Levothyroxine Sodium Injection
50b1c8a4-75b6-49c8-80fc-3841ee80b183
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Levothyroxine Sodium Injection is indicated for the treatment of myxedema coma.
Dosage and Administration
Consider the age, general physical condition, cardiac risk factors, and clinical severity of myxedema and duration of myxedema symptoms when determining dosages of Levothyroxine Sodium Injection. ( 2.1 ) Start with lower doses in elderly patients and in patients with underlying cardiovascular disease. ( 2.1 ) The recommended loading dose is 300 mcg to 500 mcg administered intravenously. ( 2.1 ) The recommended maintenance dose is 50 mcg to 100 mcg administered intravenously daily until the patient can tolerate oral therapy. ( 2.1 ) Administer Levothyroxine Sodium Injection intravenously at a rate not to exceed 100 mcg per minute. ( 2.2 ) Do not add Levothyroxine Sodium Injection to intravenous fluids. ( 2.2 )
Contraindications
Uncorrected adrenal insufficiency [see Warnings and Precautions ( 5.2 )]
Warnings and Precautions
Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease: Overtreatment may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration ( 5.1 ). Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency: Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment ( 5.2 ). Worsening of Diabetic Control: May worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control ( 5.3 ).
Adverse Reactions
Overtreatment with Levothyroxine Sodium Injection may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration of Levothyroxine Sodium Injection for cardiac adverse reactions.
Drug Interactions
See full prescribing information for drugs that affect thyroid hormone pharmacokinetics and metabolism (e.g., synthesis, secretion, catabolism, protein binding, and target tissue response) that may alter the therapeutic response to Levothyroxine Sodium Injection. ( 7 )
How Supplied
Levothyroxine Sodium Injection is a clear, colorless solution available as follows: NDC Total Strength per Total Volume Concentration 63323-885-12 100 mcg per 5 mL 20 mcg per mL Protect from light in the original vial in a carton and store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. The unopened vial may be stored for up to 24 hours exposed to indoor lighting outside of the carton. The drug product is preservative free. Discard any unused portion. PREMIERProRx ® is a registered trademark of Premier Healthcare Alliance, L.P., used under license. Manufactured by: Fresenius Kabi Lake Zurich, IL 60047 www.fresenius-kabi.com/us 451681
Storage and Handling
Levothyroxine Sodium Injection is a clear, colorless solution available as follows: NDC Total Strength per Total Volume Concentration 63323-885-12 100 mcg per 5 mL 20 mcg per mL Protect from light in the original vial in a carton and store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. The unopened vial may be stored for up to 24 hours exposed to indoor lighting outside of the carton. The drug product is preservative free. Discard any unused portion. PREMIERProRx ® is a registered trademark of Premier Healthcare Alliance, L.P., used under license. Manufactured by: Fresenius Kabi Lake Zurich, IL 60047 www.fresenius-kabi.com/us 451681
Description
Thyroid hormones, including Levothyroxine Sodium Injection, should not be used for the treatment of obesity or for weight loss. Larger doses may produce serious or even life threatening manifestations of toxicity. ( 6 , 10 )
Medication Information
Warnings and Precautions
Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease: Overtreatment may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration ( 5.1 ). Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency: Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment ( 5.2 ). Worsening of Diabetic Control: May worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control ( 5.3 ).
Indications and Usage
Levothyroxine Sodium Injection is indicated for the treatment of myxedema coma.
Dosage and Administration
Consider the age, general physical condition, cardiac risk factors, and clinical severity of myxedema and duration of myxedema symptoms when determining dosages of Levothyroxine Sodium Injection. ( 2.1 ) Start with lower doses in elderly patients and in patients with underlying cardiovascular disease. ( 2.1 ) The recommended loading dose is 300 mcg to 500 mcg administered intravenously. ( 2.1 ) The recommended maintenance dose is 50 mcg to 100 mcg administered intravenously daily until the patient can tolerate oral therapy. ( 2.1 ) Administer Levothyroxine Sodium Injection intravenously at a rate not to exceed 100 mcg per minute. ( 2.2 ) Do not add Levothyroxine Sodium Injection to intravenous fluids. ( 2.2 )
Contraindications
Uncorrected adrenal insufficiency [see Warnings and Precautions ( 5.2 )]
Adverse Reactions
Overtreatment with Levothyroxine Sodium Injection may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration of Levothyroxine Sodium Injection for cardiac adverse reactions.
