Atnaa
596c7a8f-27cd-4de2-9491-476f43570b8b
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
ATNAA is indicated for the treatment of poisoning by susceptible organophosphorus nerve agents having anticholinesterase activity in adults.
Dosage and Administration
ATNAA is intended as an initial treatment as soon as symptoms appear; definitive medical care should be sought immediately. ( 2.1 ) Dosage for Mild Symptoms: If a service member experiences some or all of the mild symptoms, they should self-administer one injection intramuscularly into the lateral thigh muscle or buttocks. If, at any time after the first dose, the service member develops any of the severe symptoms or if the mild symptoms are not relieved, a buddy should administer two additional injections intramuscularly in rapid succession. ( 2.2 ) Dosage for Severe Symptoms: If a service member has any of the severe symptoms, immediately buddy-administer three injections intramuscularly into the service member's lateral thigh muscle or buttocks in rapid succession. ( 2.2 )
Contraindications
None.
Warnings and Precautions
Cardiovascular (CV) Risks: Tachycardia, palpitations, premature ventricular contractions, flutter, fibrillation, etc. Use caution in individuals with known CV disease or conduction problems. ( 5.1 ) Heat Injury: May inhibit sweating and lead to hyperthermia; avoid excessive exercising and heat exposure. ( 5.2 ) Acute Glaucoma: May precipitate in susceptible individuals. ( 5.3 ) Urinary Retention : Administer with caution in individuals with bladder outflow obstruction. ( 5.4 ) Pyloric Stenosis: May convert into complete obstruction. ( 5.5 ) Exacerbation of Chronic Lung Disease: Atropine may cause inspiration of bronchial secretions and formation of dangerous viscid plugs in individuals with chronic lung disease; monitor respiratory status. ( 5.6 )
Adverse Reactions
The following serious adverse reactions are described elsewhere in the labeling: Cardiovascular Risks [see Warnings and Precautions (5.1) ] Heat Injury [see Warnings and Precautions (5.2) ] Acute Glaucoma [see Warnings and Precautions (5.3) ] Urinary Retention [see Warnings and Precautions (5.4) ] Pyloric Stenosis [see Warnings and Precautions (5.5) ] Exacerbation of Chronic Lung Disease [see Warnings and Precautions (5.6) ] The following adverse reactions associated with the use of atropine and pralidoxime chloride were identified in the literature. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Drug Interactions
Succinylcholine and Mivacurium: Accelerated reversal of neuromuscular blocking effects may occur; monitor with concomitant administration. ( 7.1 )
How Supplied
Each single-dose ATNAA autoinjector contains atropine (2.1 mg/0.7 mL; colorless to yellow solution, visible in front chamber) and pralidoxime chloride (600 mg/2mL, equivalent to pralidoxime 476.6 mg/2 mL; colorless to yellow solution, not visible in rear chamber). ATNAA, NDC-11704-777-01, is supplied through the Directorate of Medical Materiel, Defense Supply Center, Philadelphia. Each ATNAA is supplied in a pouch that provides protection from light.
Storage and Handling
Each single-dose ATNAA autoinjector contains atropine (2.1 mg/0.7 mL; colorless to yellow solution, visible in front chamber) and pralidoxime chloride (600 mg/2mL, equivalent to pralidoxime 476.6 mg/2 mL; colorless to yellow solution, not visible in rear chamber). ATNAA, NDC-11704-777-01, is supplied through the Directorate of Medical Materiel, Defense Supply Center, Philadelphia. Each ATNAA is supplied in a pouch that provides protection from light.
Description
ATNAA is indicated for the treatment of poisoning by susceptible organophosphorus nerve agents having anticholinesterase activity in adults.
Medication Information
Warnings and Precautions
Cardiovascular (CV) Risks: Tachycardia, palpitations, premature ventricular contractions, flutter, fibrillation, etc. Use caution in individuals with known CV disease or conduction problems. ( 5.1 ) Heat Injury: May inhibit sweating and lead to hyperthermia; avoid excessive exercising and heat exposure. ( 5.2 ) Acute Glaucoma: May precipitate in susceptible individuals. ( 5.3 ) Urinary Retention : Administer with caution in individuals with bladder outflow obstruction. ( 5.4 ) Pyloric Stenosis: May convert into complete obstruction. ( 5.5 ) Exacerbation of Chronic Lung Disease: Atropine may cause inspiration of bronchial secretions and formation of dangerous viscid plugs in individuals with chronic lung disease; monitor respiratory status. ( 5.6 )
Indications and Usage
ATNAA is indicated for the treatment of poisoning by susceptible organophosphorus nerve agents having anticholinesterase activity in adults.
