years.
5.6 Concomitant Estrogen Therapy
The safety of concomitant use of raloxifene with systemic estrogens has not been established and its use is not recommended.
17 Patient Counseling Information
See FDA-approved Medication Guide.
Physicians should instruct their patients to read the Medication Guide before starting therapy with Raloxifene hydrochloride tablets, and to reread it each time the prescription is renewed.
5.11 Unexplained Uterine Bleeding
7.5 Other Concomitant Medications
Raloxifene can be concomitantly administered with ampicillin, amoxicillin, antacids, corticosteroids, and digoxin [see Clinical Pharmacology ( 12.3)] .
The concomitant use of raloxifene and lipid-lowering agents has not been studied.
7.3 Other Highly Protein Bound Drugs
Raloxifene should be used with caution with certain other highly protein-bound drugs such as diazepam, diazoxide, and lidocaine. Although not examined, raloxifene might affect the protein binding of other drugs. Raloxifene is more than 95% bound to plasma proteins [see Clinical Pharmacology ( 12.3)] .
14.5 Effects On Cardiovascular Disease
In a randomized, placebo-controlled, double-blind, multinational clinical trial (RUTH) of 10,101 postmenopausal women with documented coronary heart disease or at increased risk for coronary events, no cardiovascular benefit was demonstrated after treatment with raloxifene hydrochloride 60 mg once daily for a median follow-up of 5.6 years. No significant increase or decrease was observed for coronary events (death from coronary causes, nonfatal myocardial infarction, or hospitalization for an acute coronary syndrome). An increased risk of death due to stroke after treatment with raloxifene hydrochloride was observed: 59 (1.2%) raloxifene hydrochloride-treated women died due to a stroke compared to 39 (0.8%) placebo-treated women (2.2 versus 1.5 per 1000 women-years; hazard ratio 1.49; 95% confidence interval, 1.00 to 2.24; p=0.0499). The incidence of stroke did not differ significantly between treatment groups (249 with raloxifene hydrochloride [4.9%] versus 224 with placebo [4.4%]; hazard ratio 1.10; 95% confidence interval 0.92 to 1.32; p=0.30; 9.5 versus 8.6 per 1000 women-years) [see Warnings and Precautions ( 5.2, 5.3)] .
13.2 Animal Toxicology And/or Pharmacology
The skeletal effects of raloxifene treatment were assessed in ovariectomized rats and monkeys. In rats, raloxifene prevented increased bone resorption and bone loss after ovariectomy. There were positive effects of raloxifene on bone strength, but the effects varied with time. Cynomolgus monkeys were treated with raloxifene or conjugated estrogens for 2 years. In terms of bone cycles, this is equivalent to approximately 6 years in humans. Raloxifene and estrogen suppressed bone turnover and increased BMD in the lumbar spine and in the central cancellous bone of the proximal tibia. In this animal model, there was a positive correlation between vertebral compressive breaking force and BMD of the lumbar spine.
Histologic examination of bone from rats and monkeys treated with raloxifene showed no evidence of woven bone, marrow fibrosis, or mineralization defects.
These results are consistent with data from human studies of radiocalcium kinetics and markers of bone metabolism, and are consistent with the action of raloxifene as a skeletal antiresorptive agent.
14.2 Prevention of Postmenopausal Osteoporosis
The effects of raloxifene on BMD in postmenopausal women were examined in three randomized, placebo-controlled, double-blind osteoporosis prevention trials: (1) a North American trial enrolled 544 women; (2) a European trial, 601 women; and (3) an international trial, 619 women who had undergone hysterectomy. In these trials, all women received calcium supplementation (400 to 600 mg/day). Women enrolled in these trials had a median age of 54 years and a median time since menopause of 5 years (less than 1 year up to 15 years postmenopause). The majority of the women were White (93.5%). Women were included if they had spine BMD between 2.5 standard deviations below and 2 standard deviations above the mean value for healthy young w omen. The mean T scores (number of standard deviations above or below the mean in healthy young women) for the three trials ranged from -1.01 to -0.74 for spine BMD and included women both with normal and low BMD. Raloxifene hydrochloride 60 mg administered once daily, produced increases in bone mass versus calcium supplementation alone, as reflected by dual-energy x-ray absorptiometric (DXA) measurements of hip, spine, and total body BMD.
2.2 Recommendations for Calcium and Vitamin D Supplementation
For either osteoporosis treatment or prevention, supplemental calcium and/or vitamin D should be added to the diet if daily intake is inadequate. Postmenopausal women require an average of 1500 mg/day of elemental calcium. Total daily intake of calcium above 1500 mg has not demonstrated additional bone benefits while daily intake above 2000 mg has been associated with increased risk of adverse effects, including hypercalcemia and kidney stones. The recommended intake of vitamin D is 400 to 800 IU daily. Patients at increased risk for vitamin D insufficiency (e.g., over the age of 70 years, nursing home bound, or chronically ill) may need additional vitamin D supplements. Patients with gastrointestinal malabsorption syndromes may require higher doses of vitamin D supplementation and measurement of 25-hydroxyvitamin D should be considered.
5.7 History of Hypertriglyceridemia When Treated With Estrogens
Limited clinical data suggest that some women with a history of marked hypertriglyceridemia (>5.6 mmol/L or >500 mg/dL) in response to treatment with oral estrogen or estrogen plus progestin may develop increased levels of triglycerides when treated with raloxifene. Women with this medical history should have serum triglycerides monitored when taking raloxifene.
1.1 Treatment and Prevention of Osteoporosis in Postmenopausal Women
Warning: Increased Risk of Venous Thromboembolism and Death From Stroke
- Increased risk of deep vein thrombosis and pulmonary embolism have been reported with raloxifene [see Warnings and Precautions ( 5.1)] . Women with active or past history of venous thromboembolism should not take raloxifene [see Contraindications ( 4.1)] .
- Increased risk of death due to stroke occurred in a trial in postmenopausal women with documented coronary heart disease or at increased risk for major coronary events. Consider risk-benefit balance in women at risk for stroke [see Warnings and Precautions ( 5.2) and Clinical Studies ( 14.5)] .
17.1 Osteoporosis Recommendations, Including Calcium and Vitamin D Supplementation
For osteoporosis treatment or prevention, patients should be instructed to take supplemental calcium and/or vitamin D if intake is inadequate. Patients at increased risk for vitamin D insufficiency (e.g., over the age of 70 years, nursing home bound, chronically ill, or with gastrointestinal malabsorption syndromes) should be instructed to take additional vitamin D if needed. Weight-bearing exercises should be considered along with the modification of certain behavioral factors, such as cigarette smoking and/or excessive alcohol consumption, if these factors exist.
