Zoledronic Acid Injection
6a153c94-3cb5-4c05-98b2-1e18f5f3fe80
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Zoledronic acid injection is a bisphosphonate indicated for the treatment of: Hypercalcemia of malignancy. ( 1.1 ) Patients with multiple myeloma and patients with documented bone metastases from solid tumors, in conjunction with standard antineoplastic therapy. Prostate cancer should have progressed after treatment with at least one hormonal therapy. ( 1.2 ) Limitations of Use: The safety and efficacy of zoledronic acid injection has not been established for use in hyperparathyroidism or non-tumor-related hypercalcemia.
Dosage and Administration
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Contraindications
Hypersensitivity to any component of zoledronic acid injection ( 4 )
Warnings and Precautions
Patients being treated with zoledronic acid injection should not be treated with Reclast ® . ( 5.1 ) Adequately rehydrate patients with hypercalcemia of malignancy prior to administration of zoledronic acid injection and monitor electrolytes during treatment. ( 5.2 ) Renal toxicity may be greater in patients with renal impairment. Do not use doses greater than 4 mg. Treatment in patients with severe renal impairment is not recommended. Monitor serum creatinine before each dose. ( 5.3 ) Osteonecrosis of the jaw (ONJ) has been reported. Preventive dental exams should be performed before starting zoledronic acid injection. Avoid invasive dental procedures. ( 5.4 ) Severe incapacitating bone, joint, and/or muscle pain may occur. Discontinue zoledronic acid injection if severe symptoms occur. ( 5.5 ) Atypical subtrochanteric and diaphyseal femoral fractures have been reported in patients receiving bisphosphonate therapy. These fractures may occur after minimal or no trauma. Evaluate patients with thigh or groin pain to rule out a femoral fracture. Consider drug discontinuation in patients suspected to have an atypical femur fracture. ( 5.6 ) Hypocalcemia: Correct before initiating zoledronic acid injection. Adequately supplement patients with calcium and vitamin D. Monitor serum calcium closely with concomitant administration of other drugs known to cause hypocalcemia to avoid severe or life-threatening hypocalcemia. ( 5.9 ) Zoledronic acid injection can cause fetal harm. Advise females of reproductive potential of potential risk to a fetus and to use effective contraception. ( 5.10 , 8.1 , 8.3 )
Adverse Reactions
The most common adverse events (greater than 25%) were nausea, fatigue, anemia, bone pain, constipation, fever, vomiting, and dyspnea. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Westminster Pharmaceuticals, LLC at 1-844-221-7294 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
In vitro studies indicate that the plasma protein binding of zoledronic acid is low, with the unbound fraction ranging from 60% to 77%. In vitro studies also indicate that zoledronic acid does not inhibit microsomal CYP450 enzymes. In vivo studies showed that zoledronic acid is not metabolized, and is excreted into the urine as the intact drug.
How Supplied
Zoledronic Acid Injection 4 mg/5 mL (0.8 mg/mL) Single-Dose Vial for Dilution Prior to Intravenous Infusion Each 5 mL vial contains 4.264 mg zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection. NDC No. Strength Vial Size 69367-190-50 4 mg per 5 mL (0.8 mg per mL) 5 mL fill in a 5 mL single-dose vial
Storage and Handling
Zoledronic Acid Injection 4 mg/5 mL (0.8 mg/mL) Single-Dose Vial for Dilution Prior to Intravenous Infusion Each 5 mL vial contains 4.264 mg zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection. NDC No. Strength Vial Size 69367-190-50 4 mg per 5 mL (0.8 mg per mL) 5 mL fill in a 5 mL single-dose vial
Description
Warnings and Precautions, Embryo-Fetal Toxicity ( 5.10 ) 12/2018
Medication Information
Warnings and Precautions
Patients being treated with zoledronic acid injection should not be treated with Reclast ® . ( 5.1 ) Adequately rehydrate patients with hypercalcemia of malignancy prior to administration of zoledronic acid injection and monitor electrolytes during treatment. ( 5.2 ) Renal toxicity may be greater in patients with renal impairment. Do not use doses greater than 4 mg. Treatment in patients with severe renal impairment is not recommended. Monitor serum creatinine before each dose. ( 5.3 ) Osteonecrosis of the jaw (ONJ) has been reported. Preventive dental exams should be performed before starting zoledronic acid injection. Avoid invasive dental procedures. ( 5.4 ) Severe incapacitating bone, joint, and/or muscle pain may occur. Discontinue zoledronic acid injection if severe symptoms occur. ( 5.5 ) Atypical subtrochanteric and diaphyseal femoral fractures have been reported in patients receiving bisphosphonate therapy. These fractures may occur after minimal or no trauma. Evaluate patients with thigh or groin pain to rule out a femoral fracture. Consider drug discontinuation in patients suspected to have an atypical femur fracture. ( 5.6 ) Hypocalcemia: Correct before initiating zoledronic acid injection. Adequately supplement patients with calcium and vitamin D. Monitor serum calcium closely with concomitant administration of other drugs known to cause hypocalcemia to avoid severe or life-threatening hypocalcemia. ( 5.9 ) Zoledronic acid injection can cause fetal harm. Advise females of reproductive potential of potential risk to a fetus and to use effective contraception. ( 5.10 , 8.1 , 8.3 )
Indications and Usage
Zoledronic acid injection is a bisphosphonate indicated for the treatment of: Hypercalcemia of malignancy. ( 1.1 ) Patients with multiple myeloma and patients with documented bone metastases from solid tumors, in conjunction with standard antineoplastic therapy. Prostate cancer should have progressed after treatment with at least one hormonal therapy. ( 1.2 ) Limitations of Use: The safety and efficacy of zoledronic acid injection has not been established for use in hyperparathyroidism or non-tumor-related hypercalcemia.
Dosage and Administration
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Contraindications
Hypersensitivity to any component of zoledronic acid injection ( 4 )
Adverse Reactions
The most common adverse events (greater than 25%) were nausea, fatigue, anemia, bone pain, constipation, fever, vomiting, and dyspnea. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Westminster Pharmaceuticals, LLC at 1-844-221-7294 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
In vitro studies indicate that the plasma protein binding of zoledronic acid is low, with the unbound fraction ranging from 60% to 77%. In vitro studies also indicate that zoledronic acid does not inhibit microsomal CYP450 enzymes. In vivo studies showed that zoledronic acid is not metabolized, and is excreted into the urine as the intact drug.
Storage and Handling
Zoledronic Acid Injection 4 mg/5 mL (0.8 mg/mL) Single-Dose Vial for Dilution Prior to Intravenous Infusion Each 5 mL vial contains 4.264 mg zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection. NDC No. Strength Vial Size 69367-190-50 4 mg per 5 mL (0.8 mg per mL) 5 mL fill in a 5 mL single-dose vial
How Supplied
Zoledronic Acid Injection 4 mg/5 mL (0.8 mg/mL) Single-Dose Vial for Dilution Prior to Intravenous Infusion Each 5 mL vial contains 4.264 mg zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection. NDC No. Strength Vial Size 69367-190-50 4 mg per 5 mL (0.8 mg per mL) 5 mL fill in a 5 mL single-dose vial
Description
Warnings and Precautions, Embryo-Fetal Toxicity ( 5.10 ) 12/2018
Section 42229-5
Limitations of Use
The safety and efficacy of zoledronic acid injection in the treatment of hypercalcemia associated with hyperparathyroidism or with other non-tumor-related conditions have not been established.
Section 43683-2
| Warnings and Precautions, Embryo-Fetal Toxicity (5.10) | 12/2018 |
Section 44425-7
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Discard unused portion.
The container closure is not made with natural rubber latex.
10 Overdosage
Clinical experience with acute overdosage of zoledronic acid injection is limited. Two patients received zoledronic acid injection 32 mg over 5 minutes in clinical trials. Neither patient experienced any clinical or laboratory toxicity. Overdosage may cause clinically significant hypocalcemia, hypophosphatemia, and hypomagnesemia. Clinically relevant reductions in serum levels of calcium, phosphorus, and magnesium should be corrected by intravenous administration of calcium gluconate, potassium or sodium phosphate, and magnesium sulfate, respectively.
In an open-label study of zoledronic acid 4 mg in breast cancer patients, a female patient received a single 48-mg dose of zoledronic acid in error. Two days after the overdose, the patient experienced a single episode of hyperthermia (38°C), which resolved after treatment. All other evaluations were normal, and the patient was discharged seven days after the overdose.
A patient with non-Hodgkin's lymphoma received zoledronic acid 4 mg daily on four successive days for a total dose of 16 mg. The patient developed paresthesia and abnormal liver function tests with increased GGT (nearly 100 unit/L, each value unknown). The outcome of this case is not known.
In controlled clinical trials, administration of zoledronic acid injection 4 mg as an intravenous infusion over 5 minutes has been shown to increase the risk of renal toxicity compared to the same dose administered as a 15-minute intravenous infusion. In controlled clinical trials, zoledronic acid injection 8 mg has been shown to be associated with an increased risk of renal toxicity compared to zoledronic acid injection 4 mg, even when given as a 15- minute intravenous infusion, and was not associated with added benefit in patients with hypercalcemia of malignancy [see Dosage and Administration (2.4)].
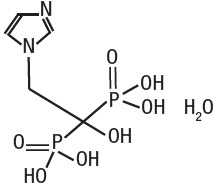
11 Description
Zoledronic acid injection contains zoledronic acid, a bisphosphonic acid which is an inhibitor of osteoclastic bone resorption. Zoledronic acid is designated chemically as (1-Hydroxy-2-imidazol-1-yl-phosphonoethyl) phosphonic acid monohydrate and its structural formula is:
Zoledronic acid is a white crystalline powder. Its molecular formula is C5H10N2O7P2 ∙ H2O and its molar mass is 290.1g/mol. Zoledronic acid is highly soluble in 0.1N sodium hydroxide solution, sparingly soluble in water and 0.1N hydrochloric acid, and practically insoluble in organic solvents. The pH of a 0.7% solution of zoledronic acid in water is approximately 2.0.