Dosage and Administration
ATNAA is intended as an initial treatment as soon as symptoms appear; definitive medical care should be sought immediately. ( 2.1 ) Dosage for Mild Symptoms: If a service member experiences some or all of the mild symptoms, they should self-administer one injection intramuscularly into the lateral thigh muscle or buttocks. If, at any time after the first dose, the service member develops any of the severe symptoms or if the mild symptoms are not relieved, a buddy should administer two additional injections intramuscularly in rapid succession. ( 2.2 ) Dosage for Severe Symptoms: If a service member has any of the severe symptoms, immediately buddy-administer three injections intramuscularly into the service member's lateral thigh muscle or buttocks in rapid succession. ( 2.2 )
Contraindications
None.
Adverse Reactions
The following serious adverse reactions are described elsewhere in the labeling: Cardiovascular Risks [see Warnings and Precautions (5.1) ] Heat Injury [see Warnings and Precautions (5.2) ] Acute Glaucoma [see Warnings and Precautions (5.3) ] Urinary Retention [see Warnings and Precautions (5.4) ] Pyloric Stenosis [see Warnings and Precautions (5.5) ] Exacerbation of Chronic Lung Disease [see Warnings and Precautions (5.6) ] The following adverse reactions associated with the use of atropine and pralidoxime chloride were identified in the literature. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Drug Interactions
Succinylcholine and Mivacurium: Accelerated reversal of neuromuscular blocking effects may occur; monitor with concomitant administration. ( 7.1 )
Storage and Handling
Each single-dose ATNAA autoinjector contains atropine (2.1 mg/0.7 mL; colorless to yellow solution, visible in front chamber) and pralidoxime chloride (600 mg/2mL, equivalent to pralidoxime 476.6 mg/2 mL; colorless to yellow solution, not visible in rear chamber). ATNAA, NDC-11704-777-01, is supplied through the Directorate of Medical Materiel, Defense Supply Center, Philadelphia. Each ATNAA is supplied in a pouch that provides protection from light.
How Supplied
Each single-dose ATNAA autoinjector contains atropine (2.1 mg/0.7 mL; colorless to yellow solution, visible in front chamber) and pralidoxime chloride (600 mg/2mL, equivalent to pralidoxime 476.6 mg/2 mL; colorless to yellow solution, not visible in rear chamber). ATNAA, NDC-11704-777-01, is supplied through the Directorate of Medical Materiel, Defense Supply Center, Philadelphia. Each ATNAA is supplied in a pouch that provides protection from light.
Description
ATNAA is indicated for the treatment of poisoning by susceptible organophosphorus nerve agents having anticholinesterase activity in adults.
Section 42229-5
Dosage for Mild Symptoms
Section 44425-7
Store between 20ºC to 25ºC (68 ºF to 77ºF); excursions permitted between 15ºC and 30ºC (between 59ºF and 86ºF) [See USP Controlled Room Temperature]. Not made with natural rubber latex. Keep from freezing. Protect from light.
Section 59845-8
Instruction Sheet for Military Personnel
Revised: 5/2020
6.1 Atropine
Because ATNAA contains pralidoxime chloride, which may potentiate the effect of atropine, signs of atropinization may occur earlier than might be expected when atropine is used alone.
Common adverse reactions of atropine can be attributed to its antimuscarinic action. These include dryness of the mouth, blurred vision, dry eyes, photophobia, confusion, headache, dizziness, tachycardia, palpitations, flushing, urinary hesitancy or retention, constipation, abdominal pain, abdominal distention, nausea and vomiting, loss of libido, and impotence. Anhidrosis may produce heat intolerance and impairment of temperature regulation in a hot environment. Dysphagia, paralytic ileus, acute angle closure glaucoma, maculopapular rash, petechial rash, and scarletiniform rash have also been reported. Adverse cardiac reactions, including arrhythmias and myocardial infarction, have been reported with atropine [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.2)].
Larger doses of atropine may produce central nervous system effects such as restlessness, tremor, fatigue, locomotor difficulties, delirium, and hallucinations [see Overdosage (10.1)].
Hypersensitivity reactions will occasionally occur; these are usually seen as skin rashes, and may progress to exfoliation. Anaphylactic reaction and laryngospasm are rare.
10.2 Treatment
For atropine overdose, supportive treatment should be administered. If respiration is depressed, artificial respiration with oxygen is necessary. Ice bags, a hypothermia blanket, or other methods of cooling may be required to reduce atropine-induced fever, especially in pediatric patients [see Use in Specific Populations (8.4)]. Catheterization may be necessary if urinary retention occurs. Since atropine elimination largely takes place through the kidney, urinary output must be maintained and increased if possible; intravenous fluids may be indicated. Because of atropine-induced photophobia, the room should be darkened.
A benzodiazepine may be needed to control marked excitement and convulsions. However, large doses for sedation should be avoided because the central nervous system depressant effect may coincide with the depressant effect occurring late in severe atropine poisoning. Barbiturates are potentiated by the anticholinesterases; therefore, barbiturates should be used cautiously in the treatment of convulsions. Central nervous system stimulants are not recommended.