1.2 Reduction in the Risk of Invasive Breast Cancer in Postmenopausal Women With Osteoporosis
Raloxifene hydrochloride tablets, USP is indicated for the reduction in risk of invasive breast cancer in postmenopausal women with osteoporosis [see Clinical Studies ( 14.3)] .
1.3 Reduction in the Risk of Invasive Breast Cancer in Postmenopausal Women At High Risk of Invasive Breast Cancer
Raloxifene hydrochloride tablets, USP is indicated for the reduction in risk of invasive breast cancer in postmenopausal women at high risk of invasive breast cancer [see Clinical Studies ( 14.4)] .
The effect in the reduction in the incidence of breast cancer was shown in a study of postmenopausal women at high risk for breast cancer with a 5-year planned duration with a median follow-up of 4.3 years [see Clinical Studies ( 14.4)] . Twenty-seven percent of the participants received drug for 5 years. The long-term effects and the recommended length of treatment are not known.
High risk of breast cancer is defined as at least one breast biopsy showing lobular carcinoma in situ (LCIS) or atypical hyperplasia, one or more first- degree relatives with breast cancer, or a 5-year predicted risk of breast cancer ≥1.66% (based on the modified Gail model). Among the factors included in the modified Gail model are the following: current age, number of first-degree relatives with breast cancer, number of breast biopsies, age at menarche, nulliparity or age of first live birth. Currently, no single clinical finding or test result can quantify risk of breast cancer with certainty.
After an assessment of the risk of developing breast cancer, the decision regarding therapy with raloxifene hydrochloride tablets, USP should be based upon an individual assessment of the benefits and risks.
Raloxifene hydrochloride tablets, USP does not eliminate the risk of breast cancer. Patients should have breast exams and mammograms before starting raloxifene hydrochloride tablets, USP and should continue regular breast exams and mammograms in keeping with good medical practice after beginning treatment with raloxifene hydrochloride tablets, USP.
Important Limitations of Use for Breast Cancer Risk Reduction
- There are no data available regarding the effect of raloxifene on invasive breast cancer incidence in women with inherited mutations (BRCA1, BRCA2) to be able to make specific recommendations on the effectiveness of raloxifene hydrochloride tablets, USP.
- Raloxifene hydrochloride tablets, USP is not indicated for the treatment of invasive breast cancer or reduction of the risk of recurrence.
- Raloxifene hydrochloride tablets, USP is not indicated for the reduction in the risk of noninvasive breast cancer.
17.4 Reduction in Risk of Invasive Breast Cancer in Postmenopausal Women With Osteoporosis Or At High Risk of Invasive Breast Cancer
Use of raloxifene hydrochloride tablets is associated with the reduction of the risk of invasive breast cancer in postmenopausal women. Raloxifene hydrochloride tablets has not been shown to reduce the risk of noninvasive breast cancer. When considering treatment, physicians need to discuss the potential benefits and risks of raloxifene hydrochloride tablets treatment with the patient.
Raloxifene hydrochloride tablets is not indicated for the treatment of invasive breast cancer or reduction of the risk of recurrence.
Patients should have breast exams and mammograms before starting raloxifene hydrochloride tablets, and should continue regular breast exams and mammograms in keeping with good medical practice after beginning treatment with raloxifene hydrochloride tablets
Structured Label Content
Principal Display Panel (PRINCIPAL DISPLAY PANEL)
NDC 50228-306-30
Raloxifene Hydrochloride Tablets, USP 60mg
PHARMACIST: Dispense the accompanying Medication Guide to each patient.
30 Tablets Rx Only
NDC 50228-306-20
Raloxifene Hydrochloride Tablets, USP 60mg
PHARMACIST: Dispense the accompanying Medication Guide to each patient.
2,000 Tablets Rx Only
Section 42229-5 (42229-5)
Osteoporosis Treatment Clinical Trial (MORE) — The safety of raloxifene in the treatment of osteoporosis was assessed in a large (7705 patients) multinational, placebo- controlled trial. Duration of treatment was 36 months, and 5129 postmenopausal women were exposed to raloxifene (2557 received 60 mg/day, and 2572 received 120 mg/day). The incidence of all-cause mortality was similar among groups: 23 (0.9%) placebo, 13 (0.5%) raloxifene-treated (raloxifene HCL 60mg), and 28 (1.1%) raloxifene HCL 120 mg women died. Therapy was discontinued due to an adverse reaction in 10.9% of raloxifene-treated women and 8.8% of placebo-treated women.
Venous Thromboembolism: The most serious adverse reaction related to raloxifene was VTE (deep venous thrombosis, pulmonary embolism, and retinal vein thrombosis). During an average of study-drug exposure of 2.6 years, VTE occurred in about 1 out of 100 patients treated with raloxifene. Twenty-six raloxifene-treated women had a VTE compared to 11 placebo-treated women, the hazard ratio was 2.4 (95% confidence interval, 1.2, 4.5), and the highest VTE risk was during the initial months of treatment.
Common adverse reactions considered to be related to raloxifene therapy were hot flashes and leg cramps. Hot flashes occurred in about one in 10 patients on raloxifene and were most commonly reported during the first 6 months of treatment and were not different from placebo thereafter. Leg cramps occurred in about one in 14 patients on raloxifene.
Section 42231-1 (42231-1)
Medication Guide
RALOXIFENE (ral.ox.i.fene) Hydrochloride Tablets, USP 60 mg for oral use
Read the Medication Guide that comes with raloxifene hydrochloride tablets before you start taking it and each time you refill your prescription. The information may have changed. This Medication Guide does not take the place of talking with your doctor about your medical condition or treatment. Talk with your doctor about raloxifene hydrochloride tablets when you start taking it and at regular checkups.
What is the most important information I should know about raloxifene hydrochloride tablets?
Serious and life-threatening side effects can occur while taking raloxifene hydrochloride tablets. These include blood clots and dying from stroke:
- Increased risk of blood clots in the legs (deep vein thrombosis) and lungs (pulmonary embolism) have been reported with raloxifene hydrochloride tablets. Women who have or have had blood clots in the legs, lungs, or eyes should not take raloxifene hydrochloride tablets.
- Women who have had a heart attack or are at risk for a heart attack may have an increased risk of dying from stroke when taking raloxifene hydrochloride tablets.
- Before starting raloxifene hydrochloride tablets, tell your doctor if you have had blood clots in your legs, lungs, or eyes, a stroke, mini-stroke (transient ischemic attack), or have an irregular heartbeat.