Drug Interactions
See full prescribing information for drugs that affect thyroid hormone pharmacokinetics and metabolism (e.g., synthesis, secretion, catabolism, protein binding, and target tissue response) that may alter the therapeutic response to Levothyroxine Sodium Injection. ( 7 )
Storage and Handling
Levothyroxine Sodium Injection is a clear, colorless solution available as follows: NDC Total Strength per Total Volume Concentration 63323-885-12 100 mcg per 5 mL 20 mcg per mL Protect from light in the original vial in a carton and store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. The unopened vial may be stored for up to 24 hours exposed to indoor lighting outside of the carton. The drug product is preservative free. Discard any unused portion. PREMIERProRx ® is a registered trademark of Premier Healthcare Alliance, L.P., used under license. Manufactured by: Fresenius Kabi Lake Zurich, IL 60047 www.fresenius-kabi.com/us 451681
How Supplied
Levothyroxine Sodium Injection is a clear, colorless solution available as follows: NDC Total Strength per Total Volume Concentration 63323-885-12 100 mcg per 5 mL 20 mcg per mL Protect from light in the original vial in a carton and store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. The unopened vial may be stored for up to 24 hours exposed to indoor lighting outside of the carton. The drug product is preservative free. Discard any unused portion. PREMIERProRx ® is a registered trademark of Premier Healthcare Alliance, L.P., used under license. Manufactured by: Fresenius Kabi Lake Zurich, IL 60047 www.fresenius-kabi.com/us 451681
Description
Thyroid hormones, including Levothyroxine Sodium Injection, should not be used for the treatment of obesity or for weight loss. Larger doses may produce serious or even life threatening manifestations of toxicity. ( 6 , 10 )
Section 42229-5
Limitations of Use:
Not recommended as a substitute for oral levothyroxine sodium because the relative bioavailability of Levothyroxine Sodium Injection to oral levothyroxine sodium has not been established and there is a risk of inaccurate dose conversion.
Section 51945-4
PACKAGE LABEL - PRINCIPAL DISPLAY – Levothyroxine Sodium Injection 5 mL Vial Label
NDC 63323-885-12
Levothyroxine Sodium
Injection
100 mcg per 5 mL
(20 mcg per mL)
For intravenous use.
Preservative free.
5 mL Single-Dose Vial-
Discard Unused Portion
2.1 Dosage
- Consider the age, general physical condition, cardiac risk factors, and clinical severity of myxedema and duration of myxedema symptoms when determining the starting and maintenance dosages of Levothyroxine Sodium Injection.
- Start with lower doses in elderly patients and in patients with underlying cardiovascular disease [see Warnings and Precautions (5.1) and Use in Specific Populations (8.5)].
- The recommended loading dose of Levothyroxine Sodium Injection is 300 mcg to 500 mcg administered intravenously.
- The recommended maintenance dose of Levothyroxine Sodium Injection is 50 mcg to 100 mcg administered intravenously daily until the patient can tolerate oral therapy.
7.6 Ketamine
Concurrent use of ketamine and levothyroxine may produce marked hypertension and tachycardia. Closely monitor blood pressure and heart rate in these patients.
10 Overdosage
The signs and symptoms of overdosage are those of hyperthyroidism [see Warnings and Precautions (5) and Adverse Reactions (6)]. In addition, confusion and disorientation may occur. Cerebral embolism, shock, coma, and death have been reported. Reduce the Levothyroxine Sodium Injection dose or temporarily discontinue if signs or symptoms of overdosage occur. Initiate appropriate supportive treatment as dictated by the patient's medical status.
11 Description
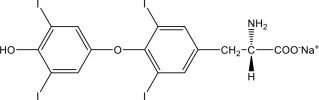
Levothyroxine Sodium Injection contains synthetic crystalline levothyroxine (T4) in sodium salt form. Levothyroxine sodium has an empirical formula of C15H10I4NNaO4, a molecular weight of 798.85 g/mol (anhydrous), and the following structural formula:
Levothyroxine Sodium Injection is a sterile, preservative free, clear, colorless, sterile solution for intravenous administration available as: 100 mcg per 5 mL (20 mcg per mL). Each mL of Levothyroxine Sodium Injection also contains 10 mg Tromethamine, USP; 0.14 mg Sodium Iodide, USP; 6.48 mg Sodium Chloride, USP; and Water for Injection, USP Sodium hydroxide, NF and/or Hydrochloric acid, USP may have been added for pH adjustment (9.5 – 10.8). Levothyroxine Sodium Injection is in single dose clear glass vials.