Zoledronic acid injection is available in 5 mL vials as a sterile liquid solution for dilution prior to intravenous infusion. Each 5 mL solution for dilution prior to intravenous infusion vial contains 4.264 mg of zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection.
Inactive Ingredients: mannitol, USP, as bulking agent, sodium citrate, USP, as buffering agent, and water for injection.
7.4 Thalidomide
No dose adjustment for zoledronic acid injection 4 mg is needed when coadministered with thalidomide. In a pharmacokinetic study of 24 patients with multiple myeloma, zoledronic acid injection 4 mg given as a 15-minute infusion was administered either alone or with thalidomide (100 mg once daily on days 1-14 and 200 mg once daily on days 15-28). Coadministration of thalidomide with zoledronic acid injection did not significantly change the pharmacokinetics of zoledronic acid or creatinine clearance.
5.9 Hypocalcemia
Hypocalcemia has been reported in patients treated with zoledronic acid injection. Cardiac arrhythmias and neurologic adverse events (seizures, tetany, and numbness) have been reported secondary to cases of severe hypocalcemia. In some instances, hypocalcemia may be life-threatening. Caution is advised when zoledronic acid injection is administered with drugs known to cause hypocalcemia, as severe hypocalcemia may develop, [see Drug Interactions (7)]. Serum calcium should be measured and hypocalcemia must be corrected before initiating zoledronic acid injection. Adequately supplement patients with calcium and vitamin D.
8.4 Pediatric Use
Zoledronic acid injection is not indicated for use in children.
The safety and effectiveness of zoledronic acid was studied in a one-year, active-controlled trial of 152 pediatric subjects (74 receiving zoledronic acid). The enrolled population was subjects with severe osteogenesis imperfecta, aged 1-17 years, 55% male, 84% Caucasian, with a mean lumbar spine bone mineral density (BMD) of 0.431 gm/cm2, which is 2.7 standard deviations below the mean for age-matched controls (BMD Z-score of -2.7). At one year, increases in BMD were observed in the zoledronic acid treatment group. However, changes in BMD in individual patients with severe osteogenesis imperfecta did not necessarily correlate with the risk for fracture or the incidence or severity of chronic bone pain. The adverse events observed with zoledronic acid injection use in children did not raise any new safety findings beyond those previously seen in adults treated for hypercalcemia of malignancy or bone metastases. However, adverse reactions seen more commonly in pediatric patients included pyrexia (61%), arthralgia (26%), hypocalcemia (22%) and headache (22%). These reactions, excluding arthralgia, occurred most frequently within 3 days after the first infusion and became less common with repeat dosing. Because of long-term retention in bone, zoledronic acid injection should only be used in children if the potential benefit outweighs the potential risk.
Plasma zoledronic acid concentration data was obtained from 10 patients with severe osteogenesis imperfecta (4 in the age group of 3-8 years and 6 in the age group of 9-17 years) infused with 0.05 mg/kg dose over 30 min. Mean Cmax and AUC(0-last) was 167 ng/mL and 220 ng.h/mL, respectively. The plasma concentration time profile of zoledronic acid in pediatric patients represent a multi-exponential decline, as observed in adult cancer patients at an approximately equivalent mg/kg dose.
8.5 Geriatric Use
Clinical studies of zoledronic acid injection in hypercalcemia of malignancy included 34 patients who were 65 years of age or older. No significant differences in response rate or adverse reactions were seen in geriatric patients receiving zoledronic acid injection as compared to younger patients. Controlled clinical studies of zoledronic acid injection in the treatment of multiple myeloma and bone metastases of solid tumors in patients over age 65 revealed similar efficacy and safety in older and younger patients. Because decreased renal function occurs more commonly in the elderly, special care should be taken to monitor renal function.
7.2 Loop Diuretics
Caution should also be exercised when zoledronic acid injection is used in combination with loop diuretics due to an increased risk of hypocalcemia.
4 Contraindications
Hypersensitivity to any component of zoledronic acid injection (4)
6 Adverse Reactions
The most common adverse events (greater than 25%) were nausea, fatigue, anemia, bone pain, constipation, fever, vomiting, and dyspnea. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Westminster Pharmaceuticals, LLC at 1-844-221-7294 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions
In vitro studies indicate that the plasma protein binding of zoledronic acid is low, with the unbound fraction ranging from 60% to 77%. In vitro studies also indicate that zoledronic acid does not inhibit microsomal CYP450 enzymes. In vivo studies showed that zoledronic acid is not metabolized, and is excreted into the urine as the intact drug.
5.3 Renal Impairment
Zoledronic acid injection is excreted intact primarily via the kidney, and the risk of adverse reactions, in particular renal adverse reactions, may be greater in patients with impaired renal function. Safety and pharmacokinetic data are limited in patients with severe renal impairment and the risk of renal deterioration is increased [see Adverse Reactions (6.1)]. Preexisting renal insufficiency and multiple cycles of zoledronic acid injection and other bisphosphonates are risk factors for subsequent renal deterioration with zoledronic acid injection. Factors predisposing to renal deterioration, such as dehydration or the use of other nephrotoxic drugs, should be identified and managed, if possible.
Zoledronic acid injection treatment in patients with hypercalcemia of malignancy with severe renal impairment should be considered only after evaluating the risks and benefits of treatment [see Dosage and Administration (2.1)]. In the clinical studies, patients with serum creatinine greater than 400 µmol/L or greater than 4.5 mg/dL were excluded.
Zoledronic acid injection treatment is not recommended in patients with bone metastases with severe renal impairment. In the clinical studies, patients with serum creatinine greater than 265 µmol/L or greater than 3.0 mg/dL were excluded and there were only 8 of 564 patients treated with zoledronic acid injection 4 mg by 15-minute infusion with a baseline creatinine greater than 2 mg/dL. Limited pharmacokinetic data exists in patients with creatinine clearance less than 30 mL/min [see Clinical Pharmacology (12.3)].
12.2 Pharmacodynamics
Clinical studies in patients with hypercalcemia of malignancy (HCM) showed that single-dose infusions of zoledronic acid injection are associated with decreases in serum calcium and phosphorus and increases in urinary calcium and phosphorus excretion.
Osteoclastic hyperactivity resulting in excessive bone resorption is the underlying pathophysiologic derangement in hypercalcemia of malignancy (HCM, tumor-induced hypercalcemia) and metastatic bone disease. Excessive release of calcium into the blood as bone is resorbed results in polyuria and gastrointestinal disturbances, with progressive dehydration and decreasing glomerular filtration rate. This, in turn, results in increased renal resorption of calcium, setting up a cycle of worsening systemic hypercalcemia. Reducing excessive bone resorption and maintaining adequate fluid administration are, therefore, essential to the management of hypercalcemia of malignancy.
Patients who have hypercalcemia of malignancy can generally be divided into two groups according to the pathophysiologic mechanism involved: humoral hypercalcemia and hypercalcemia due to tumor invasion of bone. In humoral hypercalcemia, osteoclasts are activated and bone resorption is stimulated by factors such as parathyroid hormone-related protein, which are elaborated by the tumor and circulate systemically. Humoral hypercalcemia usually occurs in squamous cell malignancies of the lung or head and neck or in genitourinary tumors such as renal cell carcinoma or ovarian cancer. Skeletal metastases may be absent or minimal in these patients.
Extensive invasion of bone by tumor cells can also result in hypercalcemia due to local tumor products that stimulate bone resorption by osteoclasts. Tumors commonly associated with locally mediated hypercalcemia include breast cancer and multiple myeloma.
Total serum calcium levels in patients who have hypercalcemia of malignancy may not reflect the severity of hypercalcemia, since concomitant hypoalbuminemia is commonly present. Ideally, ionized calcium levels should be used to diagnose and follow hypercalcemic conditions; however, these are not commonly or rapidly available in many clinical situations. Therefore, adjustment of the total serum calcium value for differences in albumin levels (corrected serum calcium, CSC) is often used in place of measurement of ionized calcium; several nomograms are in use for this type of calculation [see Dosage and Administration (2.1)].
12.3 Pharmacokinetics
Pharmacokinetic data in patients with hypercalcemia are not available.
7.3 Nephrotoxic Drugs
Caution is indicated when zoledronic acid injection is used with other potentially nephrotoxic drugs.
5.8 Hepatic Impairment
Only limited clinical data are available for use of zoledronic acid injection to treat hypercalcemia of malignancy in patients with hepatic insufficiency, and these data are not adequate to provide guidance on dosage selection or how to safely use zoledronic acid injection in these patients.
1 Indications and Usage
Zoledronic acid injection is a bisphosphonate indicated for the treatment of:
- Hypercalcemia of malignancy. (1.1)
- Patients with multiple myeloma and patients with documented bone metastases from solid tumors, in conjunction with standard antineoplastic therapy. Prostate cancer should have progressed after treatment with at least one hormonal therapy. (1.2)
Limitations of Use: The safety and efficacy of zoledronic acid injection has not been established for use in hyperparathyroidism or non-tumor-related hypercalcemia.
12.1 Mechanism of Action
The principal pharmacologic action of zoledronic acid is inhibition of bone resorption. Although the antiresorptive mechanism is not completely understood, several factors are thought to contribute to this action. In vitro, zoledronic acid inhibits osteoclastic activity and induces osteoclast apoptosis. Zoledronic acid also blocks the osteoclastic resorption of mineralized bone and cartilage through its binding to bone. Zoledronic acid inhibits the increased osteoclastic activity and skeletal calcium release induced by various stimulatory factors released by tumors.