11 Description
Each prefilled ATNAA is a single-dose autoinjector that provides an intramuscular dose of atropine, a cholinergic muscarinic antagonist, and pralidoxime chloride, a cholinesterase reactivator, in a self-contained unit, specifically designed for automatic self- or buddy-administration by military personnel.
When activated, each ATNAA injection delivers the following:
- 2.1 mg of atropine in 0.7 mL of sterile, pyrogen-free solution containing 12.47 mg glycerin, not more than 2.8 mg phenol, 3.05 mg sodium citrate dihydrate, 3.5 mg citric acid monohydrate, and Water for Injection. The pH range is 4.0 – 5.0.
- 600 mg of pralidoxime chloride equivalent to 476.6 mg of pralidoxime in 2 mL of sterile, pyrogen-free solution containing 40 mg benzyl alcohol, 22.5 mg glycine, and Water for Injection. The pH is adjusted with hydrochloric acid. The pH range is 2.0 – 3.0.
After ATNAA has been activated, the empty autoinjector should be disposed of properly [see Dosage and Administration (2.2)]. It cannot be refilled, nor can the protruding needle be retracted.
Atropine occurs as white crystals, usually needle-like, or as a white, crystalline powder. It is slightly soluble in water with a molecular weight of 289.38. Atropine, a naturally occurring belladonna alkaloid, is a racemic mixture of equal parts of d- and l-hyoscyamine, with activity due almost entirely to the levo isomer of the drug.
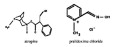
Chemically, atropine is designated as 1αH,5αH-Tropan-3α-ol (±)-tropate. Its empirical formula is C17H23NO3 and its structural formula is as follows:
Pralidoxime chloride is an odorless, white to pale-yellow crystalline powder, freely soluble in water, with a molecular weight of 172.61. Chemically, pralidoxime chloride is designated as 2-formyl-1-methylpyridinium chloride oxime. Its empirical formula is C7H9CIN2O and its structural formula is indicated above.
5.2 Heat Injury
Atropine may inhibit sweating which, in a warm environment or with excessive exercise, can lead to hyperthermia and heat injury. To the extent feasible, avoid excessive exercise and heat exposure [see Overdosage (10.2)].
8.4 Pediatric Use
Safety and effectiveness of ATNAA in pediatric patients have not been established.
8.5 Geriatric Use
Geriatric individuals may be more susceptible to the effects of atropine [see Clinical Pharmacology (12.3)].
5.3 Acute Glaucoma
Atropine should be administered with caution in individuals at risk for acute glaucoma.
6.3 Injection Site
Muscle tightness and pain may occur at the injection site.
4 Contraindications
None.
6 Adverse Reactions
The following serious adverse reactions are described elsewhere in the labeling:
- Cardiovascular Risks [see Warnings and Precautions (5.1)]
- Heat Injury [see Warnings and Precautions (5.2)]
- Acute Glaucoma [see Warnings and Precautions (5.3)]
- Urinary Retention [see Warnings and Precautions (5.4)]
- Pyloric Stenosis [see Warnings and Precautions (5.5)]
- Exacerbation of Chronic Lung Disease [see Warnings and Precautions (5.6)]
The following adverse reactions associated with the use of atropine and pralidoxime chloride were identified in the literature. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
7 Drug Interactions
- Succinylcholine and Mivacurium: Accelerated reversal of neuromuscular blocking effects may occur; monitor with concomitant administration. (7.1)
5.5 Pyloric Stenosis
Atropine should be administered with caution in individuals with partial pyloric stenosis because of the risk of complete pyloric obstruction.
8.6 Renal Impairment
Pralidoxime chloride can cause decreased renal function [see Adverse Reactions (6.2)]. Individuals with severe renal impairment may require less frequent doses after the initial dose.
5.4 Urinary Retention
Atropine should be administered with caution in individuals with clinically significant bladder outflow obstruction because of the risk of urinary retention.
8.7 Hepatic Impairment
Individuals with severe hepatic impairment may require less frequent doses after the initial dose.
1 Indications and Usage
ATNAA is indicated for the treatment of poisoning by susceptible organophosphorus nerve agents having anticholinesterase activity in adults.
5.1 Cardiovascular Risks
Cardiovascular adverse reactions reported in the literature for atropine include, but are not limited to, sinus tachycardia, palpitations, premature ventricular contractions, atrial flutter, atrial fibrillation, ventricular flutter, ventricular fibrillation, cardiac syncope, asystole, and myocardial infarction. In individuals with a recent myocardial infarction and/or severe coronary artery disease, there is a possibility that atropine-induced tachycardia may cause ischemia, extend or initiate myocardial infarcts, and stimulate ventricular ectopy and fibrillation. ATNAA should be used with caution in individuals with known cardiovascular disease or cardiac conduction problems.