8.4 Pediatric Use
The safety and efficacy of Levothyroxine Sodium Injection have not been established in pediatric patients.
8.5 Geriatric Use
Because of the increased prevalence of cardiovascular disease among the elderly, initiate Levothyroxine Sodium Injection with lower doses in elderly patients and in patients with underlying cardiovascular disease and closely monitor for cardiac adverse reactions. Atrial arrhythmias can occur in elderly patients. Atrial fibrillation is the most common of the arrhythmias observed with levothyroxine overtreatment in the elderly [see Dosage and Administration (2.1) and Warnings and Precautions (5.1)].
4 Contraindications
Uncorrected adrenal insufficiency [see Warnings and Precautions (5.2)]
6 Adverse Reactions
Adverse reactions associated with levothyroxine are primarily those of hyperthyroidism due to therapeutic overdosage [see Warnings and Precautions (5) , Overdosage (10) ]. They include the following:
- General: fatigue, increased appetite, weight loss, heat intolerance, fever, excessive sweating
- Central nervous system: headache, hyperactivity, nervousness, anxiety, irritability, emotional lability, insomnia
- Musculoskeletal: tremors, muscle weakness, muscle spasm
- Cardiovascular: palpitations, tachycardia, arrhythmias, increased pulse and blood pressure, heart failure, angina, myocardial infarction, cardiac arrest
- Respiratory: dyspnea
- Gastrointestinal: diarrhea, vomiting, abdominal cramps, elevations in liver function tests
- Dermatologic: flushing, rash
Seizures have been reported rarely with the institution of levothyroxine therapy.
7 Drug Interactions
See full prescribing information for drugs that affect thyroid hormone pharmacokinetics and metabolism (e.g., synthesis, secretion, catabolism, protein binding, and target tissue response) that may alter the therapeutic response to Levothyroxine Sodium Injection. (7)
7.7 Sympathomimetics
Concurrent use may of sympathomimetics and levothyroxine may increase the effects of sympathomimetics or thyroid hormone. Thyroid hormones may increase the risk of coronary insufficiency when sympathomimetic agents are administered to patients with coronary artery disease.
12.2 Pharmacodynamics
Levothyroxine sodium is a synthetic T4 hormone that exerts the same physiologic effect as endogenous T4, thereby maintaining normal T4 levels when a deficiency is present.
1 Indications and Usage
Levothyroxine Sodium Injection is indicated for the treatment of myxedema coma.
7.3 Oral Anticoagulants
Levothyroxine increases the response to oral anticoagulant therapy. Therefore, a decrease in the dose of anticoagulant may be warranted with correction of the hypothyroid state. Closely monitor coagulation tests to permit appropriate and timely dosage adjustments.
12.1 Mechanism of Action
Thyroid hormones exert their physiologic actions through control of DNA transcription and protein synthesis. Triiodothyronine (T3) and levothyroxine (T4) diffuse into the cell nucleus and bind to thyroid receptor proteins attached to DNA. This hormone nuclear receptor complex activates gene transcription and synthesis of messenger RNA and cytoplasmic proteins.
The physiological actions of thyroid hormones are produced predominantly by T3, the majority of which (approximately 80%) is derived from T4 by deiodination in peripheral tissues.
7.2 Antidiabetic Therapy
Addition of levothyroxine to antidiabetic or insulin therapy may result in increased antidiabetic agent or insulin requirements. Careful monitoring of glycemic control is recommended.
7.4 Digitalis Glycosides
Levothyroxine may reduce the therapeutic effects of digitalis glycosides. Serum digitalis glycoside levels may be decreased when a hypothyroid patient becomes euthyroid, necessitating an increase in the dose of digitalis glycosides.
5 Warnings and Precautions
- Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease: Overtreatment may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration (5.1).
- Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency: Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment (5.2).
- Worsening of Diabetic Control: May worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control (5.3).
7.5 Antidepressant Therapy
Concurrent use of tricyclic (e.g., amitriptyline) or tetracyclic (e.g., maprotiline) antidepressants and levothyroxine may increase the therapeutic and toxic effects of both drugs, possibly due to increased receptor sensitivity to catecholamines. Toxic effects may include increased risk of cardiac arrhythmias and central nervous system stimulation. Levothyroxine may accelerate the onset of action of tricyclics. Administration of sertraline in patients stabilized on levothyroxine may result in increased levothyroxine requirements.