- Stop taking raloxifene hydrochloride tablets and call your doctor if you have:
- leg pain or a feeling of warmth in the lower leg (calf).
- swelling of the legs, hands, or feet.
- sudden chest pain, shortness of breath, or coughing up blood.
- sudden change in your vision, such as loss of vision or blurred vision.
- Being still for a long time (such as sitting still during a long car or airplane trip or being in bed after surgery) can increase your risk of blood clots. (See “ What should I avoid if I am taking raloxifene hydrochloride tablets?” )
What is raloxifene hydrochloride?
Raloxifene hydrochloride is a type of prescription medicine called a Selective Estrogen Receptor Modulator (SERM). Raloxifene hydrochloride tablets are for women after menopause, and has more than one use:
- Osteoporosis: Raloxifene hydrochloride tablets treats and prevents osteoporosis by helping make your bones stronger and less likely to break.
- Invasive Breast Cancer: If you have osteoporosis or are at high risk for breast cancer, raloxifene hydrochloride tablets can be used to lower your chance of getting invasive breast cancer. Raloxifene hydrochloride tablets will not totally get rid of your chance of getting breast cancer. Your doctor can estimate your risk of breast cancer by asking you about risk factors, including:
- your age (getting older).
- family history of breast cancer in your mother, sister, or daughter.
- a history of any breast biopsy, especially an abnormal biopsy.
You and your doctor should talk about whether the possible benefit of raloxifene hydrochloride tablets in lowering your chance of getting invasive breast cancer is greater than its possible risks.
Raloxifene hydrochloride tablets are not for use in premenopausal women (women who have not passed menopause).
Who should not take raloxifene hydrochloride tablets?
Do not take raloxifene hydrochloride tablets if you:
- have or have had blood clots in your legs, lungs, or eyes. Taking raloxifene hydrochloride tablets may increase the risk of getting blood clots.
- are pregnant or could become pregnant. Raloxifene hydrochloride tablets could harm your unborn child.
- are nursing a baby. It is not known if raloxifene passes into breast milk or what effect it might have on the baby.
What should I tell my doctor before taking raloxifene hydrochloride tablets?
Raloxifene hydrochloride tablets may not be right for you. Before taking raloxifene hydrochloride tablets, tell your doctor about all your medical conditions, including if you:
- have had blood clots in your legs, lungs, or eyes, a stroke, mini-stroke (TIA/transient ischemic attack), or a type of irregular heartbeat (atrial fibrillation).
- have had breast cancer. Raloxifene hydrochloride tablets have not been fully studied in women who have a history of breast cancer.
- have liver or kidney problems.
- have taken estrogen in the past and had a high increase of triglycerides (a kind of fat in the blood).
- are pregnant, planning to become pregnant, or breast-feeding (see “ Who should not take raloxifene hydrochloride tablets?” ).
Tell your doctor about all medicines you take, including prescription and non-prescription medicines, vitamins, and herbal supplements. Know the medicines you take. Keep a list of them and show it to your doctor and pharmacist each time you get a new medicine. Especially tell your doctor if you take*:
- warfarin (Coumadin
®, Jantoven
®)
If you are taking warfarin or other coumarin blood thinners, your doctor may need to do a blood test when you first start or if you need to stop taking raloxifene hydrochloride tablets. Names for this test include “prothrombin time,” “pro-time,” or “INR.” Your doctor may need to adjust the dose of your warfarin or other coumarin blood thinner. - cholestyramine
- estrogens
Raloxifene hydrochloride tablets should not be taken with cholestyramine or estrogens.
How should I take raloxifene hydrochloride tablets?
- Take raloxifene hydrochloride tablets exactly how your doctor tells you to.
- Keep taking raloxifene hydrochloride tablets for as long as your doctor prescribes it for you. It is not known how long you should keep taking raloxifene hydrochloride tablets to lower your chance of getting invasive breast cancers.
- It is important to get your refills on time so you do not run out of the medicine.
- Take one raloxifene hydrochloride tablets each day.
- Take raloxifene hydrochloride tablets at any time of the day, with or without food.
- To help you remember to take raloxifene hydrochloride tablets, it may be best to take it at about the same time each day.
- Calcium and vitamin D may be taken at the same time as raloxifene hydrochloride tablets. It is important to take calcium and vitamin D, as directed by your physician, to prevent or treat osteoporosis.
- If you miss a dose, take it as soon as you remember. However, if it is almost time for your next dose, skip the missed dose and take only your next regularly scheduled dose. Do not take two doses at the same time.
What should I avoid while taking raloxifene hydrochloride tablets?
- Being still for a long time (such as during long trips or being in bed after surgery) can increase the risk of blood clots. Raloxifene hydrochloride tablets may add to this risk. If you will need to be still for a long time, talk with your doctor about ways to reduce the risk of blood clots. On long trips, move around periodically. Stop taking raloxifene hydrochloride tablets at least 3 days before a planned surgery or before you plan on being still for a long time. You should start taking raloxifene hydrochloride tablets again when you return to your normal activities.
- Some medicines should not be taken with raloxifene hydrochloride tablets (see “ What should I tell my doctor before taking raloxifene hydrochloride tablets?” ).
What are the possible side effects of raloxifene hydrochloride tablets?
Serious and life-threatening side effects can occur while taking raloxifene hydrochloride tablets. These include blood clots and dying from stroke:
- Increased risk of blood clots in the legs (deep vein thrombosis) and lungs (pulmonary embolism) have been reported with raloxifene hydrochloride tablets. Women who have or have had blood clots in the legs, lungs, or eyes should not take raloxifene hydrochloride tablets.
- Women who have had a heart attack or are at risk for a heart attack may have an increased risk of dying from stroke when taking raloxifene hydrochloride tablets .
See “ What is the most important information I should know about raloxifene hydrochloride tablets?”
The most common side effects of raloxifene hydrochloride tablets are hot flashes, leg cramps, swelling of the feet, ankles, and legs, flu syndrome, joint pain, and sweating. Hot flashes are more common during the first 6 months after starting treatment.
These are not all the side effects of raloxifene hydrochloride tablets. Tell your doctor about any side effect that bothers you or that does not go away. If you have any problems or questions that concern you while taking raloxifene hydrochloride tablets? ask your doctor or pharmacist for more information.
What else should I know about raloxifene hydrochloride tablets?
- Do not use raloxifene hydrochloride tablets to prevent heart disease, heart attack, or strokes.