6.2 Pralidoxime Chloride
Pralidoxime chloride can cause blurred vision, diplopia and impaired accommodation, dizziness, headache, drowsiness, nausea, tachycardia, increased systolic and diastolic blood pressure [see Clinical Pharmacology 12.2)], muscular weakness, dry mouth, emesis, rash, dry skin, hyperventilation, decreased renal function, and decreased sweating when given parenterally to normal adult volunteers who have not been exposed to anticholinesterase poisons.
In several cases of organophosphorus poisoning, excitement and manic behavior have occurred immediately following recovery of consciousness, in either the presence or absence of pralidoxime chloride administration. However, similar behavior has not been reported in subjects given pralidoxime chloride in the absence of organophosphorus poisoning.
Elevations in AST and/or ALT enzyme levels were observed in 1 of 6 normal adult volunteers given 1200 mg of pralidoxime chloride intramuscularly, and in 4 of 6 adult volunteers given 1800 mg intramuscularly. Levels returned to normal in about two weeks. Transient elevations in creatine kinase were observed in all normal volunteers given the drug.
6.4 Inadvertent Injection
In cases where ATNAA is inadvertently administered to service members who are not poisoned with susceptible organophosphorus nerve agents having anticholinesterase activity, the following effects on their ability to function normally may occur.
Atropine 2 mg IM, roughly the equivalent of one ATNAA injection, when given to healthy male volunteers, is associated with minimal effects on visual, motor, and mental functions, though unsteadiness walking and difficulty concentrating may occur. Atropine reduces body sweating and increases body temperature, particularly with exercise and under hot conditions.
Atropine 4 mg IM, roughly the equivalent of two ATNAA injections, when given to healthy male volunteers, is associated with impaired visual acuity, visual near point accommodation, logical reasoning, digital recall, learning, and cognitive reaction time. Ability to read is reduced or lost. Subjects are unsteady and need to concentrate on walking. These effects begin about 15 minutes to one hour or more post-dose.
Atropine 6 mg IM, roughly the equivalent of three ATNAA injections, when given to healthy male volunteers, is associated with the effects described above plus additional central effects including poor coordination, poor attention span, and visual hallucinations (colored flashes) in many subjects. Frank visual hallucinations, auditory hallucinations, disorientation, and ataxia occur in some subjects. Skilled and labor-intense tasks are performed more slowly and less efficiently. Decision making takes longer and is sometimes impaired.
It is unclear if the above data, obtained from studies of healthy male subjects, can be extrapolated to other populations. In the elderly and individuals with co-morbid conditions, the effects of ≥2 mg atropine on the ability to see, walk, and think properly are unstudied; effects may be greater in susceptible populations.
Service members who are mistakenly injected with ATNAA should avoid potentially dangerous overheating, avoid vigorous physical activity, and seek medical attention as soon as feasible.
5 Warnings and Precautions
- Cardiovascular (CV) Risks: Tachycardia, palpitations, premature ventricular contractions, flutter, fibrillation, etc. Use caution in individuals with known CV disease or conduction problems. (5.1)
- Heat Injury: May inhibit sweating and lead to hyperthermia; avoid excessive exercising and heat exposure. (5.2)
- Acute Glaucoma: May precipitate in susceptible individuals. (5.3)
- Urinary Retention: Administer with caution in individuals with bladder outflow obstruction. (5.4)
- Pyloric Stenosis: May convert into complete obstruction. (5.5)
- Exacerbation of Chronic Lung Disease: Atropine may cause inspiration of bronchial secretions and formation of dangerous viscid plugs in individuals with chronic lung disease; monitor respiratory status. (5.6)
2 Dosage and Administration
- ATNAA is intended as an initial treatment as soon as symptoms appear; definitive medical care should be sought immediately. (2.1)
- Dosage for Mild Symptoms: If a service member experiences some or all of the mild symptoms, they should self-administer one injection intramuscularly into the lateral thigh muscle or buttocks. If, at any time after the first dose, the service member develops any of the severe symptoms or if the mild symptoms are not relieved, a buddy should administer two additional injections intramuscularly in rapid succession. (2.2)
- Dosage for Severe Symptoms: If a service member has any of the severe symptoms, immediately buddy-administer three injections intramuscularly into the service member's lateral thigh muscle or buttocks in rapid succession. (2.2)
3 Dosage Forms and Strengths
Injection: Each single-dose ATNAA autoinjector contains the following in two separate chambers:
- front chamber (visible): a clear, colorless to yellow, sterile solution of atropine (2.1 mg/0.7 mL)
- back chamber (not visible): a clear, colorless to yellow, sterile solution of pralidoxime chloride (600 mg/2 mL) equivalent to pralidoxime (476.6 mg/2 mL)
When activated, ATNAA sequentially administers both drugs intramuscularly through a single needle in one injection.