2 Dosage and Administration
- Consider the age, general physical condition, cardiac risk factors, and clinical severity of myxedema and duration of myxedema symptoms when determining dosages of Levothyroxine Sodium Injection. (2.1)
- Start with lower doses in elderly patients and in patients with underlying cardiovascular disease. (2.1)
- The recommended loading dose is 300 mcg to 500 mcg administered intravenously. (2.1)
- The recommended maintenance dose is 50 mcg to 100 mcg administered intravenously daily until the patient can tolerate oral therapy. (2.1)
- Administer Levothyroxine Sodium Injection intravenously at a rate not to exceed 100 mcg per minute. (2.2)
- Do not add Levothyroxine Sodium Injection to intravenous fluids. (2.2)
3 Dosage Forms and Strengths
Levothyroxine Sodium Injection is clear, colorless solution supplied as:
- 100 mcg per 5 mL (20 mcg per mL) single-dose vial
2.2 Administration Instructions
- Administer Levothyroxine Sodium Injection as an intravenous injection at a rate not to exceed 100 mcg per minute.
- Do not add Levothyroxine Sodium Injection to intravenous fluids.
- Inspect Levothyroxine Sodium Injection visually prior to injection. It should appear clear and colorless, solution free of visible particulates. Do not use if particulate matter or coloration is seen.
- Discard any unused portion.
5.3 Worsening of Diabetic Control
Addition of levothyroxine therapy in patients with diabetes mellitus may worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control [see Drug Interactions (7.2)].
16 How Supplied/storage and Handling
Levothyroxine Sodium Injection is a clear, colorless solution available as follows:
|
NDC |
Total Strength per Total Volume | Concentration |
| 63323-885-12 | 100 mcg per 5 mL | 20 mcg per mL |
Protect from light in the original vial in a carton and store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. The unopened vial may be stored for up to 24 hours exposed to indoor lighting outside of the carton. The drug product is preservative free. Discard any unused portion.
PREMIERProRx® is a registered trademark of Premier Healthcare Alliance, L.P., used under license.
Manufactured by:
Fresenius Kabi
Lake Zurich, IL 60047
www.fresenius-kabi.com/us
451681
7.8 Drug Laboratory Test Interactions
Consider changes in TBG concentration when interpreting T4 and T3 values. Measure and evaluate unbound (free) hormone and/or determine the free T4 index (FT4I) in this circumstance. Pregnancy, infectious hepatitis, estrogens, estrogen containing oral contraceptives, and acute intermittent porphyria increase TBG concentrations. Nephrosis, severe hypoproteinemia, severe liver disease, acromegaly, androgens, and corticosteroids decrease TBG concentration. Familial hyper- or hypo-thyroxine binding globulinemias have been described, with the incidence of TBG deficiency approximating 1 in 9,000.
Warning: Not for Treatment of Obesity Or for Weight Loss
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Animal studies have not been performed to evaluate the carcinogenic potential, mutagenic potential or effects on fertility of Levothyroxine Sodium Injection.
7.1 Drugs Known to Affect Thyroid Hormone Pharmacokinetics
Many drugs affect thyroid hormone pharmacokinetics and metabolism (e.g., synthesis, secretion, catabolism, protein binding, and target tissue response) and may alter the therapeutic response to Levothyroxine Sodium Injection (see Tables 1-3).