- To get the calcium and vitamin D you need, your doctor may advise you to change your diet and/or take supplemental calcium and vitamin D. Your doctor may suggest other ways to help treat or prevent osteoporosis, in addition to taking raloxifene hydrochloride tablets and getting the calcium and vitamin D you need. These may include regular exercise, stopping smoking, and drinking less alcohol.
- Women who have hot flashes can take raloxifene hydrochloride. Raloxifene hydrochloride tablets do not treat hot flashes, and it may cause hot flashes in some women. (See “ What are the possible side effects of raloxifene hydrochloride?” )
- Raloxifene hydrochloride tablets have not been found to cause breast tenderness or enlargement. If you notice any changes in your breasts, call your doctor to find out the cause. Before starting and while taking raloxifene hydrochloride tablets you should have breast exams and mammograms, as directed by your doctor. Because raloxifene hydrochloride tablets does not eliminate the chance of developing breast cancers, you need these examinations to find any breast cancers as early as possible.
- Raloxifene hydrochloride tablets should not cause spotting or menstrual-type bleeding. If you have any vaginal bleeding, call your doctor to find out the cause. Raloxifene hydrochloride tablets have not been found to increase the risk for cancer of the lining of the uterus.
- Women in clinical trials have taken raloxifene hydrochloride tablets for up to eight years.
How should I store raloxifene hydrochloride tablets?
- Store raloxifene hydrochloride tablets at 68°F to 77°F (20°C to 25°C).
- Keep raloxifene hydrochloride tablets and all medicines out of the reach of children.
General Information about the safe and effective use of raloxifene hydrochloride tablets
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use raloxifene hydrochloride tablets for a condition for which it was not prescribed. Do not give your raloxifene hydrochloride tablets to other people, even if they have the same symptoms you have. It may harm them.
This Medication Guide is a summary of the most important information about raloxifene hydrochloride tablets. If you would like more information about raloxifene hydrochloride tablets, talk with your doctor. You can ask your doctor or pharmacist for information about raloxifene hydrochloride tablets that is written for health professionals. For more information, call 1-855-724-3436 (toll-free).
What are the ingredients in raloxifene hydrochloride tablets, USP?
Active Ingredient: raloxifene hydrochloride USP
Inactive Ingredients: citric acid monohydrate, crospovidone, hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate 80, povidone and titanium dioxide.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
*The brands listed are trademarks of their respective owners and are not trademarks of ScieGen Pharmaceuticals Inc. The makers of these brands are not affiliated with and do not endorse ScieGen Pharmaceuticals Inc and company or its products.
Manufactured by:
ScieGen Pharmaceuticals, Inc.
Huappauge, NY 11788, USA
Revision: 6/18
Section 43683-2 (43683-2)
7.2 Warfarin
If raloxifene is given concomitantly with warfarin or other warfarin derivatives, prothrombin time should be monitored more closely when starting or stopping therapy with raloxifene [see Clinical Pharmacology ( 12.3)] .
10 Overdosage (10 OVERDOSAGE)
In an 8-week study of 63 postmenopausal women, a dose of raloxifene hydrochloride (HCL) 600 mg/day was safely tolerated. In clinical trials, no raloxifene overdose has been reported.
In postmarketing spontaneous reports, raloxifene overdose has been reported very rarely (less than 1 out of 10,000 [<0.01%] patients treated). The highest overdose has been approximately 1.5 grams. No fatalities associated with raloxifene overdose have been reported. Adverse reactions were reported in approximately half of the adults who took ≥180 mg raloxifene HCL and included leg cramps and dizziness.
Two 18-month-old children each ingested raloxifene HCL 180 mg. In these two children, symptoms reported included ataxia, dizziness, vomiting, rash, diarrhea, tremor, and flushing, as well as elevation in alkaline phosphatase.
There is no specific antidote for raloxifene.
No mortality was seen after a single oral dose in rats or mice at 5000 mg/kg (810 times the human dose for rats and 405 times the human dose for mice based on surface area, mg/m 2) or in monkeys at 1000 mg/kg (80 times the AUC in humans).
4.2 Pregnancy
Raloxifene hydrochloride tablets, USP is contraindicated for use in pregnancy, as it may cause fetal harm [see Use in Specific Populations ( 8.1)] .
11 Description (11 DESCRIPTION)
Raloxifene Hydrochloride is an estrogen agonist/antagonist, commonly referred to as a selective estrogen receptor modulator (SERM) that belongs to the benzothiophene class of compounds. The chemical structure is:
The chemical designation is methanone, [6-hydroxy-2-(4-hydroxyphenyl)benzo[ b ]thien-3-yl]-[4-[2-(1-piperidinyl)ethoxy]phenyl]-, hydrochloride. Raloxifene hydrochloride (HCl) has the empirical formula C 28H 27NO 4S•HCl, which corresponds to a molecular weight of 510.04. Raloxifene Hydrochloride USP is an Almost white to pale yellow powder that freely soluble in dimethyl sulfoxide, practically insoluble in ether and in ethyl acetate.
Raloxifene hydrochloride tablets USP, 60 mg is supplied in a tablet dosage form for oral administration. Each raloxifene hydrochloride tablets USP, 60 mg contains 60 mg of raloxifene HCl, which is the molar equivalent of 55.71 mg of free base. Inactive ingredients include citric acid monohydrate, crospovidone, hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, polysorbate 80, povidone and titanium dioxide.
USP Dissolution Test is pending.
5.10 Use in Men
There is no indication for the use of raloxifene in men. Raloxifene has not been adequately studied in men and its use is not recommended.
16.1 How Supplied
Raloxifene hydrochloride tablets, USP 60 mg tablets are white to off-white, oval, biconvex, film coated tablets, debossed with ‘SG’ on one side and ‘306’ on other side. They are available as follows:
Bottle (count)
NDC Number
30 (unit of use) NDC 50228-306-30
2000
NDC 50228-306-20
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
Of the total number of patients in placebo-controlled clinical studies of raloxifene, 61% were 65 and over, while 15.5% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. Based on clinical trials, there is no need for dose adjustment for geriatric patients [see Clinical Pharmacology ( 12.3)] .
7.1 Cholestyramine
Concomitant administration of cholestyramine with raloxifene is not recommended. Although not specifically studied, it is anticipated that other anion exchange resins would have a similar effect. Raloxifene should not be co-administered with other anion exchange resins [see Clinical Pharmacology ( 12.3)] .