8 Use in Specific Populations
- Geriatric individuals may be more susceptible to the effects of atropine. (8.5)
2.3 Administration Instructions
The following instructions should be given to service members for the administration of ATNAA single-dose injections.
7.1 Succinylcholine and Mivacurium
Since pralidoxime chloride in ATNAA reactivates cholinesterases and succinylcholine and mivacurium are metabolized by cholinesterases, service members poisoned by susceptible organophosphorus nerve agents having anticholinesterase activity who have received ATNAA may exhibit accelerated reversal of the neuromuscular blocking effects of succinylcholine and mivacurium (relative to poisoned service member who has not received pralidoxime). Monitor for neuromuscular effects with concomitant administration.
16 How Supplied/storage and Handling
Each single-dose ATNAA autoinjector contains atropine (2.1 mg/0.7 mL; colorless to yellow solution, visible in front chamber) and pralidoxime chloride (600 mg/2mL, equivalent to pralidoxime 476.6 mg/2 mL; colorless to yellow solution, not visible in rear chamber). ATNAA, NDC-11704-777-01, is supplied through the Directorate of Medical Materiel, Defense Supply Center, Philadelphia.
Each ATNAA is supplied in a pouch that provides protection from light.
2.1 Important Administration Information
- Three (3) ATNAA single-dose autoinjectors should be available for use by each service member at risk for organophosphorus nerve agent poisoning; one (1) for mild symptoms plus two (2) more for severe symptoms [see Dosage and Administration (2.2)]. Note that individuals may not have all symptoms included under the mild or severe symptom category.
- For optimal reactivation of organophosphorus-inhibited cholinesterase, the ATNAA should be administered as soon as possible after appearance of symptoms of organophosphorus nerve agent poisoning.
- ATNAA should be self- or buddy–administered by service members after donning protective mask and hood at the first sign of a chemical attack, and only if some or all of the mild symptoms of organophosphorus nerve agent exposure are present.
- Only administer ATNAA to service members experiencing symptoms of organophosphorus nerve agent poisoning in a situation where exposure is known or suspected. The ATNAA autoinjector is intended as an initial treatment of the symptoms of organophosphorus nerve agent poisoning as soon as symptoms appear; definitive medical care should be sought immediately.
- Close supervision of all treated service members is indicated for at least 48 to 72 hours.
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit [see Dosage Forms and Strengths (3)].
5.6 Exacerbation of Chronic Lung Disease
Atropine may cause inspiration of bronchial secretions and formation of dangerous viscid plugs in individuals with chronic lung disease. Respiratory status should be monitored in individuals with chronic lung disease following administration of ATNAA.
Principal Display Panel Kit Carton Label
ANTIDOTE TREATMENT
NERVE AGENT, AUTO-INJECTOR
For Use in Nerve Agent Poisoning Only
(atropine and pralidoxime chloride injection) Each single-dose auto-injector
delivers an intramuscular injection of 2.1 mg/0.7 mL of atropine and
600 mg/2 mL of pralidoxime chloride equivalent to 476.6 mg pralidoxime.
Distributed by: Defense
Logistics Agency Troop
Support, Philadelphia
Medical Directorate
Manufactured for: U.S.
Army Medical Research
and Development
Command, by Meridian
Medical Technologies,LLC
1
2
3
10 SECONDS
ATNAA Utilizes
Binaject® Technology
0002163
Sterile Solution for Intramuscular Use Only
NSN 6505-01-362-7427
Rx Only
Store at 25°C (77°F); excursions
permitted to 15 - 30°C (59 - 86°F).
Keep From Freezing. Protect From Light.
Structured Label Content
Section 42229-5 (42229-5)
Dosage for Mild Symptoms
Section 44425-7 (44425-7)
Store between 20ºC to 25ºC (68 ºF to 77ºF); excursions permitted between 15ºC and 30ºC (between 59ºF and 86ºF) [See USP Controlled Room Temperature]. Not made with natural rubber latex. Keep from freezing. Protect from light.
Section 59845-8 (59845-8)
Instruction Sheet for Military Personnel
Revised: 5/2020
6.1 Atropine
Because ATNAA contains pralidoxime chloride, which may potentiate the effect of atropine, signs of atropinization may occur earlier than might be expected when atropine is used alone.
Common adverse reactions of atropine can be attributed to its antimuscarinic action. These include dryness of the mouth, blurred vision, dry eyes, photophobia, confusion, headache, dizziness, tachycardia, palpitations, flushing, urinary hesitancy or retention, constipation, abdominal pain, abdominal distention, nausea and vomiting, loss of libido, and impotence. Anhidrosis may produce heat intolerance and impairment of temperature regulation in a hot environment. Dysphagia, paralytic ileus, acute angle closure glaucoma, maculopapular rash, petechial rash, and scarletiniform rash have also been reported. Adverse cardiac reactions, including arrhythmias and myocardial infarction, have been reported with atropine [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.2)].