| Drug or Drug Class | Effect |
| Clofibrate Estrogen-containing oral contraceptives Estrogens (oral) Heroin / Methadone 5-Fluorouracil Mitotane Tamoxifen |
These drugs may increase serum thyroxine-binding globulin (TBG) concentration. |
| Androgens / Anabolic Steroids Asparaginase Glucocorticoids Slow-Release Nicotinic Acid |
These drugs may decrease serum TBG concentration. |
| Potential impact (below): Administration of these agents with levothyroxine results in an initial transient increase in FT4. Continued administration results in a decrease in serum T4 and normal FT4 and TSH concentrations. | |
| Salicylates (> 2 g/day) |
Salicylates inhibit binding of T4 and T3 to TBG and transthyretin. An initial increase in serum FT4 is followed by return of FT4 to normal levels with sustained therapeutic serum salicylate concentrations, although total T4 levels may decrease by as much as 30%. |
| Other drugs: Carbamazepine Furosemide (> 80 mg IV) Heparin Hydantoins Non-Steroidal Anti-inflammatory Drugs - Fenamates |
These drugs may cause protein-binding site displacement. Furosemide has been shown to inhibit the protein binding of T4 to TBG and albumin, causing an increase free T4 fraction in serum. Furosemide competes for T4-binding sites on TBG, prealbumin, and albumin, so that a single high dose can acutely lower the total T4 level. Phenytoin and carbamazepine reduce serum protein binding of levothyroxine, and total and free T4 may be reduced by 20% to 40%, but most patients have normal serum TSH levels and are clinically euthyroid. Closely monitor thyroid hormone parameters. |
| Potential impact: Stimulation of hepatic microsomal drug-metabolizing enzyme activity may cause increased hepatic degradation of levothyroxine, resulting in increased levothyroxine requirements. | |
| Drug or Drug Class | Effect |
| Phenobarbital Rifampin |
Phenobarbital has been shown to reduce the response to thyroxine. Phenobarbital increases L-thyroxine metabolism by inducing uridine 5'-diphospho-glucuronosyltransferase (UGT) and leads to a lower T4 serum levels. Changes in thyroid status may occur if barbiturates are added or withdrawn from patients being treated for hypothyroidism. Rifampin has been shown to accelerate the metabolism of levothyroxine. |
| Potential impact: Administration of these enzyme inhibitors decreases the peripheral conversion of T4 to T3, leading to decreased T3 levels. However, serum T4 levels are usually normal but may occasionally be slightly increased. | |
| Drug or Drug Class | Effect |
| Beta-adrenergic antagonists (e.g., Propranolol > 160 mg/day) |
In patients treated with large doses of propranolol (> 160 mg/day), T3 and T4 levels change slightly, TSH levels remain normal, and patients are clinically euthyroid. It should be noted that actions of particular beta-adrenergic antagonists may be impaired when the hypothyroid patient is converted to the euthyroid state. |
| Glucocorticoids (e.g., Dexamethasone ≥ 4 mg/day) |
Short-term administration of large doses of glucocorticoids may decrease serum T3 concentrations by 30% with minimal change in serum T4 levels. However, long-term glucocorticoid therapy may result in slightly decreased T3 and T4 levels due to decreased TBG production (See above). |
| Other drugs: Amiodarone |
Amiodarone inhibits peripheral conversion of levothyroxine (T4) to triiodothyronine (T3) and may cause isolated biochemical changes (increase in serum free-T4, and decreased or normal free-T3) in clinically euthyroid patients. |
5.2 Acute Adrenal Crisis in Patients With Concomitant Adrenal Insufficiency
Chronic autoimmune thyroiditis, which can lead to myxedema coma, may occur in association with other autoimmune disorders such as adrenal insufficiency. Thyroid hormone increases metabolic clearance of glucocorticoids. Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency [see Contraindications (4)]. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment with Levothyroxine Sodium Injection.
5.1 Cardiac Adverse Reactions in the Elderly and in Patients With Underlying Cardiovascular Disease
Overtreatment with Levothyroxine Sodium Injection may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration of Levothyroxine Sodium Injection for cardiac adverse reactions.
Structured Label Content
Section 42229-5 (42229-5)
Limitations of Use:
Not recommended as a substitute for oral levothyroxine sodium because the relative bioavailability of Levothyroxine Sodium Injection to oral levothyroxine sodium has not been established and there is a risk of inaccurate dose conversion.
Section 51945-4 (51945-4)
PACKAGE LABEL - PRINCIPAL DISPLAY – Levothyroxine Sodium Injection 5 mL Vial Label
NDC 63323-885-12
Levothyroxine Sodium
Injection
100 mcg per 5 mL
(20 mcg per mL)
For intravenous use.
Preservative free.
5 mL Single-Dose Vial-
Discard Unused Portion
2.1 Dosage
- Consider the age, general physical condition, cardiac risk factors, and clinical severity of myxedema and duration of myxedema symptoms when determining the starting and maintenance dosages of Levothyroxine Sodium Injection.
- Start with lower doses in elderly patients and in patients with underlying cardiovascular disease [see Warnings and Precautions (5.1) and Use in Specific Populations (8.5)].
- The recommended loading dose of Levothyroxine Sodium Injection is 300 mcg to 500 mcg administered intravenously.