4 Contraindications (4 CONTRAINDICATIONS)
6 Adverse Reactions (6 ADVERSE REACTIONS)
Adverse reactions (>2% and more common than with placebo) include: hot flashes, leg cramps, peripheral edema, flu syndrome, arthralgia, sweating. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ScieGen Pharmaeuticals Inc at 1-855-724-3436 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions (7 DRUG INTERACTIONS)
- Cholestyramine: Use with raloxifene is not recommended. Reduces the absorption and enterohepatic cycling of raloxifene. ( 7.1, 12.3)
- Warfarin: Monitor prothrombin time when starting or stopping raloxifene. ( 7.2, 12.3)
- Highly Protein-Bound Drugs: Use with raloxifene with caution. Highly protein-bound drugs include diazepam, diazoxide, and lidocaine. Raloxifene is more than 95% bound to plasma proteins. ( 7.3, 12.3)
5.8 Renal Impairment
Raloxifene should be used with caution in patients with moderate or severe renal impairment. Safety and efficacy have not been established in patients with moderate or severe renal impairment [see Clinical Pharmacology ( 12.3)] .
8.6 Renal Impairment
12.2 Pharmacodynamics
Decreases in estrogen levels after oophorectomy or menopause lead to increases in bone resorption and accelerated bone loss. Bone is initially lost rapidly because the compensatory increase in bone formation is inadequate to offset resorptive losses. In addition to loss of estrogen, this imbalance between resorption and formation may be due to age-related impairment of osteoblasts or their precursors. In some women, these changes will eventually lead to decreased bone mass, osteoporosis, and increased risk for fractures, particularly of the spine, hip, and wrist. Vertebral fractures are the most common type of osteoporotic fracture in postmenopausal women.
In both the osteoporosis treatment and prevention trials, raloxifene resulted in consistent, statistically significant suppression of bone resorption and bone formation, as reflected by changes in serum and urine markers of bone turnover (e.g., bone-specific alkaline phosphatase, osteocalcin, and collagen breakdown products). The suppression of bone turnover markers was evident by 3 months and persisted throughout the 36-month and 24-month observation periods.
In a 31-week, open-label, radiocalcium kinetics study, 33 early postmenopausal women were randomized to treatment with once-daily raloxifene hydrochloride 60 mg, cyclic estrogen/progestin (0.625 mg conjugated estrogens daily with 5 mg medroxyprogesterone acetate daily for the first 2 weeks of each month [hormone therapy]), or no treatment. Treatment with either raloxifene or hormone therapy was associated with reduced bone resorption and a positive shift in calcium balance (-82 mg Ca/day and +60 mg Ca/day, respectively, for raloxifene and -162 mg Ca/day and +91 mg Ca/day, respectively, for hormone therapy). There were small decreases in serum total calcium, inorganic phosphate, total protein, and albumin, which were generally of lesser magnitude than decreases observed during estrogen or hormone therapy. Platelet count was also decreased slightly and was not different from estrogen therapy.
12.3 Pharmacokinetics
The disposition of raloxifene has been evaluated in more than 3000 postmenopausal women in selected raloxifene osteoporosis treatment and prevention clinical trials, using a population approach. Pharmacokinetic data also were obtained in conventional pharmacology studies in 292 postmenopausal women. Raloxifene exhibits high within-subject variability (approximately 30% coefficient of variation) of most pharmacokinetic parameters. Table 3 summarizes the pharmacokinetic parameters of raloxifene.
Absorption — Raloxifene is absorbed rapidly after oral administration. Approximately 60% of an oral dose is absorbed, but presystemic glucuronide conjugation is extensive. Absolute bioavailability of raloxifene is 2%. The time to reach average maximum plasma concentration and bioavailability are functions of systemic interconversion and enterohepatic cycling of raloxifene and its glucuronide metabolites. Administration of raloxifene HCl with a standardized, high-fat meal increases the absorption of raloxifene (C max 28% and AUC 16%), but does not lead to clinically meaningful changes in systemic exposure. Raloxifene can be administered without regard to meals.
Distribution — Following oral administration of single doses ranging from 30 to 150 mg of raloxifene HCl, the apparent volume of distribution is 2348 L/kg and is not dose dependent. Raloxifene and the monoglucuronide conjugates are highly (95%) bound to plasma proteins. Raloxifene binds to both albumin and α1-acid glycoprotein, but not to sex-steroid binding globulin.
Metabolism — Biotransformation and disposition of raloxifene in humans have been determined following oral administration of 14C-labeled raloxifene. Raloxifene undergoes extensive first-pass metabolism to the glucuronide conjugates: raloxifene-4′-glucuronide, raloxifene-6-glucuronide, and raloxifene-6,4′-diglucuronide. No other metabolites have been detected, providing strong evidence that raloxifene is not metabolized by cytochrome P450 pathways. Unconjugated raloxifene comprises less than 1% of the total radiolabeled material in plasma. The terminal log-linear portions of the plasma concentration curves for raloxifene and the glucuronides are generally parallel. This is consistent with interconversion of raloxifene and the glucuronide metabolites. Following intravenous administration, raloxifene is cleared at a rate approximating hepatic blood flow. Apparent oral clearance is 44.1 L/kg•hr. Raloxifene and its glucuronide conjugates are interconverted by reversible systemic metabolism and enterohepatic cycling, thereby prolonging its plasma elimination half-life to 27.7 hours after oral dosing. Results from single oral doses of raloxifene predict multiple-dose pharmacokinetics. Following chronic dosing, clearance ranges from 40 to 60 L/kg•hr. Increasing doses of raloxifene HCl (ranging from 30 to 150 mg) result in slightly less than a proportional increase in the area under the plasma time concentration curve (AUC).
Excretion — Raloxifene is primarily excreted in feces, and less than 0.2% is excreted unchanged in urine. Less than 6% of the raloxifene dose is eliminated in urine as glucuronide conjugates.
|
a Abbreviations: C max = maximum plasma concentration, t 1/2 = half-life, AUC = area under the curve, CL = clearance, V = volume of distribution, F = bioavailability, CV = coefficient of variation. |
|||||
|
b Data normalized for dose in mg and body weight in kg. |
|||||
|
c Range of observed half-life. |
|||||
|
C
max
a, b
(ng/mL)/ (mg/kg) |
t 1/2 (hr) a |
AUC
0-
∞
a, b
(ng•hr/mL)/ (mg/kg) |
CL/F
a
(L/kg•hr) |
V/F
a
(L/kg) |
|
|
Single Dose
Mean |
0.50 | 27.7 | 27.2 | 44.1 | 2348 |
| CV a (%) | 52 | 10.7 to 273 c | 44 | 46 | 52 |
|
Multiple Dose
Mean |
1.36 | 32.5 | 24.2 | 47.4 | 2853 |
| CV a (%) | 37 | 15.8 to 86.6 c | 36 | 41 | 56 |
Special Populations
Pediatric — The pharmacokinetics of raloxifene has not been evaluated in a pediatric population [see Use in Specific Populations ( 8.4)] .