5.5 Musculoskeletal Pain
In postmarketing experience, severe and occasionally incapacitating bone, joint, and/or muscle pain has been reported in patients taking bisphosphonates, including zoledronic acid injection. The time to onset of symptoms varied from one day to several months after starting the drug. Discontinue use if severe symptoms develop. Most patients had relief of symptoms after stopping. A subset had recurrence of symptoms when rechallenged with the same drug or another bisphosphonate [see Adverse Reactions (6.2)].
5.7 Patients With Asthma
While not observed in clinical trials with zoledronic acid injection, there have been reports of bronchoconstriction in aspirin-sensitive patients receiving bisphosphonates.
5 Warnings and Precautions
- Patients being treated with zoledronic acid injection should not be treated with Reclast®. (5.1)
- Adequately rehydrate patients with hypercalcemia of malignancy prior to administration of zoledronic acid injection and monitor electrolytes during treatment. (5.2)
- Renal toxicity may be greater in patients with renal impairment. Do not use doses greater than 4 mg. Treatment in patients with severe renal impairment is not recommended. Monitor serum creatinine before each dose. (5.3)
- Osteonecrosis of the jaw (ONJ) has been reported. Preventive dental exams should be performed before starting zoledronic acid injection. Avoid invasive dental procedures. (5.4)
- Severe incapacitating bone, joint, and/or muscle pain may occur. Discontinue zoledronic acid injection if severe symptoms occur. (5.5)
- Atypical subtrochanteric and diaphyseal femoral fractures have been reported in patients receiving bisphosphonate therapy. These fractures may occur after minimal or no trauma. Evaluate patients with thigh or groin pain to rule out a femoral fracture. Consider drug discontinuation in patients suspected to have an atypical femur fracture. (5.6)
- Hypocalcemia: Correct before initiating zoledronic acid injection. Adequately supplement patients with calcium and vitamin D. Monitor serum calcium closely with concomitant administration of other drugs known to cause hypocalcemia to avoid severe or life-threatening hypocalcemia. (5.9)
- Zoledronic acid injection can cause fetal harm. Advise females of reproductive potential of potential risk to a fetus and to use effective contraception. (5.10, 8.1, 8.3)
5.10 Embryo Fetal Toxicity
Based on findings from animal studies and its mechanism of action, zoledronic acid injection can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, administration of zoledronic acid to pregnant rats during organogenesis resulted in fetal malformations and embryo-fetal lethality at maternal exposures that were greater than or equal to 2.4 times the human clinical exposure based on area under the curve (AUC). Bisphosphonates, such as zoledronic acid, are incorporated into the bone matrix, from where they are gradually released over periods of weeks to years. There may be a risk of fetal harm (e.g., skeletal and other abnormalities) if a woman becomes pregnant after completing a course of bisphosphonate therapy. Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during and after zoledronic acid injection treatment [see Use in Specific Populations (8.1, 8.3), Clinical Pharmacology (12.1)].
2 Dosage and Administration
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
2.3 Preparation of Solution
Zoledronic acid injection must not be mixed with calcium or other divalent cation-containing infusion solutions, such as Lactated Ringer's solution, and should be administered as a single intravenous solution in a line separate from all other drugs.
2.4 Method of Administration
Due to the risk of clinically significant deterioration in renal function, which may progress to renal failure, single doses of zoledronic acid injection should not exceed 4 mg and the duration of infusion should be no less than 15 minutes [see Warnings and Precautions (5.3)]. In the trials and in postmarketing experience, renal deterioration, progression to renal failure and dialysis, have occurred in patients, including those treated with the approved dose of 4 mg infused over 15 minutes. There have been instances of this occurring after the initial zoledronic acid injection dose.
3 Dosage Forms and Strengths
Injection: 4 mg/5 mL (0.8 mg/mL) single-dose vial for dilution prior to intravenous infusion.
5.4 Osteonecrosis of the Jaw
Osteonecrosis of the jaw (ONJ) has been reported predominantly in cancer patients treated with intravenous bisphosphonates, including zoledronic acid injection. Many of these patients were also receiving chemotherapy and corticosteroids which may be risk factors for ONJ. The risk of ONJ may increase with duration of exposure to bisphosphonates.
Postmarketing experience and the literature suggest a greater frequency of reports of ONJ based on tumor type (advanced breast cancer, multiple myeloma), and dental status (dental extraction, periodontal disease, local trauma including poorly fitting dentures). Many reports of ONJ involved patients with signs of local infection including osteomyelitis.
Cancer patients should maintain good oral hygiene and should have a dental examination with preventive dentistry prior to treatment with bisphosphonates.
While on treatment, these patients should avoid invasive dental procedures if possible. For patients who develop ONJ while on bisphosphonate therapy, dental surgery may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ. Clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment [see Adverse Reactions (6.2)].
6.2 Postmarketing Experience
The following adverse reactions have been reported during postapproval use of zoledronic acid injection. Because these reports are from a population of uncertain size and are subject to confounding factors, it is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 Use in Specific Populations
- Lactation: Advise not to breastfeed. (8.2)
- Females and Males of Reproductive Potential: Verify pregnancy status prior to initiation of zoledronic acid injection. May impair fertility. Counsel patients on pregnancy planning and prevention. (8.3)
- Pediatric Use: Not indicated for use in pediatric patients. (8.4)
- Geriatric Use: Special care to monitor renal function. (8.5)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
1.1 Hypercalcemia of Malignancy
Zoledronic acid injection is indicated for the treatment of hypercalcemia of malignancy defined as an albumin-corrected calcium (cCa) of greater than or equal to 12 mg/dL [3.0 mmol/L] using the formula: cCa in mg/dL = Ca in mg/dL + 0.8 (4.0 g/dL - patient albumin [g/dL]).
2.1 Hypercalcemia of Malignancy
The maximum recommended dose of zoledronic acid injection in hypercalcemia of malignancy (albumin-corrected serum calcium greater than or equal to 12 mg/dL [3.0 mmol/L]) is 4 mg. The 4-mg dose must be given as a single-dose intravenous infusion over no less than 15 minutes. Patients who receive zoledronic acid injection should have serum creatinine assessed prior to each treatment.
Dose adjustments of zoledronic acid injection are not necessary in treating patients for hypercalcemia of malignancy presenting with mild-to-moderate renal impairment prior to initiation of therapy (serum creatinine less than 400 µmol/L or less than 4.5 mg/dL).
Patients should be adequately rehydrated prior to administration of zoledronic acid injection [see Warnings and Precautions (5.2)].
Consideration should be given to the severity of, as well as the symptoms of, tumor-induced hypercalcemia when considering use of zoledronic acid injection. Vigorous saline hydration, an integral part of hypercalcemia therapy, should be initiated promptly and an attempt should be made to restore the urine output to about 2 L/day throughout treatment. Mild or asymptomatic hypercalcemia may be treated with conservative measures (i.e., saline hydration, with or without loop diuretics). Patients should be hydrated adequately throughout the treatment, but overhydration, especially in those patients who have cardiac failure, must be avoided. Diuretic therapy should not be employed prior to correction of hypovolemia.
Retreatment with zoledronic acid injection 4 mg may be considered if serum calcium does not return to normal or remain normal after initial treatment. It is recommended that a minimum of 7 days elapse before retreatment, to allow for full response to the initial dose. Renal function must be carefully monitored in all patients receiving zoledronic acid injection and serum creatinine must be assessed prior to retreatment with zoledronic acid injection [see Warnings and Precautions (5.2)].
14.1 Hypercalcemia of Malignancy
Two identical multicenter, randomized, double-blind, double-dummy studies of zoledronic acid injection 4 mg given as a 5-minute intravenous infusion or pamidronate 90 mg given as a 2-hour intravenous infusion were conducted in 185 patients with hypercalcemia of malignancy (HCM). NOTE: Administration of zoledronic acid injection 4 mg given as a 5-minute intravenous infusion has been shown to result in an increased risk of renal toxicity, as measured by increases in serum creatinine, which can progress to renal failure. The incidence of renal toxicity and renal failure has been shown to be reduced when zoledronic acid injection 4 mg is given as a 15-minute intravenous infusion. Zoledronic acid injection should be administered by intravenous infusion over no less than 15 minutes [see Warnings and Precautions (5.1, 5.2), Dosage and Administration (2.4)]. The treatment groups in the clinical studies were generally well balanced with regards to age, sex, race, and tumor types. The mean age of the study population was 59 years; 81% were Caucasian, 15% were Black, and 4% were of other races. Sixty percent (60%) of the patients were male. The most common tumor types were lung, breast, head and neck, and renal.
In these studies, HCM was defined as a corrected serum calcium (CSC) concentration of greater than or equal to 12.0 mg/dL (3.00 mmol/L). The primary efficacy variable was the proportion of patients having a complete response, defined as the lowering of the CSC to less than or equal to 10.8 mg/dL (2.70 mmol/L) within 10 days after drug infusion.
To assess the effects of zoledronic acid injection versus those of pamidronate, the two multi-center HCM studies were combined in a preplanned analysis. The results of the primary analysis revealed that the proportion of patients that had normalization of corrected serum calcium by Day 10 were 88% and 70% for zoledronic acid injection 4 mg and pamidronate 90 mg, respectively (P=0.002) (see Figure 1). In these studies, no additional benefit was seen for zoledronic acid injection 8 mg over zoledronic acid injection 4 mg; however, the risk of renal toxicity of zoledronic acid injection 8 mg was significantly greater than that seen with zoledronic acid injection 4 mg.