- The recommended maintenance dose of Levothyroxine Sodium Injection is 50 mcg to 100 mcg administered intravenously daily until the patient can tolerate oral therapy.
7.6 Ketamine
Concurrent use of ketamine and levothyroxine may produce marked hypertension and tachycardia. Closely monitor blood pressure and heart rate in these patients.
10 Overdosage (10 OVERDOSAGE)
The signs and symptoms of overdosage are those of hyperthyroidism [see Warnings and Precautions (5) and Adverse Reactions (6)]. In addition, confusion and disorientation may occur. Cerebral embolism, shock, coma, and death have been reported. Reduce the Levothyroxine Sodium Injection dose or temporarily discontinue if signs or symptoms of overdosage occur. Initiate appropriate supportive treatment as dictated by the patient's medical status.
11 Description (11 DESCRIPTION)
Levothyroxine Sodium Injection contains synthetic crystalline levothyroxine (T4) in sodium salt form. Levothyroxine sodium has an empirical formula of C15H10I4NNaO4, a molecular weight of 798.85 g/mol (anhydrous), and the following structural formula:
Levothyroxine Sodium Injection is a sterile, preservative free, clear, colorless, sterile solution for intravenous administration available as: 100 mcg per 5 mL (20 mcg per mL). Each mL of Levothyroxine Sodium Injection also contains 10 mg Tromethamine, USP; 0.14 mg Sodium Iodide, USP; 6.48 mg Sodium Chloride, USP; and Water for Injection, USP Sodium hydroxide, NF and/or Hydrochloric acid, USP may have been added for pH adjustment (9.5 – 10.8). Levothyroxine Sodium Injection is in single dose clear glass vials.
8.4 Pediatric Use
The safety and efficacy of Levothyroxine Sodium Injection have not been established in pediatric patients.
8.5 Geriatric Use
Because of the increased prevalence of cardiovascular disease among the elderly, initiate Levothyroxine Sodium Injection with lower doses in elderly patients and in patients with underlying cardiovascular disease and closely monitor for cardiac adverse reactions. Atrial arrhythmias can occur in elderly patients. Atrial fibrillation is the most common of the arrhythmias observed with levothyroxine overtreatment in the elderly [see Dosage and Administration (2.1) and Warnings and Precautions (5.1)].
4 Contraindications (4 CONTRAINDICATIONS)
Uncorrected adrenal insufficiency [see Warnings and Precautions (5.2)]
6 Adverse Reactions (6 ADVERSE REACTIONS)
Adverse reactions associated with levothyroxine are primarily those of hyperthyroidism due to therapeutic overdosage [see Warnings and Precautions (5) , Overdosage (10) ]. They include the following:
- General: fatigue, increased appetite, weight loss, heat intolerance, fever, excessive sweating
- Central nervous system: headache, hyperactivity, nervousness, anxiety, irritability, emotional lability, insomnia
- Musculoskeletal: tremors, muscle weakness, muscle spasm
- Cardiovascular: palpitations, tachycardia, arrhythmias, increased pulse and blood pressure, heart failure, angina, myocardial infarction, cardiac arrest
- Respiratory: dyspnea
- Gastrointestinal: diarrhea, vomiting, abdominal cramps, elevations in liver function tests
- Dermatologic: flushing, rash
Seizures have been reported rarely with the institution of levothyroxine therapy.
7 Drug Interactions (7 DRUG INTERACTIONS)
See full prescribing information for drugs that affect thyroid hormone pharmacokinetics and metabolism (e.g., synthesis, secretion, catabolism, protein binding, and target tissue response) that may alter the therapeutic response to Levothyroxine Sodium Injection. (7)
7.7 Sympathomimetics
Concurrent use may of sympathomimetics and levothyroxine may increase the effects of sympathomimetics or thyroid hormone. Thyroid hormones may increase the risk of coronary insufficiency when sympathomimetic agents are administered to patients with coronary artery disease.
12.2 Pharmacodynamics
Levothyroxine sodium is a synthetic T4 hormone that exerts the same physiologic effect as endogenous T4, thereby maintaining normal T4 levels when a deficiency is present.
1 Indications and Usage (1 INDICATIONS AND USAGE)
Levothyroxine Sodium Injection is indicated for the treatment of myxedema coma.
7.3 Oral Anticoagulants
Levothyroxine increases the response to oral anticoagulant therapy. Therefore, a decrease in the dose of anticoagulant may be warranted with correction of the hypothyroid state. Closely monitor coagulation tests to permit appropriate and timely dosage adjustments.