Geriatric — No differences in raloxifene pharmacokinetics were detected with regard to age (range 42 to 84 years) [see Use in Specific Populations ( 8.5)] .
Gender — Total extent of exposure and oral clearance, normalized for lean body weight, are not significantly different between age-matched female and male volunteers.
Race — Pharmacokinetic differences due to race have been studied in 1712 women, including 97.5% White, 1.0% Asian, 0.7% Hispanic, and 0.5% Black in the osteoporosis treatment trial and in 1053 women, including 93.5% White, 4.3% Hispanic, 1.2% Asian, and 0.5% Black in the osteoporosis prevention trials. There were no discernible differences in raloxifene plasma concentrations among these groups; however, the influence of race cannot be conclusively determined.
5.4 Premenopausal Use
There is no indication for premenopausal use of raloxifene. Safety of raloxifene in premenopausal women has not been established and its use is not recommended.
Additionally, there is concern regarding inadvertent drug exposure in pregnancy in women of reproductive potential who become pregnant, due to risk of fetal harm [see Use in Specific Populations ( 8.1)] .
2.1 Recommended Dosing
The recommended dosage is one raloxifene hydrochloride tablets, USP 60 mg daily, which may be administered any time of day without regard to meals [see Clinical Pharmacology ( 12.3)] .
For the indications in risk of invasive breast cancer the optimum duration of treatment is not known [see Clinical Studies ( 14.3, 14.4)] .
5.5 Hepatic Impairment
Raloxifene should be used with caution in patients with hepatic impairment. Safety and efficacy have not been established in patients with hepatic impairment [see Clinical Pharmacology ( 12.3)] .
7.4 Systemic Estrogens
The safety of concomitant use of raloxifene with systemic estrogens has not been established and its use is not recommended.
8.7 Hepatic Impairment
1 Indications and Usage (1 INDICATIONS AND USAGE)
Raloxifene hydrochloride tablets, USP is an estrogen agonist/antagonist indicated for:
- Treatment and prevention of osteoporosis in postmenopausal women. ( 1.1)
- Reduction in risk of invasive breast cancer in postmenopausal women with osteoporosis. ( 1.2)
- Reduction in risk of invasive breast cancer in postmenopausal women at high risk for invasive breast cancer. ( 1.3)
Important Limitations: Raloxifene hydrochloride tablets, USP is not indicated for the treatment of invasive breast cancer, reduction of the risk of recurrence of breast cancer, or reduction of risk of noninvasive breast cancer.
5.2 Death Due to Stroke
In a clinical trial of postmenopausal women with documented coronary heart disease or at increased risk for coronary events, an increased risk of death due to stroke was observed after treatment with raloxifene. During an average follow-up of 5.6 years, 59 (1.2%) raloxifene-treated women died due to a stroke compared to 39 (0.8%) placebo-treated women (22 versus 15 per 10,000 women-years; hazard ratio 1.49; 95% confidence interval, 1.00 to 2.24; p=0.0499). There was no statistically significant difference between treatment groups in the incidence of stroke (249 in raloxifene [4.9%] versus 224 placebo [4.4%]). Raloxifene had no significant effect on all-cause mortality. The risk-benefit balance should be considered in women at risk for stroke, such as prior stroke or transient ischemic attack (TIA), atrial fibrillation, hypertension, or cigarette smoking [see Clinical Studies ( 14.5)] .
12.1 Mechanism of Action
Raloxifene is an estrogen agonist/antagonist, commonly referred to as a selective estrogen receptor modulator (SERM). The biological actions of raloxifene are largely mediated through binding to estrogen receptors. This binding results in activation of estrogenic pathways in some tissues (agonism) and blockade of estrogenic pathways in others (antagonism). The agonistic or antagonistic action of raloxifene depends on the extent of recruitment of coactivators and corepressors to estrogen receptor (ER) target gene promoters.
Raloxifene appears to act as an estrogen agonist in bone. It decreases bone resorption and bone turnover, increases bone mineral density (BMD) and decreases fracture incidence. Preclinical data demonstrate that raloxifene is an estrogen antagonist in uterine and breast tissues. These results are consistent with findings in clinical trials, which suggest that raloxifene lacks estrogen-like effects on the uterus and breast tissue.
16.2 Storage and Handling
Store at controlled room temperature, 20° to 25°C (68° to 77°F) [ see USP]. The USP defines controlled room temperature as a temperature maintained thermostatically that encompasses the usual and customary working environment of 20° to 25°C (68° to 77°F); that results in a mean kinetic temperature calculated to be not more than 25°C; and that allows for excursions between 15° and 30°C (59° and 86°F) that are experienced in pharmacies, hospitals, and warehouses.
5.12 Breast Abnormalities
Any unexplained breast abnormality occurring during raloxifene therapy should be investigated. Raloxifene does not eliminate the risk of breast cancer [see Clinical Studies ( 14.4)] .
4.1 Venous Thromboembolism
Raloxifene is contraindicated in women with active or past history of venous thromboembolism (VTE), including deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis [see Warnings and Precautions ( 5.1)] .
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Venous Thromboembolism: Increased risk of deep vein thrombosis, pulmonary embolism, and retinal vein thrombosis. Discontinue use 72 hours prior to and during prolonged immobilization. ( 5.1, 6.1)
- Death Due to Stroke: Increased risk of death due to stroke occurred in a trial in postmenopausal women with documented coronary heart disease or at increased risk for major coronary events. No increased risk of stroke was seen in this trial. Consider risk-benefit balance in women at risk for stroke. ( 5.2, 14.5)
- Cardiovascular Disease: Raloxifene should not be used for the primary or secondary prevention of cardiovascular disease. ( 5.3, 14.5)
- Premenopausal Women: Use is not recommended. ( 5.4)
- Hepatic Impairment: Use with caution. ( 5.5)
- Concomitant Use with Systemic Estrogens: Not recommended. ( 5.6)
- Hypertriglyceridemia: If previous treatment with estrogen resulted in hypertriglyceridemia, monitor serum triglycerides. ( 5.7)
5.1 Venous Thromboembolism
In clinical trials, raloxifene-treated women had an increased risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism). Other venous thromboembolic events also could occur. A less serious event, superficial thrombophlebitis, also has been reported more frequently with raloxifene than with placebo. The greatest risk for deep vein thrombosis and pulmonary embolism occurs during the first 4 months of treatment, and the magnitude of risk appears to be similar to the reported risk associated with use of hormone therapy. Because immobilization increases the risk for venous thromboembolic events independent of therapy, raloxifene should be discontinued at least 72 hours prior to and during prolonged immobilization (e.g., post-surgical recovery, prolonged bed rest), and raloxifene therapy should be resumed only after the patient is fully ambulatory. In addition, women taking raloxifene should be advised to move about periodically during prolonged travel. The risk-benefit balance should be considered in women at risk of thromboembolic disease for other reasons, such as congestive heart failure, superficial thrombophlebitis, and active malignancy [see Contraindications ( 4.1) and Adverse Reactions ( 6.1)] .