Larger doses of atropine may produce central nervous system effects such as restlessness, tremor, fatigue, locomotor difficulties, delirium, and hallucinations [see Overdosage (10.1)].
Hypersensitivity reactions will occasionally occur; these are usually seen as skin rashes, and may progress to exfoliation. Anaphylactic reaction and laryngospasm are rare.
10.2 Treatment
For atropine overdose, supportive treatment should be administered. If respiration is depressed, artificial respiration with oxygen is necessary. Ice bags, a hypothermia blanket, or other methods of cooling may be required to reduce atropine-induced fever, especially in pediatric patients [see Use in Specific Populations (8.4)]. Catheterization may be necessary if urinary retention occurs. Since atropine elimination largely takes place through the kidney, urinary output must be maintained and increased if possible; intravenous fluids may be indicated. Because of atropine-induced photophobia, the room should be darkened.
A benzodiazepine may be needed to control marked excitement and convulsions. However, large doses for sedation should be avoided because the central nervous system depressant effect may coincide with the depressant effect occurring late in severe atropine poisoning. Barbiturates are potentiated by the anticholinesterases; therefore, barbiturates should be used cautiously in the treatment of convulsions. Central nervous system stimulants are not recommended.
11 Description (11 DESCRIPTION)
Each prefilled ATNAA is a single-dose autoinjector that provides an intramuscular dose of atropine, a cholinergic muscarinic antagonist, and pralidoxime chloride, a cholinesterase reactivator, in a self-contained unit, specifically designed for automatic self- or buddy-administration by military personnel.
When activated, each ATNAA injection delivers the following:
- 2.1 mg of atropine in 0.7 mL of sterile, pyrogen-free solution containing 12.47 mg glycerin, not more than 2.8 mg phenol, 3.05 mg sodium citrate dihydrate, 3.5 mg citric acid monohydrate, and Water for Injection. The pH range is 4.0 – 5.0.
- 600 mg of pralidoxime chloride equivalent to 476.6 mg of pralidoxime in 2 mL of sterile, pyrogen-free solution containing 40 mg benzyl alcohol, 22.5 mg glycine, and Water for Injection. The pH is adjusted with hydrochloric acid. The pH range is 2.0 – 3.0.
After ATNAA has been activated, the empty autoinjector should be disposed of properly [see Dosage and Administration (2.2)]. It cannot be refilled, nor can the protruding needle be retracted.
Atropine occurs as white crystals, usually needle-like, or as a white, crystalline powder. It is slightly soluble in water with a molecular weight of 289.38. Atropine, a naturally occurring belladonna alkaloid, is a racemic mixture of equal parts of d- and l-hyoscyamine, with activity due almost entirely to the levo isomer of the drug.
Chemically, atropine is designated as 1αH,5αH-Tropan-3α-ol (±)-tropate. Its empirical formula is C17H23NO3 and its structural formula is as follows:
Pralidoxime chloride is an odorless, white to pale-yellow crystalline powder, freely soluble in water, with a molecular weight of 172.61. Chemically, pralidoxime chloride is designated as 2-formyl-1-methylpyridinium chloride oxime. Its empirical formula is C7H9CIN2O and its structural formula is indicated above.
5.2 Heat Injury
Atropine may inhibit sweating which, in a warm environment or with excessive exercise, can lead to hyperthermia and heat injury. To the extent feasible, avoid excessive exercise and heat exposure [see Overdosage (10.2)].
8.4 Pediatric Use
Safety and effectiveness of ATNAA in pediatric patients have not been established.
8.5 Geriatric Use
Geriatric individuals may be more susceptible to the effects of atropine [see Clinical Pharmacology (12.3)].
5.3 Acute Glaucoma
Atropine should be administered with caution in individuals at risk for acute glaucoma.
6.3 Injection Site
Muscle tightness and pain may occur at the injection site.
4 Contraindications (4 CONTRAINDICATIONS)
None.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following serious adverse reactions are described elsewhere in the labeling:
- Cardiovascular Risks [see Warnings and Precautions (5.1)]
- Heat Injury [see Warnings and Precautions (5.2)]
- Acute Glaucoma [see Warnings and Precautions (5.3)]
- Urinary Retention [see Warnings and Precautions (5.4)]
- Pyloric Stenosis [see Warnings and Precautions (5.5)]
- Exacerbation of Chronic Lung Disease [see Warnings and Precautions (5.6)]
The following adverse reactions associated with the use of atropine and pralidoxime chloride were identified in the literature. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
7 Drug Interactions (7 DRUG INTERACTIONS)
- Succinylcholine and Mivacurium: Accelerated reversal of neuromuscular blocking effects may occur; monitor with concomitant administration. (7.1)
5.5 Pyloric Stenosis
Atropine should be administered with caution in individuals with partial pyloric stenosis because of the risk of complete pyloric obstruction.