Secondary efficacy variables from the pooled HCM studies included the proportion of patients who had normalization of corrected serum calcium (CSC) by Day 4; the proportion of patients who had normalization of CSC by Day 7; time to relapse of HCM; and duration of complete response. Time to relapse of HCM was defined as the duration (in days) of normalization of serum calcium from study drug infusion until the last CSC value less than 11.6 mg/dL (less than 2.90 mmol/L). Patients who did not have a complete response were assigned a time to relapse of 0 days. Duration of complete response was defined as the duration (in days) from the occurrence of a complete response until the last CSC less than or equal to 10.8 mg/dL (2.70 mmol/L). The results of these secondary analyses for zoledronic acid injection 4 mg and pamidronate 90 mg are shown in Table 11.
| Zoledronic Acid Injection 4 mg | Pamidronate 90 mg | |||
|---|---|---|---|---|
| Complete Response | N | Response Rate | N | Response Rate |
| By Day 4 | 86 | 45.3% | 99 | 33.3% |
| By Day 7 | 86 | 82.6% P less than 0.05 versus pamidronate 90 mg.
|
99 | 63.6% |
| Duration of Response | N | Median Duration (Days) | N | Median Duration (Days) |
| Time to Relapse | 86 | 30 | 99 | 17 |
| Duration of Complete Response | 76 | 32 | 69 | 18 |
7.1 Aminoglycosides and Calcitonin
Caution is advised when bisphosphonates are administered with aminoglycosides or calcitonin, since these agents may have an additive effect to lower serum calcium level for prolonged periods. This effect has not been reported in zoledronic acid injection clinical trials.
16 How Supplied/storage and Handling
Zoledronic Acid Injection 4 mg/5 mL (0.8 mg/mL) Single-Dose Vial for Dilution Prior to Intravenous Infusion
Each 5 mL vial contains 4.264 mg zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection.
| NDC No. | Strength | Vial Size |
|---|---|---|
| 69367-190-50 | 4 mg per 5 mL (0.8 mg per mL) |
5 mL fill in a 5 mL single-dose vial |
5.2 Hydration and Electrolyte Monitoring
Patients with hypercalcemia of malignancy must be adequately rehydrated prior to administration of zoledronic acid injection. Loop diuretics should not be used until the patient is adequately rehydrated and should be used with caution in combination with zoledronic acid injection in order to avoid hypocalcemia. Zoledronic acid injection should be used with caution with other nephrotoxic drugs.
Standard hypercalcemia-related metabolic parameters, such as serum levels of calcium, phosphate, and magnesium, as well as serum creatinine, should be carefully monitored following initiation of therapy with zoledronic acid injection. If hypocalcemia, hypophosphatemia, or hypomagnesemia occur, short-term supplemental therapy may be necessary.
Principal Display Panel 5 Ml Vial Carton
NDC 69367-190-50
Rx only
Zoledronic Acid
Injection
4 mg per 5 mL
(0.8 mg per mL)
For Intravenous Infusion after Dilution
Sterile
Not for direct injection.
DOSE MUST BE DILUTED.
Do not mix with calcium-containing
infusion solutions.
One 5 mL Single-Dose Vial
Westminster
Pharmaceuticals
1.2 Multiple Myeloma and Bone Metastases of Solid Tumors
Zoledronic acid injection is indicated for the treatment of patients with multiple myeloma and patients with documented bone metastases from solid tumors, in conjunction with standard antineoplastic therapy. Prostate cancer should have progressed after treatment with at least one hormonal therapy.
2.2 Multiple Myeloma and Bone Metastases of Solid Tumors
The recommended dose of zoledronic acid injection in patients with multiple myeloma and metastatic bone lesions from solid tumors for patients with creatinine clearance (CrCl) greater than 60 mL/min is 4 mg infused over no less than 15 minutes every 3 to 4 weeks. The optimal duration of therapy is not known.
Upon treatment initiation, the recommended zoledronic acid injection doses for patients with reduced renal function (mild and moderate renal impairment) are listed in Table 1. These doses are calculated to achieve the same area under the curve (AUC) as that achieved in patients with creatinine clearance of 75 mL/min. CrCl is calculated using the Cockcroft-Gault formula [see Warnings and Precautions (5.2)].
| Baseline Creatinine Clearance (mL/min) |
Zoledronic Acid Injection Recommended Dose (mg) Doses calculated assuming target AUC of 0.66 (mg∙hr/L) (CrCl = 75 mL/min)
|
|---|---|
| greater than 60 | 4 |
| 50-60 | 3.5 |
| 40-49 | 3.3 |
| 30-39 | 3 |
During treatment, serum creatinine should be measured before each zoledronic acid injection dose and treatment should be withheld for renal deterioration. In the clinical studies, renal deterioration was defined as follows:
-
For patients with normal baseline creatinine, increase of 0.5 mg/dL
-
For patients with abnormal baseline creatinine, increase of 1.0 mg/dL
In the clinical studies, zoledronic acid injection treatment was resumed only when the creatinine returned to within 10% of the baseline value. Zoledronic acid injection should be reinitiated at the same dose as that prior to treatment interruption.
Patients should also be administered an oral calcium supplement of 500 mg and a multiple vitamin containing 400 international units of vitamin D daily.
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Standard lifetime carcinogenicity bioassays were conducted in mice and rats. Mice were given oral doses of zoledronic acid of 0.1, 0.5, or 2.0 mg/kg/day. There was an increased incidence of Harderian gland adenomas in males and females in all treatment groups (at doses greater than or equal to 0.002 times a human intravenous dose of 4 mg, based on a comparison of relative body surface areas). Rats were given oral doses of zoledronic acid of 0.1, 0.5, or 2.0 mg/kg/day. No increased incidence of tumors was observed (at doses less than or equal to 0.2 times the human intravenous dose of 4 mg, based on a comparison of relative body surface areas).
Zoledronic acid was not genotoxic in the Ames bacterial mutagenicity assay, in the Chinese hamster ovary cell assay, or in the Chinese hamster gene mutation assay, with or without metabolic activation. Zoledronic acid was not genotoxic in the in vivo rat micronucleus assay.
Female rats were given subcutaneous doses of zoledronic acid of 0.01, 0.03, or 0.1 mg/kg/day beginning 15 days before mating and continuing through gestation. Effects observed in the high-dose group (with systemic exposure of 1.2 times the human systemic exposure following an intravenous dose of 4 mg, based on AUC comparison) included inhibition of ovulation and a decrease in the number of pregnant rats. Effects observed in both the mid-dose group (with systemic exposure of 0.2 times the human systemic exposure following an intravenous dose of 4 mg, based on an AUC comparison) and high-dose group included an increase in preimplantation losses and a decrease in the number of implantations and live fetuses.
5.6 Atypical Subtrochanteric and Diaphyseal Femoral Fractures
Atypical subtrochanteric and diaphyseal femoral fractures have been reported in patients receiving bisphosphonate therapy, including zoledronic acid injection. These fractures can occur anywhere in the femoral shaft from just below the lesser trochanter to just above the supracondylar flare and are transverse or short oblique in orientation without evidence of comminution. These fractures occur after minimal or no trauma. Patients may experience thigh or groin pain weeks to months before presenting with a completed femoral fracture. Fractures are often bilateral; therefore the contralateral femur should be examined in bisphosphonate-treated patients who have sustained a femoral shaft fracture. Poor healing of these fractures has also been reported. A number of case reports noted that patients were also receiving treatment with glucocorticoids (such as prednisone or dexamethasone) at the time of fracture. Causality with bisphosphonate therapy has not been established.
Any patient with a history of bisphosphonate exposure who presents with thigh or groin pain in the absence of trauma should be suspected of having an atypical fracture and should be evaluated. Discontinuation of zoledronic acid injection therapy in patients suspected to have an atypical femur fracture should be considered pending evaluation of the patient, based on an individual benefit risk assessment. It is unknown whether the risk of atypical femur fracture continues after stopping therapy.
5.1 Drugs With Same Active Ingredient Or in the Same Drug Class
Zoledronic acid injection contains the same active ingredient as found in Reclast® (zoledronic acid). Patients being treated with zoledronic acid injection should not be treated with Reclast or other bisphosphonates.
14.2 Clinical Trials in Multiple Myeloma and Bone Metastases of Solid Tumors
Table 12 describes an overview of the efficacy population in three randomized zoledronic acid injection trials in patients with multiple myeloma and bone metastases of solid tumors. These trials included a pamidronate-controlled study in breast cancer and multiple myeloma, a placebo-controlled study in prostate cancer, and a placebo-controlled study in other solid tumors. The prostate cancer study required documentation of previous bone metastases and 3 consecutive rising PSAs while on hormonal therapy. The other placebo-controlled solid tumor study included patients with bone metastases from malignancies other than breast cancer and prostate cancer, including NSCLC, renal cell cancer, small cell lung cancer, colorectal cancer, bladder cancer, GI/genitourinary cancer, head and neck cancer, and others. These trials were comprised of a core phase and an extension phase. In the solid tumor, breast cancer and multiple myeloma trials, only the core phase was evaluated for efficacy as a high percentage of patients did not choose to participate in the extension phase. In the prostate cancer trials, both the core and extension phases were evaluated for efficacy showing the zoledronic acid injection effect during the first 15 months was maintained without decrement or improvement for another 9 months. The design of these clinical trials does not permit assessment of whether more than one-year administration of zoledronic acid injection is beneficial. The optimal duration of zoledronic acid injection administration is not known.