12.1 Mechanism of Action
Thyroid hormones exert their physiologic actions through control of DNA transcription and protein synthesis. Triiodothyronine (T3) and levothyroxine (T4) diffuse into the cell nucleus and bind to thyroid receptor proteins attached to DNA. This hormone nuclear receptor complex activates gene transcription and synthesis of messenger RNA and cytoplasmic proteins.
The physiological actions of thyroid hormones are produced predominantly by T3, the majority of which (approximately 80%) is derived from T4 by deiodination in peripheral tissues.
7.2 Antidiabetic Therapy
Addition of levothyroxine to antidiabetic or insulin therapy may result in increased antidiabetic agent or insulin requirements. Careful monitoring of glycemic control is recommended.
7.4 Digitalis Glycosides
Levothyroxine may reduce the therapeutic effects of digitalis glycosides. Serum digitalis glycoside levels may be decreased when a hypothyroid patient becomes euthyroid, necessitating an increase in the dose of digitalis glycosides.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease: Overtreatment may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration (5.1).
- Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency: Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment (5.2).
- Worsening of Diabetic Control: May worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control (5.3).
7.5 Antidepressant Therapy
Concurrent use of tricyclic (e.g., amitriptyline) or tetracyclic (e.g., maprotiline) antidepressants and levothyroxine may increase the therapeutic and toxic effects of both drugs, possibly due to increased receptor sensitivity to catecholamines. Toxic effects may include increased risk of cardiac arrhythmias and central nervous system stimulation. Levothyroxine may accelerate the onset of action of tricyclics. Administration of sertraline in patients stabilized on levothyroxine may result in increased levothyroxine requirements.
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
- Consider the age, general physical condition, cardiac risk factors, and clinical severity of myxedema and duration of myxedema symptoms when determining dosages of Levothyroxine Sodium Injection. (2.1)
- Start with lower doses in elderly patients and in patients with underlying cardiovascular disease. (2.1)
- The recommended loading dose is 300 mcg to 500 mcg administered intravenously. (2.1)
- The recommended maintenance dose is 50 mcg to 100 mcg administered intravenously daily until the patient can tolerate oral therapy. (2.1)
- Administer Levothyroxine Sodium Injection intravenously at a rate not to exceed 100 mcg per minute. (2.2)
- Do not add Levothyroxine Sodium Injection to intravenous fluids. (2.2)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Levothyroxine Sodium Injection is clear, colorless solution supplied as:
- 100 mcg per 5 mL (20 mcg per mL) single-dose vial
2.2 Administration Instructions
- Administer Levothyroxine Sodium Injection as an intravenous injection at a rate not to exceed 100 mcg per minute.
- Do not add Levothyroxine Sodium Injection to intravenous fluids.
- Inspect Levothyroxine Sodium Injection visually prior to injection. It should appear clear and colorless, solution free of visible particulates. Do not use if particulate matter or coloration is seen.
- Discard any unused portion.
5.3 Worsening of Diabetic Control
Addition of levothyroxine therapy in patients with diabetes mellitus may worsen glycemic control and result in increased antidiabetic agent or insulin requirements. Carefully monitor glycemic control [see Drug Interactions (7.2)].
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
Levothyroxine Sodium Injection is a clear, colorless solution available as follows:
|
NDC |
Total Strength per Total Volume | Concentration |
| 63323-885-12 | 100 mcg per 5 mL | 20 mcg per mL |
Protect from light in the original vial in a carton and store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. The unopened vial may be stored for up to 24 hours exposed to indoor lighting outside of the carton. The drug product is preservative free. Discard any unused portion.
PREMIERProRx® is a registered trademark of Premier Healthcare Alliance, L.P., used under license.
Manufactured by:
Fresenius Kabi
Lake Zurich, IL 60047
www.fresenius-kabi.com/us
451681
7.8 Drug Laboratory Test Interactions (7.8 Drug-Laboratory Test Interactions)
Consider changes in TBG concentration when interpreting T4 and T3 values. Measure and evaluate unbound (free) hormone and/or determine the free T4 index (FT4I) in this circumstance. Pregnancy, infectious hepatitis, estrogens, estrogen containing oral contraceptives, and acute intermittent porphyria increase TBG concentrations. Nephrosis, severe hypoproteinemia, severe liver disease, acromegaly, androgens, and corticosteroids decrease TBG concentration. Familial hyper- or hypo-thyroxine binding globulinemias have been described, with the incidence of TBG deficiency approximating 1 in 9,000.