8.6 Renal Impairment
Pralidoxime chloride can cause decreased renal function [see Adverse Reactions (6.2)]. Individuals with severe renal impairment may require less frequent doses after the initial dose.
5.4 Urinary Retention
Atropine should be administered with caution in individuals with clinically significant bladder outflow obstruction because of the risk of urinary retention.
8.7 Hepatic Impairment
Individuals with severe hepatic impairment may require less frequent doses after the initial dose.
1 Indications and Usage (1 INDICATIONS AND USAGE)
ATNAA is indicated for the treatment of poisoning by susceptible organophosphorus nerve agents having anticholinesterase activity in adults.
5.1 Cardiovascular Risks
Cardiovascular adverse reactions reported in the literature for atropine include, but are not limited to, sinus tachycardia, palpitations, premature ventricular contractions, atrial flutter, atrial fibrillation, ventricular flutter, ventricular fibrillation, cardiac syncope, asystole, and myocardial infarction. In individuals with a recent myocardial infarction and/or severe coronary artery disease, there is a possibility that atropine-induced tachycardia may cause ischemia, extend or initiate myocardial infarcts, and stimulate ventricular ectopy and fibrillation. ATNAA should be used with caution in individuals with known cardiovascular disease or cardiac conduction problems.
6.2 Pralidoxime Chloride
Pralidoxime chloride can cause blurred vision, diplopia and impaired accommodation, dizziness, headache, drowsiness, nausea, tachycardia, increased systolic and diastolic blood pressure [see Clinical Pharmacology 12.2)], muscular weakness, dry mouth, emesis, rash, dry skin, hyperventilation, decreased renal function, and decreased sweating when given parenterally to normal adult volunteers who have not been exposed to anticholinesterase poisons.
In several cases of organophosphorus poisoning, excitement and manic behavior have occurred immediately following recovery of consciousness, in either the presence or absence of pralidoxime chloride administration. However, similar behavior has not been reported in subjects given pralidoxime chloride in the absence of organophosphorus poisoning.
Elevations in AST and/or ALT enzyme levels were observed in 1 of 6 normal adult volunteers given 1200 mg of pralidoxime chloride intramuscularly, and in 4 of 6 adult volunteers given 1800 mg intramuscularly. Levels returned to normal in about two weeks. Transient elevations in creatine kinase were observed in all normal volunteers given the drug.
6.4 Inadvertent Injection
In cases where ATNAA is inadvertently administered to service members who are not poisoned with susceptible organophosphorus nerve agents having anticholinesterase activity, the following effects on their ability to function normally may occur.
Atropine 2 mg IM, roughly the equivalent of one ATNAA injection, when given to healthy male volunteers, is associated with minimal effects on visual, motor, and mental functions, though unsteadiness walking and difficulty concentrating may occur. Atropine reduces body sweating and increases body temperature, particularly with exercise and under hot conditions.
Atropine 4 mg IM, roughly the equivalent of two ATNAA injections, when given to healthy male volunteers, is associated with impaired visual acuity, visual near point accommodation, logical reasoning, digital recall, learning, and cognitive reaction time. Ability to read is reduced or lost. Subjects are unsteady and need to concentrate on walking. These effects begin about 15 minutes to one hour or more post-dose.
Atropine 6 mg IM, roughly the equivalent of three ATNAA injections, when given to healthy male volunteers, is associated with the effects described above plus additional central effects including poor coordination, poor attention span, and visual hallucinations (colored flashes) in many subjects. Frank visual hallucinations, auditory hallucinations, disorientation, and ataxia occur in some subjects. Skilled and labor-intense tasks are performed more slowly and less efficiently. Decision making takes longer and is sometimes impaired.
It is unclear if the above data, obtained from studies of healthy male subjects, can be extrapolated to other populations. In the elderly and individuals with co-morbid conditions, the effects of ≥2 mg atropine on the ability to see, walk, and think properly are unstudied; effects may be greater in susceptible populations.