5.3 Cardiovascular Disease
Raloxifene should not be used for the primary or secondary prevention of cardiovascular disease. In a clinical trial of postmenopausal women with documented coronary heart disease or at increased risk for coronary events, no cardiovascular benefit was demonstrated after treatment with raloxifene for 5 years [see Clinical Studies ( 14.5)] .
17.2 Patient Immobilization
Raloxifene hydrochloride tablets should be discontinued at least 72 hours prior to and during prolonged immobilization (e.g., post-surgical recovery, prolonged bed rest), and patients should be advised to avoid prolonged restrictions of movement during travel because of the increased risk of venous thromboembolic events [see Warnings and Precautions ( 5.1)] .
17.3 Hot Flashes Or Flushes (17.3 Hot Flashes or Flushes)
Raloxifene hydrochloride tablets may increase the incidence of hot flashes and is not effective in reducing hot flashes or flushes associated with estrogen deficiency. In some asymptomatic patients, hot flashes may occur upon beginning raloxifene hydrochloride tablets therapy.
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
60 mg tablet orally once daily. ( 2.1)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
60 mg, white to off-white, oval, biconvex, film coated tablets (not scored). They are debossed with ‘SG’ on one side and ‘306’ on other side.
5.9 History of Breast Cancer
Raloxifene has not been adequately studied in women with a prior history of breast cancer.
6.2 Postmarketing Experience
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Adverse reactions reported very rarely since market introduction include retinal vein occlusion, stroke, and death associated with venous thromboembolism (VTE).
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Pediatric Use: Safety and effectiveness not established. ( 8.4)
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described below reflect exposure to raloxifene in 8429 patients who were enrolled in placebo-controlled trials, including 6666 exposed for 1 year and 5685 for at least 3 years.
5.6 Concomitant Estrogen Therapy
The safety of concomitant use of raloxifene with systemic estrogens has not been established and its use is not recommended.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
See FDA-approved Medication Guide.
Physicians should instruct their patients to read the Medication Guide before starting therapy with Raloxifene hydrochloride tablets, and to reread it each time the prescription is renewed.
5.11 Unexplained Uterine Bleeding
7.5 Other Concomitant Medications
Raloxifene can be concomitantly administered with ampicillin, amoxicillin, antacids, corticosteroids, and digoxin [see Clinical Pharmacology ( 12.3)] .
The concomitant use of raloxifene and lipid-lowering agents has not been studied.
7.3 Other Highly Protein Bound Drugs (7.3 Other Highly Protein-Bound Drugs)
Raloxifene should be used with caution with certain other highly protein-bound drugs such as diazepam, diazoxide, and lidocaine. Although not examined, raloxifene might affect the protein binding of other drugs. Raloxifene is more than 95% bound to plasma proteins [see Clinical Pharmacology ( 12.3)] .
14.5 Effects On Cardiovascular Disease (14.5 Effects on Cardiovascular Disease)
In a randomized, placebo-controlled, double-blind, multinational clinical trial (RUTH) of 10,101 postmenopausal women with documented coronary heart disease or at increased risk for coronary events, no cardiovascular benefit was demonstrated after treatment with raloxifene hydrochloride 60 mg once daily for a median follow-up of 5.6 years. No significant increase or decrease was observed for coronary events (death from coronary causes, nonfatal myocardial infarction, or hospitalization for an acute coronary syndrome). An increased risk of death due to stroke after treatment with raloxifene hydrochloride was observed: 59 (1.2%) raloxifene hydrochloride-treated women died due to a stroke compared to 39 (0.8%) placebo-treated women (2.2 versus 1.5 per 1000 women-years; hazard ratio 1.49; 95% confidence interval, 1.00 to 2.24; p=0.0499). The incidence of stroke did not differ significantly between treatment groups (249 with raloxifene hydrochloride [4.9%] versus 224 with placebo [4.4%]; hazard ratio 1.10; 95% confidence interval 0.92 to 1.32; p=0.30; 9.5 versus 8.6 per 1000 women-years) [see Warnings and Precautions ( 5.2, 5.3)] .
13.2 Animal Toxicology And/or Pharmacology (13.2 Animal Toxicology and/or Pharmacology)
The skeletal effects of raloxifene treatment were assessed in ovariectomized rats and monkeys. In rats, raloxifene prevented increased bone resorption and bone loss after ovariectomy. There were positive effects of raloxifene on bone strength, but the effects varied with time. Cynomolgus monkeys were treated with raloxifene or conjugated estrogens for 2 years. In terms of bone cycles, this is equivalent to approximately 6 years in humans. Raloxifene and estrogen suppressed bone turnover and increased BMD in the lumbar spine and in the central cancellous bone of the proximal tibia. In this animal model, there was a positive correlation between vertebral compressive breaking force and BMD of the lumbar spine.
Histologic examination of bone from rats and monkeys treated with raloxifene showed no evidence of woven bone, marrow fibrosis, or mineralization defects.
These results are consistent with data from human studies of radiocalcium kinetics and markers of bone metabolism, and are consistent with the action of raloxifene as a skeletal antiresorptive agent.
14.2 Prevention of Postmenopausal Osteoporosis
The effects of raloxifene on BMD in postmenopausal women were examined in three randomized, placebo-controlled, double-blind osteoporosis prevention trials: (1) a North American trial enrolled 544 women; (2) a European trial, 601 women; and (3) an international trial, 619 women who had undergone hysterectomy. In these trials, all women received calcium supplementation (400 to 600 mg/day). Women enrolled in these trials had a median age of 54 years and a median time since menopause of 5 years (less than 1 year up to 15 years postmenopause). The majority of the women were White (93.5%). Women were included if they had spine BMD between 2.5 standard deviations below and 2 standard deviations above the mean value for healthy young w omen. The mean T scores (number of standard deviations above or below the mean in healthy young women) for the three trials ranged from -1.01 to -0.74 for spine BMD and included women both with normal and low BMD. Raloxifene hydrochloride 60 mg administered once daily, produced increases in bone mass versus calcium supplementation alone, as reflected by dual-energy x-ray absorptiometric (DXA) measurements of hip, spine, and total body BMD.