The studies were amended twice because of renal toxicity. The zoledronic acid injection infusion duration was increased from 5 minutes to 15 minutes. After all patients had been accrued, but while dosing and follow-up continued, patients in the 8 mg zoledronic acid injection treatment arm were switched to 4 mg due to toxicity. Patients who were randomized to the zoledronic acid injection 8 mg group are not included in these analyses.
| Patient Population | No. of Patients | Zoledronic Acid Injection Dose | Control | Median Duration (Planned Duration) Zoledronic Acid Injection 4 mg |
|---|---|---|---|---|
| Multiple myeloma or metastatic breast cancer | 1,648 | 4 and 8 Patients who were randomized to the 8 mg zoledronic acid injection group are not included in any of the analyses in this package insert. mg Q3-4 weeks |
Pamidronate 90 mg Q3-4 weeks | 12.0 months (13 months) |
| Metastatic prostate cancer | 643 | 4 and 8 mg Q3 weeks | Placebo | 10.5 months (15 months) |
| Metastatic solid tumor other than breast or prostate cancer | 773 | 4 and 8 mg Q3 weeks | Placebo | 3.8 months (9 months) |
Each study evaluated skeletal-related events (SREs), defined as any of the following: pathologic fracture, radiation therapy to bone, surgery to bone, or spinal cord compression. Change in antineoplastic therapy due to increased pain was a SRE in the prostate cancer study only. Planned analyses included the proportion of patients with a SRE during the study and time to the first SRE. Results for the two zoledronic acid injection placebo-controlled studies are given in Table 13.
| I. Analysis of Proportion of Patients with a SRE SRE=Skeletal-Related Event.
|
II. Analysis of Time to the First SRE | ||||||
|---|---|---|---|---|---|---|---|
| Study | Study Arm & Patient Number | Proportion | Difference Difference for the proportion of patients with a SRE of zoledronic acid injection 4 mg versus placebo. & 95% CI |
P-value | Median (Days) | Hazard Ratio Hazard ratio for the first occurrence of a SRE of zoledronic acid injection 4 mg versus placebo. & 95% CI |
P-value |
| Prostate Cancer | Zoledronic Acid Injection 4 mg (n=214) |
33% | -11% (-20%, -1%) |
0.02 | Not Reached | 0.67 (0.49, 0.91) |
0.011 |
| Placebo (n=208) |
44% | 321 | |||||
| Solid Tumors | Zoledronic Acid Injection 4 mg (n=257) |
38% | -7% (-15%, 2%) |
0.13 | 230 | 0.73 (0.55, 0.96) |
0.023 |
| Placebo (n=250) |
44% | 163 |
In the breast cancer and myeloma trial, efficacy was determined by a noninferiority analysis comparing zoledronic acid injection to pamidronate 90 mg for the proportion of patients with a SRE. This analysis required an estimation of pamidronate efficacy. Historical data from 1,128 patients in three pamidronate placebo-controlled trials demonstrated that pamidronate decreased the proportion of patients with a SRE by 13.1% (95% CI = 7.3%, 18.9%). Results of the comparison of treatment with zoledronic acid injection compared to pamidronate are given in Table 14.
| I. Analysis of Proportion of Patients with a SRE SRE=Skeletal-Related Event.
|
II. Analysis of Time to the First SRE | ||||||
|---|---|---|---|---|---|---|---|
| Study | Study Arm & Patient Number | Proportion | Difference Difference for the proportion of patients with a SRE of zoledronic acid injection 4 mg versus pamidronate 90 mg. & 95% CI |
P-value | Median (Days) | Hazard Ratio Hazard ratio for the first occurrence of a SRE of zoledronic acid injection 4 mg versus pamidronate 90 mg. & 95% CI |
P-value |
| Multiple Myeloma & Breast Cancer | Zoledronic Acid Injection 4 mg (n=561) |
44% | -2% (-7.9%, 3.7%) |
0.46 | 373 | 0.92 (0.77, 1.09) |
0.32 |
| Pamidronate (n=555) |
46% | 363 |
Structured Label Content
Section 42229-5 (42229-5)
Limitations of Use
The safety and efficacy of zoledronic acid injection in the treatment of hypercalcemia associated with hyperparathyroidism or with other non-tumor-related conditions have not been established.
Section 43683-2 (43683-2)
| Warnings and Precautions, Embryo-Fetal Toxicity (5.10) | 12/2018 |
Section 44425-7 (44425-7)
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Discard unused portion.
The container closure is not made with natural rubber latex.
10 Overdosage (10 OVERDOSAGE)
Clinical experience with acute overdosage of zoledronic acid injection is limited. Two patients received zoledronic acid injection 32 mg over 5 minutes in clinical trials. Neither patient experienced any clinical or laboratory toxicity. Overdosage may cause clinically significant hypocalcemia, hypophosphatemia, and hypomagnesemia. Clinically relevant reductions in serum levels of calcium, phosphorus, and magnesium should be corrected by intravenous administration of calcium gluconate, potassium or sodium phosphate, and magnesium sulfate, respectively.
In an open-label study of zoledronic acid 4 mg in breast cancer patients, a female patient received a single 48-mg dose of zoledronic acid in error. Two days after the overdose, the patient experienced a single episode of hyperthermia (38°C), which resolved after treatment. All other evaluations were normal, and the patient was discharged seven days after the overdose.
A patient with non-Hodgkin's lymphoma received zoledronic acid 4 mg daily on four successive days for a total dose of 16 mg. The patient developed paresthesia and abnormal liver function tests with increased GGT (nearly 100 unit/L, each value unknown). The outcome of this case is not known.
In controlled clinical trials, administration of zoledronic acid injection 4 mg as an intravenous infusion over 5 minutes has been shown to increase the risk of renal toxicity compared to the same dose administered as a 15-minute intravenous infusion. In controlled clinical trials, zoledronic acid injection 8 mg has been shown to be associated with an increased risk of renal toxicity compared to zoledronic acid injection 4 mg, even when given as a 15- minute intravenous infusion, and was not associated with added benefit in patients with hypercalcemia of malignancy [see Dosage and Administration (2.4)].
11 Description (11 DESCRIPTION)
Zoledronic acid injection contains zoledronic acid, a bisphosphonic acid which is an inhibitor of osteoclastic bone resorption. Zoledronic acid is designated chemically as (1-Hydroxy-2-imidazol-1-yl-phosphonoethyl) phosphonic acid monohydrate and its structural formula is:
Zoledronic acid is a white crystalline powder. Its molecular formula is C5H10N2O7P2 ∙ H2O and its molar mass is 290.1g/mol. Zoledronic acid is highly soluble in 0.1N sodium hydroxide solution, sparingly soluble in water and 0.1N hydrochloric acid, and practically insoluble in organic solvents. The pH of a 0.7% solution of zoledronic acid in water is approximately 2.0.
Zoledronic acid injection is available in 5 mL vials as a sterile liquid solution for dilution prior to intravenous infusion. Each 5 mL solution for dilution prior to intravenous infusion vial contains 4.264 mg of zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection.
Inactive Ingredients: mannitol, USP, as bulking agent, sodium citrate, USP, as buffering agent, and water for injection.
7.4 Thalidomide
No dose adjustment for zoledronic acid injection 4 mg is needed when coadministered with thalidomide. In a pharmacokinetic study of 24 patients with multiple myeloma, zoledronic acid injection 4 mg given as a 15-minute infusion was administered either alone or with thalidomide (100 mg once daily on days 1-14 and 200 mg once daily on days 15-28). Coadministration of thalidomide with zoledronic acid injection did not significantly change the pharmacokinetics of zoledronic acid or creatinine clearance.
5.9 Hypocalcemia
Hypocalcemia has been reported in patients treated with zoledronic acid injection. Cardiac arrhythmias and neurologic adverse events (seizures, tetany, and numbness) have been reported secondary to cases of severe hypocalcemia. In some instances, hypocalcemia may be life-threatening. Caution is advised when zoledronic acid injection is administered with drugs known to cause hypocalcemia, as severe hypocalcemia may develop, [see Drug Interactions (7)]. Serum calcium should be measured and hypocalcemia must be corrected before initiating zoledronic acid injection. Adequately supplement patients with calcium and vitamin D.
8.4 Pediatric Use
Zoledronic acid injection is not indicated for use in children.
The safety and effectiveness of zoledronic acid was studied in a one-year, active-controlled trial of 152 pediatric subjects (74 receiving zoledronic acid). The enrolled population was subjects with severe osteogenesis imperfecta, aged 1-17 years, 55% male, 84% Caucasian, with a mean lumbar spine bone mineral density (BMD) of 0.431 gm/cm2, which is 2.7 standard deviations below the mean for age-matched controls (BMD Z-score of -2.7). At one year, increases in BMD were observed in the zoledronic acid treatment group. However, changes in BMD in individual patients with severe osteogenesis imperfecta did not necessarily correlate with the risk for fracture or the incidence or severity of chronic bone pain. The adverse events observed with zoledronic acid injection use in children did not raise any new safety findings beyond those previously seen in adults treated for hypercalcemia of malignancy or bone metastases. However, adverse reactions seen more commonly in pediatric patients included pyrexia (61%), arthralgia (26%), hypocalcemia (22%) and headache (22%). These reactions, excluding arthralgia, occurred most frequently within 3 days after the first infusion and became less common with repeat dosing. Because of long-term retention in bone, zoledronic acid injection should only be used in children if the potential benefit outweighs the potential risk.
Plasma zoledronic acid concentration data was obtained from 10 patients with severe osteogenesis imperfecta (4 in the age group of 3-8 years and 6 in the age group of 9-17 years) infused with 0.05 mg/kg dose over 30 min. Mean Cmax and AUC(0-last) was 167 ng/mL and 220 ng.h/mL, respectively. The plasma concentration time profile of zoledronic acid in pediatric patients represent a multi-exponential decline, as observed in adult cancer patients at an approximately equivalent mg/kg dose.
8.5 Geriatric Use
Clinical studies of zoledronic acid injection in hypercalcemia of malignancy included 34 patients who were 65 years of age or older. No significant differences in response rate or adverse reactions were seen in geriatric patients receiving zoledronic acid injection as compared to younger patients. Controlled clinical studies of zoledronic acid injection in the treatment of multiple myeloma and bone metastases of solid tumors in patients over age 65 revealed similar efficacy and safety in older and younger patients. Because decreased renal function occurs more commonly in the elderly, special care should be taken to monitor renal function.