Service members who are mistakenly injected with ATNAA should avoid potentially dangerous overheating, avoid vigorous physical activity, and seek medical attention as soon as feasible.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Cardiovascular (CV) Risks: Tachycardia, palpitations, premature ventricular contractions, flutter, fibrillation, etc. Use caution in individuals with known CV disease or conduction problems. (5.1)
- Heat Injury: May inhibit sweating and lead to hyperthermia; avoid excessive exercising and heat exposure. (5.2)
- Acute Glaucoma: May precipitate in susceptible individuals. (5.3)
- Urinary Retention: Administer with caution in individuals with bladder outflow obstruction. (5.4)
- Pyloric Stenosis: May convert into complete obstruction. (5.5)
- Exacerbation of Chronic Lung Disease: Atropine may cause inspiration of bronchial secretions and formation of dangerous viscid plugs in individuals with chronic lung disease; monitor respiratory status. (5.6)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
- ATNAA is intended as an initial treatment as soon as symptoms appear; definitive medical care should be sought immediately. (2.1)
- Dosage for Mild Symptoms: If a service member experiences some or all of the mild symptoms, they should self-administer one injection intramuscularly into the lateral thigh muscle or buttocks. If, at any time after the first dose, the service member develops any of the severe symptoms or if the mild symptoms are not relieved, a buddy should administer two additional injections intramuscularly in rapid succession. (2.2)
- Dosage for Severe Symptoms: If a service member has any of the severe symptoms, immediately buddy-administer three injections intramuscularly into the service member's lateral thigh muscle or buttocks in rapid succession. (2.2)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Injection: Each single-dose ATNAA autoinjector contains the following in two separate chambers:
- front chamber (visible): a clear, colorless to yellow, sterile solution of atropine (2.1 mg/0.7 mL)
- back chamber (not visible): a clear, colorless to yellow, sterile solution of pralidoxime chloride (600 mg/2 mL) equivalent to pralidoxime (476.6 mg/2 mL)
When activated, ATNAA sequentially administers both drugs intramuscularly through a single needle in one injection.
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Geriatric individuals may be more susceptible to the effects of atropine. (8.5)
2.3 Administration Instructions
The following instructions should be given to service members for the administration of ATNAA single-dose injections.
7.1 Succinylcholine and Mivacurium
Since pralidoxime chloride in ATNAA reactivates cholinesterases and succinylcholine and mivacurium are metabolized by cholinesterases, service members poisoned by susceptible organophosphorus nerve agents having anticholinesterase activity who have received ATNAA may exhibit accelerated reversal of the neuromuscular blocking effects of succinylcholine and mivacurium (relative to poisoned service member who has not received pralidoxime). Monitor for neuromuscular effects with concomitant administration.
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
Each single-dose ATNAA autoinjector contains atropine (2.1 mg/0.7 mL; colorless to yellow solution, visible in front chamber) and pralidoxime chloride (600 mg/2mL, equivalent to pralidoxime 476.6 mg/2 mL; colorless to yellow solution, not visible in rear chamber). ATNAA, NDC-11704-777-01, is supplied through the Directorate of Medical Materiel, Defense Supply Center, Philadelphia.
Each ATNAA is supplied in a pouch that provides protection from light.
2.1 Important Administration Information
- Three (3) ATNAA single-dose autoinjectors should be available for use by each service member at risk for organophosphorus nerve agent poisoning; one (1) for mild symptoms plus two (2) more for severe symptoms [see Dosage and Administration (2.2)]. Note that individuals may not have all symptoms included under the mild or severe symptom category.
- For optimal reactivation of organophosphorus-inhibited cholinesterase, the ATNAA should be administered as soon as possible after appearance of symptoms of organophosphorus nerve agent poisoning.
- ATNAA should be self- or buddy–administered by service members after donning protective mask and hood at the first sign of a chemical attack, and only if some or all of the mild symptoms of organophosphorus nerve agent exposure are present.
- Only administer ATNAA to service members experiencing symptoms of organophosphorus nerve agent poisoning in a situation where exposure is known or suspected. The ATNAA autoinjector is intended as an initial treatment of the symptoms of organophosphorus nerve agent poisoning as soon as symptoms appear; definitive medical care should be sought immediately.
- Close supervision of all treated service members is indicated for at least 48 to 72 hours.
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit [see Dosage Forms and Strengths (3)].
5.6 Exacerbation of Chronic Lung Disease
Atropine may cause inspiration of bronchial secretions and formation of dangerous viscid plugs in individuals with chronic lung disease. Respiratory status should be monitored in individuals with chronic lung disease following administration of ATNAA.
Principal Display Panel Kit Carton Label (PRINCIPAL DISPLAY PANEL - Kit Carton Label)
ANTIDOTE TREATMENT
NERVE AGENT, AUTO-INJECTOR
For Use in Nerve Agent Poisoning Only
(atropine and pralidoxime chloride injection) Each single-dose auto-injector
delivers an intramuscular injection of 2.1 mg/0.7 mL of atropine and
600 mg/2 mL of pralidoxime chloride equivalent to 476.6 mg pralidoxime.
Distributed by: Defense
Logistics Agency Troop
Support, Philadelphia
Medical Directorate
Manufactured for: U.S.
Army Medical Research
and Development
Command, by Meridian
Medical Technologies,LLC
1
2
3
10 SECONDS
ATNAA Utilizes
Binaject® Technology
0002163
Sterile Solution for Intramuscular Use Only
NSN 6505-01-362-7427
Rx Only
Store at 25°C (77°F); excursions
permitted to 15 - 30°C (59 - 86°F).
Keep From Freezing. Protect From Light.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:37:07.369444 · Updated: 2026-03-14T21:48:58.126908