2.2 Recommendations for Calcium and Vitamin D Supplementation
For either osteoporosis treatment or prevention, supplemental calcium and/or vitamin D should be added to the diet if daily intake is inadequate. Postmenopausal women require an average of 1500 mg/day of elemental calcium. Total daily intake of calcium above 1500 mg has not demonstrated additional bone benefits while daily intake above 2000 mg has been associated with increased risk of adverse effects, including hypercalcemia and kidney stones. The recommended intake of vitamin D is 400 to 800 IU daily. Patients at increased risk for vitamin D insufficiency (e.g., over the age of 70 years, nursing home bound, or chronically ill) may need additional vitamin D supplements. Patients with gastrointestinal malabsorption syndromes may require higher doses of vitamin D supplementation and measurement of 25-hydroxyvitamin D should be considered.
5.7 History of Hypertriglyceridemia When Treated With Estrogens (5.7 History of Hypertriglyceridemia when Treated with Estrogens)
Limited clinical data suggest that some women with a history of marked hypertriglyceridemia (>5.6 mmol/L or >500 mg/dL) in response to treatment with oral estrogen or estrogen plus progestin may develop increased levels of triglycerides when treated with raloxifene. Women with this medical history should have serum triglycerides monitored when taking raloxifene.
1.1 Treatment and Prevention of Osteoporosis in Postmenopausal Women
Warning: Increased Risk of Venous Thromboembolism and Death From Stroke (WARNING: INCREASED RISK OF VENOUS THROMBOEMBOLISM AND DEATH FROM STROKE)
- Increased risk of deep vein thrombosis and pulmonary embolism have been reported with raloxifene [see Warnings and Precautions ( 5.1)] . Women with active or past history of venous thromboembolism should not take raloxifene [see Contraindications ( 4.1)] .
- Increased risk of death due to stroke occurred in a trial in postmenopausal women with documented coronary heart disease or at increased risk for major coronary events. Consider risk-benefit balance in women at risk for stroke [see Warnings and Precautions ( 5.2) and Clinical Studies ( 14.5)] .
17.1 Osteoporosis Recommendations, Including Calcium and Vitamin D Supplementation
For osteoporosis treatment or prevention, patients should be instructed to take supplemental calcium and/or vitamin D if intake is inadequate. Patients at increased risk for vitamin D insufficiency (e.g., over the age of 70 years, nursing home bound, chronically ill, or with gastrointestinal malabsorption syndromes) should be instructed to take additional vitamin D if needed. Weight-bearing exercises should be considered along with the modification of certain behavioral factors, such as cigarette smoking and/or excessive alcohol consumption, if these factors exist.
1.2 Reduction in the Risk of Invasive Breast Cancer in Postmenopausal Women With Osteoporosis (1.2 Reduction in the Risk of Invasive Breast Cancer in Postmenopausal Women with Osteoporosis)
Raloxifene hydrochloride tablets, USP is indicated for the reduction in risk of invasive breast cancer in postmenopausal women with osteoporosis [see Clinical Studies ( 14.3)] .
1.3 Reduction in the Risk of Invasive Breast Cancer in Postmenopausal Women At High Risk of Invasive Breast Cancer (1.3 Reduction in the Risk of Invasive Breast Cancer in Postmenopausal Women at High Risk of Invasive Breast Cancer)
Raloxifene hydrochloride tablets, USP is indicated for the reduction in risk of invasive breast cancer in postmenopausal women at high risk of invasive breast cancer [see Clinical Studies ( 14.4)] .
The effect in the reduction in the incidence of breast cancer was shown in a study of postmenopausal women at high risk for breast cancer with a 5-year planned duration with a median follow-up of 4.3 years [see Clinical Studies ( 14.4)] . Twenty-seven percent of the participants received drug for 5 years. The long-term effects and the recommended length of treatment are not known.
High risk of breast cancer is defined as at least one breast biopsy showing lobular carcinoma in situ (LCIS) or atypical hyperplasia, one or more first- degree relatives with breast cancer, or a 5-year predicted risk of breast cancer ≥1.66% (based on the modified Gail model). Among the factors included in the modified Gail model are the following: current age, number of first-degree relatives with breast cancer, number of breast biopsies, age at menarche, nulliparity or age of first live birth. Currently, no single clinical finding or test result can quantify risk of breast cancer with certainty.
After an assessment of the risk of developing breast cancer, the decision regarding therapy with raloxifene hydrochloride tablets, USP should be based upon an individual assessment of the benefits and risks.
Raloxifene hydrochloride tablets, USP does not eliminate the risk of breast cancer. Patients should have breast exams and mammograms before starting raloxifene hydrochloride tablets, USP and should continue regular breast exams and mammograms in keeping with good medical practice after beginning treatment with raloxifene hydrochloride tablets, USP.
Important Limitations of Use for Breast Cancer Risk Reduction
- There are no data available regarding the effect of raloxifene on invasive breast cancer incidence in women with inherited mutations (BRCA1, BRCA2) to be able to make specific recommendations on the effectiveness of raloxifene hydrochloride tablets, USP.
- Raloxifene hydrochloride tablets, USP is not indicated for the treatment of invasive breast cancer or reduction of the risk of recurrence.
- Raloxifene hydrochloride tablets, USP is not indicated for the reduction in the risk of noninvasive breast cancer.
17.4 Reduction in Risk of Invasive Breast Cancer in Postmenopausal Women With Osteoporosis Or At High Risk of Invasive Breast Cancer (17.4 Reduction in Risk of Invasive Breast Cancer in Postmenopausal Women with Osteoporosis or at High Risk of Invasive Breast Cancer)
Use of raloxifene hydrochloride tablets is associated with the reduction of the risk of invasive breast cancer in postmenopausal women. Raloxifene hydrochloride tablets has not been shown to reduce the risk of noninvasive breast cancer. When considering treatment, physicians need to discuss the potential benefits and risks of raloxifene hydrochloride tablets treatment with the patient.
Raloxifene hydrochloride tablets is not indicated for the treatment of invasive breast cancer or reduction of the risk of recurrence.
Patients should have breast exams and mammograms before starting raloxifene hydrochloride tablets, and should continue regular breast exams and mammograms in keeping with good medical practice after beginning treatment with raloxifene hydrochloride tablets
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:37:38.956660 · Updated: 2026-03-14T21:51:11.794870