7.2 Loop Diuretics
Caution should also be exercised when zoledronic acid injection is used in combination with loop diuretics due to an increased risk of hypocalcemia.
4 Contraindications (4 CONTRAINDICATIONS)
Hypersensitivity to any component of zoledronic acid injection (4)
6 Adverse Reactions (6 ADVERSE REACTIONS)
The most common adverse events (greater than 25%) were nausea, fatigue, anemia, bone pain, constipation, fever, vomiting, and dyspnea. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Westminster Pharmaceuticals, LLC at 1-844-221-7294 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions (7 DRUG INTERACTIONS)
In vitro studies indicate that the plasma protein binding of zoledronic acid is low, with the unbound fraction ranging from 60% to 77%. In vitro studies also indicate that zoledronic acid does not inhibit microsomal CYP450 enzymes. In vivo studies showed that zoledronic acid is not metabolized, and is excreted into the urine as the intact drug.
5.3 Renal Impairment
Zoledronic acid injection is excreted intact primarily via the kidney, and the risk of adverse reactions, in particular renal adverse reactions, may be greater in patients with impaired renal function. Safety and pharmacokinetic data are limited in patients with severe renal impairment and the risk of renal deterioration is increased [see Adverse Reactions (6.1)]. Preexisting renal insufficiency and multiple cycles of zoledronic acid injection and other bisphosphonates are risk factors for subsequent renal deterioration with zoledronic acid injection. Factors predisposing to renal deterioration, such as dehydration or the use of other nephrotoxic drugs, should be identified and managed, if possible.
Zoledronic acid injection treatment in patients with hypercalcemia of malignancy with severe renal impairment should be considered only after evaluating the risks and benefits of treatment [see Dosage and Administration (2.1)]. In the clinical studies, patients with serum creatinine greater than 400 µmol/L or greater than 4.5 mg/dL were excluded.
Zoledronic acid injection treatment is not recommended in patients with bone metastases with severe renal impairment. In the clinical studies, patients with serum creatinine greater than 265 µmol/L or greater than 3.0 mg/dL were excluded and there were only 8 of 564 patients treated with zoledronic acid injection 4 mg by 15-minute infusion with a baseline creatinine greater than 2 mg/dL. Limited pharmacokinetic data exists in patients with creatinine clearance less than 30 mL/min [see Clinical Pharmacology (12.3)].
12.2 Pharmacodynamics
Clinical studies in patients with hypercalcemia of malignancy (HCM) showed that single-dose infusions of zoledronic acid injection are associated with decreases in serum calcium and phosphorus and increases in urinary calcium and phosphorus excretion.
Osteoclastic hyperactivity resulting in excessive bone resorption is the underlying pathophysiologic derangement in hypercalcemia of malignancy (HCM, tumor-induced hypercalcemia) and metastatic bone disease. Excessive release of calcium into the blood as bone is resorbed results in polyuria and gastrointestinal disturbances, with progressive dehydration and decreasing glomerular filtration rate. This, in turn, results in increased renal resorption of calcium, setting up a cycle of worsening systemic hypercalcemia. Reducing excessive bone resorption and maintaining adequate fluid administration are, therefore, essential to the management of hypercalcemia of malignancy.
Patients who have hypercalcemia of malignancy can generally be divided into two groups according to the pathophysiologic mechanism involved: humoral hypercalcemia and hypercalcemia due to tumor invasion of bone. In humoral hypercalcemia, osteoclasts are activated and bone resorption is stimulated by factors such as parathyroid hormone-related protein, which are elaborated by the tumor and circulate systemically. Humoral hypercalcemia usually occurs in squamous cell malignancies of the lung or head and neck or in genitourinary tumors such as renal cell carcinoma or ovarian cancer. Skeletal metastases may be absent or minimal in these patients.
Extensive invasion of bone by tumor cells can also result in hypercalcemia due to local tumor products that stimulate bone resorption by osteoclasts. Tumors commonly associated with locally mediated hypercalcemia include breast cancer and multiple myeloma.
Total serum calcium levels in patients who have hypercalcemia of malignancy may not reflect the severity of hypercalcemia, since concomitant hypoalbuminemia is commonly present. Ideally, ionized calcium levels should be used to diagnose and follow hypercalcemic conditions; however, these are not commonly or rapidly available in many clinical situations. Therefore, adjustment of the total serum calcium value for differences in albumin levels (corrected serum calcium, CSC) is often used in place of measurement of ionized calcium; several nomograms are in use for this type of calculation [see Dosage and Administration (2.1)].
12.3 Pharmacokinetics
Pharmacokinetic data in patients with hypercalcemia are not available.
7.3 Nephrotoxic Drugs
Caution is indicated when zoledronic acid injection is used with other potentially nephrotoxic drugs.
5.8 Hepatic Impairment
Only limited clinical data are available for use of zoledronic acid injection to treat hypercalcemia of malignancy in patients with hepatic insufficiency, and these data are not adequate to provide guidance on dosage selection or how to safely use zoledronic acid injection in these patients.
1 Indications and Usage (1 INDICATIONS AND USAGE)
Zoledronic acid injection is a bisphosphonate indicated for the treatment of:
- Hypercalcemia of malignancy. (1.1)
- Patients with multiple myeloma and patients with documented bone metastases from solid tumors, in conjunction with standard antineoplastic therapy. Prostate cancer should have progressed after treatment with at least one hormonal therapy. (1.2)
Limitations of Use: The safety and efficacy of zoledronic acid injection has not been established for use in hyperparathyroidism or non-tumor-related hypercalcemia.
12.1 Mechanism of Action
The principal pharmacologic action of zoledronic acid is inhibition of bone resorption. Although the antiresorptive mechanism is not completely understood, several factors are thought to contribute to this action. In vitro, zoledronic acid inhibits osteoclastic activity and induces osteoclast apoptosis. Zoledronic acid also blocks the osteoclastic resorption of mineralized bone and cartilage through its binding to bone. Zoledronic acid inhibits the increased osteoclastic activity and skeletal calcium release induced by various stimulatory factors released by tumors.
5.5 Musculoskeletal Pain
In postmarketing experience, severe and occasionally incapacitating bone, joint, and/or muscle pain has been reported in patients taking bisphosphonates, including zoledronic acid injection. The time to onset of symptoms varied from one day to several months after starting the drug. Discontinue use if severe symptoms develop. Most patients had relief of symptoms after stopping. A subset had recurrence of symptoms when rechallenged with the same drug or another bisphosphonate [see Adverse Reactions (6.2)].
5.7 Patients With Asthma
While not observed in clinical trials with zoledronic acid injection, there have been reports of bronchoconstriction in aspirin-sensitive patients receiving bisphosphonates.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Patients being treated with zoledronic acid injection should not be treated with Reclast®. (5.1)
- Adequately rehydrate patients with hypercalcemia of malignancy prior to administration of zoledronic acid injection and monitor electrolytes during treatment. (5.2)
- Renal toxicity may be greater in patients with renal impairment. Do not use doses greater than 4 mg. Treatment in patients with severe renal impairment is not recommended. Monitor serum creatinine before each dose. (5.3)
- Osteonecrosis of the jaw (ONJ) has been reported. Preventive dental exams should be performed before starting zoledronic acid injection. Avoid invasive dental procedures. (5.4)
- Severe incapacitating bone, joint, and/or muscle pain may occur. Discontinue zoledronic acid injection if severe symptoms occur. (5.5)
- Atypical subtrochanteric and diaphyseal femoral fractures have been reported in patients receiving bisphosphonate therapy. These fractures may occur after minimal or no trauma. Evaluate patients with thigh or groin pain to rule out a femoral fracture. Consider drug discontinuation in patients suspected to have an atypical femur fracture. (5.6)
- Hypocalcemia: Correct before initiating zoledronic acid injection. Adequately supplement patients with calcium and vitamin D. Monitor serum calcium closely with concomitant administration of other drugs known to cause hypocalcemia to avoid severe or life-threatening hypocalcemia. (5.9)
- Zoledronic acid injection can cause fetal harm. Advise females of reproductive potential of potential risk to a fetus and to use effective contraception. (5.10, 8.1, 8.3)
5.10 Embryo Fetal Toxicity (5.10 Embryo-Fetal Toxicity)
Based on findings from animal studies and its mechanism of action, zoledronic acid injection can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, administration of zoledronic acid to pregnant rats during organogenesis resulted in fetal malformations and embryo-fetal lethality at maternal exposures that were greater than or equal to 2.4 times the human clinical exposure based on area under the curve (AUC). Bisphosphonates, such as zoledronic acid, are incorporated into the bone matrix, from where they are gradually released over periods of weeks to years. There may be a risk of fetal harm (e.g., skeletal and other abnormalities) if a woman becomes pregnant after completing a course of bisphosphonate therapy. Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during and after zoledronic acid injection treatment [see Use in Specific Populations (8.1, 8.3), Clinical Pharmacology (12.1)].
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
2.3 Preparation of Solution
Zoledronic acid injection must not be mixed with calcium or other divalent cation-containing infusion solutions, such as Lactated Ringer's solution, and should be administered as a single intravenous solution in a line separate from all other drugs.
2.4 Method of Administration
Due to the risk of clinically significant deterioration in renal function, which may progress to renal failure, single doses of zoledronic acid injection should not exceed 4 mg and the duration of infusion should be no less than 15 minutes [see Warnings and Precautions (5.3)]. In the trials and in postmarketing experience, renal deterioration, progression to renal failure and dialysis, have occurred in patients, including those treated with the approved dose of 4 mg infused over 15 minutes. There have been instances of this occurring after the initial zoledronic acid injection dose.
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Injection: 4 mg/5 mL (0.8 mg/mL) single-dose vial for dilution prior to intravenous infusion.
5.4 Osteonecrosis of the Jaw
Osteonecrosis of the jaw (ONJ) has been reported predominantly in cancer patients treated with intravenous bisphosphonates, including zoledronic acid injection. Many of these patients were also receiving chemotherapy and corticosteroids which may be risk factors for ONJ. The risk of ONJ may increase with duration of exposure to bisphosphonates.
Postmarketing experience and the literature suggest a greater frequency of reports of ONJ based on tumor type (advanced breast cancer, multiple myeloma), and dental status (dental extraction, periodontal disease, local trauma including poorly fitting dentures). Many reports of ONJ involved patients with signs of local infection including osteomyelitis.
Cancer patients should maintain good oral hygiene and should have a dental examination with preventive dentistry prior to treatment with bisphosphonates.
While on treatment, these patients should avoid invasive dental procedures if possible. For patients who develop ONJ while on bisphosphonate therapy, dental surgery may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ. Clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment [see Adverse Reactions (6.2)].
6.2 Postmarketing Experience
The following adverse reactions have been reported during postapproval use of zoledronic acid injection. Because these reports are from a population of uncertain size and are subject to confounding factors, it is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Lactation: Advise not to breastfeed. (8.2)
- Females and Males of Reproductive Potential: Verify pregnancy status prior to initiation of zoledronic acid injection. May impair fertility. Counsel patients on pregnancy planning and prevention. (8.3)
- Pediatric Use: Not indicated for use in pediatric patients. (8.4)
- Geriatric Use: Special care to monitor renal function. (8.5)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
1.1 Hypercalcemia of Malignancy
Zoledronic acid injection is indicated for the treatment of hypercalcemia of malignancy defined as an albumin-corrected calcium (cCa) of greater than or equal to 12 mg/dL [3.0 mmol/L] using the formula: cCa in mg/dL = Ca in mg/dL + 0.8 (4.0 g/dL - patient albumin [g/dL]).
2.1 Hypercalcemia of Malignancy
The maximum recommended dose of zoledronic acid injection in hypercalcemia of malignancy (albumin-corrected serum calcium greater than or equal to 12 mg/dL [3.0 mmol/L]) is 4 mg. The 4-mg dose must be given as a single-dose intravenous infusion over no less than 15 minutes. Patients who receive zoledronic acid injection should have serum creatinine assessed prior to each treatment.
Dose adjustments of zoledronic acid injection are not necessary in treating patients for hypercalcemia of malignancy presenting with mild-to-moderate renal impairment prior to initiation of therapy (serum creatinine less than 400 µmol/L or less than 4.5 mg/dL).
Patients should be adequately rehydrated prior to administration of zoledronic acid injection [see Warnings and Precautions (5.2)].
Consideration should be given to the severity of, as well as the symptoms of, tumor-induced hypercalcemia when considering use of zoledronic acid injection. Vigorous saline hydration, an integral part of hypercalcemia therapy, should be initiated promptly and an attempt should be made to restore the urine output to about 2 L/day throughout treatment. Mild or asymptomatic hypercalcemia may be treated with conservative measures (i.e., saline hydration, with or without loop diuretics). Patients should be hydrated adequately throughout the treatment, but overhydration, especially in those patients who have cardiac failure, must be avoided. Diuretic therapy should not be employed prior to correction of hypovolemia.
Retreatment with zoledronic acid injection 4 mg may be considered if serum calcium does not return to normal or remain normal after initial treatment. It is recommended that a minimum of 7 days elapse before retreatment, to allow for full response to the initial dose. Renal function must be carefully monitored in all patients receiving zoledronic acid injection and serum creatinine must be assessed prior to retreatment with zoledronic acid injection [see Warnings and Precautions (5.2)].
14.1 Hypercalcemia of Malignancy
Two identical multicenter, randomized, double-blind, double-dummy studies of zoledronic acid injection 4 mg given as a 5-minute intravenous infusion or pamidronate 90 mg given as a 2-hour intravenous infusion were conducted in 185 patients with hypercalcemia of malignancy (HCM). NOTE: Administration of zoledronic acid injection 4 mg given as a 5-minute intravenous infusion has been shown to result in an increased risk of renal toxicity, as measured by increases in serum creatinine, which can progress to renal failure. The incidence of renal toxicity and renal failure has been shown to be reduced when zoledronic acid injection 4 mg is given as a 15-minute intravenous infusion. Zoledronic acid injection should be administered by intravenous infusion over no less than 15 minutes [see Warnings and Precautions (5.1, 5.2), Dosage and Administration (2.4)]. The treatment groups in the clinical studies were generally well balanced with regards to age, sex, race, and tumor types. The mean age of the study population was 59 years; 81% were Caucasian, 15% were Black, and 4% were of other races. Sixty percent (60%) of the patients were male. The most common tumor types were lung, breast, head and neck, and renal.
In these studies, HCM was defined as a corrected serum calcium (CSC) concentration of greater than or equal to 12.0 mg/dL (3.00 mmol/L). The primary efficacy variable was the proportion of patients having a complete response, defined as the lowering of the CSC to less than or equal to 10.8 mg/dL (2.70 mmol/L) within 10 days after drug infusion.
To assess the effects of zoledronic acid injection versus those of pamidronate, the two multi-center HCM studies were combined in a preplanned analysis. The results of the primary analysis revealed that the proportion of patients that had normalization of corrected serum calcium by Day 10 were 88% and 70% for zoledronic acid injection 4 mg and pamidronate 90 mg, respectively (P=0.002) (see Figure 1). In these studies, no additional benefit was seen for zoledronic acid injection 8 mg over zoledronic acid injection 4 mg; however, the risk of renal toxicity of zoledronic acid injection 8 mg was significantly greater than that seen with zoledronic acid injection 4 mg.
Secondary efficacy variables from the pooled HCM studies included the proportion of patients who had normalization of corrected serum calcium (CSC) by Day 4; the proportion of patients who had normalization of CSC by Day 7; time to relapse of HCM; and duration of complete response. Time to relapse of HCM was defined as the duration (in days) of normalization of serum calcium from study drug infusion until the last CSC value less than 11.6 mg/dL (less than 2.90 mmol/L). Patients who did not have a complete response were assigned a time to relapse of 0 days. Duration of complete response was defined as the duration (in days) from the occurrence of a complete response until the last CSC less than or equal to 10.8 mg/dL (2.70 mmol/L). The results of these secondary analyses for zoledronic acid injection 4 mg and pamidronate 90 mg are shown in Table 11.
| Zoledronic Acid Injection 4 mg | Pamidronate 90 mg | |||
|---|---|---|---|---|
| Complete Response | N | Response Rate | N | Response Rate |
| By Day 4 | 86 | 45.3% | 99 | 33.3% |
| By Day 7 | 86 | 82.6% P less than 0.05 versus pamidronate 90 mg.
|
99 | 63.6% |
| Duration of Response | N | Median Duration (Days) | N | Median Duration (Days) |
| Time to Relapse | 86 | 30 | 99 | 17 |
| Duration of Complete Response | 76 | 32 | 69 | 18 |
7.1 Aminoglycosides and Calcitonin
Caution is advised when bisphosphonates are administered with aminoglycosides or calcitonin, since these agents may have an additive effect to lower serum calcium level for prolonged periods. This effect has not been reported in zoledronic acid injection clinical trials.
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
Zoledronic Acid Injection 4 mg/5 mL (0.8 mg/mL) Single-Dose Vial for Dilution Prior to Intravenous Infusion
Each 5 mL vial contains 4.264 mg zoledronic acid monohydrate, corresponding to 4 mg zoledronic acid on an anhydrous basis, 220 mg of mannitol, USP, 24 mg of sodium citrate, USP, and water for injection.
| NDC No. | Strength | Vial Size |
|---|---|---|
| 69367-190-50 | 4 mg per 5 mL (0.8 mg per mL) |
5 mL fill in a 5 mL single-dose vial |
5.2 Hydration and Electrolyte Monitoring
Patients with hypercalcemia of malignancy must be adequately rehydrated prior to administration of zoledronic acid injection. Loop diuretics should not be used until the patient is adequately rehydrated and should be used with caution in combination with zoledronic acid injection in order to avoid hypocalcemia. Zoledronic acid injection should be used with caution with other nephrotoxic drugs.
Standard hypercalcemia-related metabolic parameters, such as serum levels of calcium, phosphate, and magnesium, as well as serum creatinine, should be carefully monitored following initiation of therapy with zoledronic acid injection. If hypocalcemia, hypophosphatemia, or hypomagnesemia occur, short-term supplemental therapy may be necessary.
Principal Display Panel 5 Ml Vial Carton (PRINCIPAL DISPLAY PANEL - 5 mL Vial Carton)
NDC 69367-190-50
Rx only
Zoledronic Acid
Injection
4 mg per 5 mL
(0.8 mg per mL)
For Intravenous Infusion after Dilution
Sterile
Not for direct injection.
DOSE MUST BE DILUTED.
Do not mix with calcium-containing
infusion solutions.
One 5 mL Single-Dose Vial
Westminster
Pharmaceuticals
1.2 Multiple Myeloma and Bone Metastases of Solid Tumors
Zoledronic acid injection is indicated for the treatment of patients with multiple myeloma and patients with documented bone metastases from solid tumors, in conjunction with standard antineoplastic therapy. Prostate cancer should have progressed after treatment with at least one hormonal therapy.
2.2 Multiple Myeloma and Bone Metastases of Solid Tumors
The recommended dose of zoledronic acid injection in patients with multiple myeloma and metastatic bone lesions from solid tumors for patients with creatinine clearance (CrCl) greater than 60 mL/min is 4 mg infused over no less than 15 minutes every 3 to 4 weeks. The optimal duration of therapy is not known.
Upon treatment initiation, the recommended zoledronic acid injection doses for patients with reduced renal function (mild and moderate renal impairment) are listed in Table 1. These doses are calculated to achieve the same area under the curve (AUC) as that achieved in patients with creatinine clearance of 75 mL/min. CrCl is calculated using the Cockcroft-Gault formula [see Warnings and Precautions (5.2)].
| Baseline Creatinine Clearance (mL/min) |
Zoledronic Acid Injection Recommended Dose (mg) Doses calculated assuming target AUC of 0.66 (mg∙hr/L) (CrCl = 75 mL/min)
|
|---|---|
| greater than 60 | 4 |
| 50-60 | 3.5 |
| 40-49 | 3.3 |
| 30-39 | 3 |
During treatment, serum creatinine should be measured before each zoledronic acid injection dose and treatment should be withheld for renal deterioration. In the clinical studies, renal deterioration was defined as follows:
-
For patients with normal baseline creatinine, increase of 0.5 mg/dL
-
For patients with abnormal baseline creatinine, increase of 1.0 mg/dL
In the clinical studies, zoledronic acid injection treatment was resumed only when the creatinine returned to within 10% of the baseline value. Zoledronic acid injection should be reinitiated at the same dose as that prior to treatment interruption.
Patients should also be administered an oral calcium supplement of 500 mg and a multiple vitamin containing 400 international units of vitamin D daily.
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Standard lifetime carcinogenicity bioassays were conducted in mice and rats. Mice were given oral doses of zoledronic acid of 0.1, 0.5, or 2.0 mg/kg/day. There was an increased incidence of Harderian gland adenomas in males and females in all treatment groups (at doses greater than or equal to 0.002 times a human intravenous dose of 4 mg, based on a comparison of relative body surface areas). Rats were given oral doses of zoledronic acid of 0.1, 0.5, or 2.0 mg/kg/day. No increased incidence of tumors was observed (at doses less than or equal to 0.2 times the human intravenous dose of 4 mg, based on a comparison of relative body surface areas).
Zoledronic acid was not genotoxic in the Ames bacterial mutagenicity assay, in the Chinese hamster ovary cell assay, or in the Chinese hamster gene mutation assay, with or without metabolic activation. Zoledronic acid was not genotoxic in the in vivo rat micronucleus assay.
Female rats were given subcutaneous doses of zoledronic acid of 0.01, 0.03, or 0.1 mg/kg/day beginning 15 days before mating and continuing through gestation. Effects observed in the high-dose group (with systemic exposure of 1.2 times the human systemic exposure following an intravenous dose of 4 mg, based on AUC comparison) included inhibition of ovulation and a decrease in the number of pregnant rats. Effects observed in both the mid-dose group (with systemic exposure of 0.2 times the human systemic exposure following an intravenous dose of 4 mg, based on an AUC comparison) and high-dose group included an increase in preimplantation losses and a decrease in the number of implantations and live fetuses.
5.6 Atypical Subtrochanteric and Diaphyseal Femoral Fractures
Atypical subtrochanteric and diaphyseal femoral fractures have been reported in patients receiving bisphosphonate therapy, including zoledronic acid injection. These fractures can occur anywhere in the femoral shaft from just below the lesser trochanter to just above the supracondylar flare and are transverse or short oblique in orientation without evidence of comminution. These fractures occur after minimal or no trauma. Patients may experience thigh or groin pain weeks to months before presenting with a completed femoral fracture. Fractures are often bilateral; therefore the contralateral femur should be examined in bisphosphonate-treated patients who have sustained a femoral shaft fracture. Poor healing of these fractures has also been reported. A number of case reports noted that patients were also receiving treatment with glucocorticoids (such as prednisone or dexamethasone) at the time of fracture. Causality with bisphosphonate therapy has not been established.
Any patient with a history of bisphosphonate exposure who presents with thigh or groin pain in the absence of trauma should be suspected of having an atypical fracture and should be evaluated. Discontinuation of zoledronic acid injection therapy in patients suspected to have an atypical femur fracture should be considered pending evaluation of the patient, based on an individual benefit risk assessment. It is unknown whether the risk of atypical femur fracture continues after stopping therapy.
5.1 Drugs With Same Active Ingredient Or in the Same Drug Class (5.1 Drugs With Same Active Ingredient or in the Same Drug Class)
Zoledronic acid injection contains the same active ingredient as found in Reclast® (zoledronic acid). Patients being treated with zoledronic acid injection should not be treated with Reclast or other bisphosphonates.
14.2 Clinical Trials in Multiple Myeloma and Bone Metastases of Solid Tumors
Table 12 describes an overview of the efficacy population in three randomized zoledronic acid injection trials in patients with multiple myeloma and bone metastases of solid tumors. These trials included a pamidronate-controlled study in breast cancer and multiple myeloma, a placebo-controlled study in prostate cancer, and a placebo-controlled study in other solid tumors. The prostate cancer study required documentation of previous bone metastases and 3 consecutive rising PSAs while on hormonal therapy. The other placebo-controlled solid tumor study included patients with bone metastases from malignancies other than breast cancer and prostate cancer, including NSCLC, renal cell cancer, small cell lung cancer, colorectal cancer, bladder cancer, GI/genitourinary cancer, head and neck cancer, and others. These trials were comprised of a core phase and an extension phase. In the solid tumor, breast cancer and multiple myeloma trials, only the core phase was evaluated for efficacy as a high percentage of patients did not choose to participate in the extension phase. In the prostate cancer trials, both the core and extension phases were evaluated for efficacy showing the zoledronic acid injection effect during the first 15 months was maintained without decrement or improvement for another 9 months. The design of these clinical trials does not permit assessment of whether more than one-year administration of zoledronic acid injection is beneficial. The optimal duration of zoledronic acid injection administration is not known.
The studies were amended twice because of renal toxicity. The zoledronic acid injection infusion duration was increased from 5 minutes to 15 minutes. After all patients had been accrued, but while dosing and follow-up continued, patients in the 8 mg zoledronic acid injection treatment arm were switched to 4 mg due to toxicity. Patients who were randomized to the zoledronic acid injection 8 mg group are not included in these analyses.
| Patient Population | No. of Patients | Zoledronic Acid Injection Dose | Control | Median Duration (Planned Duration) Zoledronic Acid Injection 4 mg |
|---|---|---|---|---|
| Multiple myeloma or metastatic breast cancer | 1,648 | 4 and 8 Patients who were randomized to the 8 mg zoledronic acid injection group are not included in any of the analyses in this package insert. mg Q3-4 weeks |
Pamidronate 90 mg Q3-4 weeks | 12.0 months (13 months) |
| Metastatic prostate cancer | 643 | 4 and 8 mg Q3 weeks | Placebo | 10.5 months (15 months) |
| Metastatic solid tumor other than breast or prostate cancer | 773 | 4 and 8 mg Q3 weeks | Placebo | 3.8 months (9 months) |
Each study evaluated skeletal-related events (SREs), defined as any of the following: pathologic fracture, radiation therapy to bone, surgery to bone, or spinal cord compression. Change in antineoplastic therapy due to increased pain was a SRE in the prostate cancer study only. Planned analyses included the proportion of patients with a SRE during the study and time to the first SRE. Results for the two zoledronic acid injection placebo-controlled studies are given in Table 13.
| I. Analysis of Proportion of Patients with a SRE SRE=Skeletal-Related Event.
|
II. Analysis of Time to the First SRE | ||||||
|---|---|---|---|---|---|---|---|
| Study | Study Arm & Patient Number | Proportion | Difference Difference for the proportion of patients with a SRE of zoledronic acid injection 4 mg versus placebo. & 95% CI |
P-value | Median (Days) | Hazard Ratio Hazard ratio for the first occurrence of a SRE of zoledronic acid injection 4 mg versus placebo. & 95% CI |
P-value |
| Prostate Cancer | Zoledronic Acid Injection 4 mg (n=214) |
33% | -11% (-20%, -1%) |
0.02 | Not Reached | 0.67 (0.49, 0.91) |
0.011 |
| Placebo (n=208) |
44% | 321 | |||||
| Solid Tumors | Zoledronic Acid Injection 4 mg (n=257) |
38% | -7% (-15%, 2%) |
0.13 | 230 | 0.73 (0.55, 0.96) |
0.023 |
| Placebo (n=250) |
44% | 163 |
In the breast cancer and myeloma trial, efficacy was determined by a noninferiority analysis comparing zoledronic acid injection to pamidronate 90 mg for the proportion of patients with a SRE. This analysis required an estimation of pamidronate efficacy. Historical data from 1,128 patients in three pamidronate placebo-controlled trials demonstrated that pamidronate decreased the proportion of patients with a SRE by 13.1% (95% CI = 7.3%, 18.9%). Results of the comparison of treatment with zoledronic acid injection compared to pamidronate are given in Table 14.
| I. Analysis of Proportion of Patients with a SRE SRE=Skeletal-Related Event.
|
II. Analysis of Time to the First SRE | ||||||
|---|---|---|---|---|---|---|---|
| Study | Study Arm & Patient Number | Proportion | Difference Difference for the proportion of patients with a SRE of zoledronic acid injection 4 mg versus pamidronate 90 mg. & 95% CI |
P-value | Median (Days) | Hazard Ratio Hazard ratio for the first occurrence of a SRE of zoledronic acid injection 4 mg versus pamidronate 90 mg. & 95% CI |
P-value |
| Multiple Myeloma & Breast Cancer | Zoledronic Acid Injection 4 mg (n=561) |
44% | -2% (-7.9%, 3.7%) |
0.46 | 373 | 0.92 (0.77, 1.09) |
0.32 |
| Pamidronate (n=555) |
46% | 363 |
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:37:52.312636 · Updated: 2026-03-14T21:52:26.652971