Warning: Not for Treatment of Obesity Or for Weight Loss (WARNING: NOT FOR TREATMENT OF OBESITY OR FOR WEIGHT LOSS)
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Animal studies have not been performed to evaluate the carcinogenic potential, mutagenic potential or effects on fertility of Levothyroxine Sodium Injection.
7.1 Drugs Known to Affect Thyroid Hormone Pharmacokinetics
Many drugs affect thyroid hormone pharmacokinetics and metabolism (e.g., synthesis, secretion, catabolism, protein binding, and target tissue response) and may alter the therapeutic response to Levothyroxine Sodium Injection (see Tables 1-3).
| Drug or Drug Class | Effect |
| Clofibrate Estrogen-containing oral contraceptives Estrogens (oral) Heroin / Methadone 5-Fluorouracil Mitotane Tamoxifen |
These drugs may increase serum thyroxine-binding globulin (TBG) concentration. |
| Androgens / Anabolic Steroids Asparaginase Glucocorticoids Slow-Release Nicotinic Acid |
These drugs may decrease serum TBG concentration. |
| Potential impact (below): Administration of these agents with levothyroxine results in an initial transient increase in FT4. Continued administration results in a decrease in serum T4 and normal FT4 and TSH concentrations. | |
| Salicylates (> 2 g/day) |
Salicylates inhibit binding of T4 and T3 to TBG and transthyretin. An initial increase in serum FT4 is followed by return of FT4 to normal levels with sustained therapeutic serum salicylate concentrations, although total T4 levels may decrease by as much as 30%. |
| Other drugs: Carbamazepine Furosemide (> 80 mg IV) Heparin Hydantoins Non-Steroidal Anti-inflammatory Drugs - Fenamates |
These drugs may cause protein-binding site displacement. Furosemide has been shown to inhibit the protein binding of T4 to TBG and albumin, causing an increase free T4 fraction in serum. Furosemide competes for T4-binding sites on TBG, prealbumin, and albumin, so that a single high dose can acutely lower the total T4 level. Phenytoin and carbamazepine reduce serum protein binding of levothyroxine, and total and free T4 may be reduced by 20% to 40%, but most patients have normal serum TSH levels and are clinically euthyroid. Closely monitor thyroid hormone parameters. |
| Potential impact: Stimulation of hepatic microsomal drug-metabolizing enzyme activity may cause increased hepatic degradation of levothyroxine, resulting in increased levothyroxine requirements. | |
| Drug or Drug Class | Effect |
| Phenobarbital Rifampin |
Phenobarbital has been shown to reduce the response to thyroxine. Phenobarbital increases L-thyroxine metabolism by inducing uridine 5'-diphospho-glucuronosyltransferase (UGT) and leads to a lower T4 serum levels. Changes in thyroid status may occur if barbiturates are added or withdrawn from patients being treated for hypothyroidism. Rifampin has been shown to accelerate the metabolism of levothyroxine. |
| Potential impact: Administration of these enzyme inhibitors decreases the peripheral conversion of T4 to T3, leading to decreased T3 levels. However, serum T4 levels are usually normal but may occasionally be slightly increased. | |
| Drug or Drug Class | Effect |
| Beta-adrenergic antagonists (e.g., Propranolol > 160 mg/day) |
In patients treated with large doses of propranolol (> 160 mg/day), T3 and T4 levels change slightly, TSH levels remain normal, and patients are clinically euthyroid. It should be noted that actions of particular beta-adrenergic antagonists may be impaired when the hypothyroid patient is converted to the euthyroid state. |
| Glucocorticoids (e.g., Dexamethasone ≥ 4 mg/day) |
Short-term administration of large doses of glucocorticoids may decrease serum T3 concentrations by 30% with minimal change in serum T4 levels. However, long-term glucocorticoid therapy may result in slightly decreased T3 and T4 levels due to decreased TBG production (See above). |
| Other drugs: Amiodarone |
Amiodarone inhibits peripheral conversion of levothyroxine (T4) to triiodothyronine (T3) and may cause isolated biochemical changes (increase in serum free-T4, and decreased or normal free-T3) in clinically euthyroid patients. |
5.2 Acute Adrenal Crisis in Patients With Concomitant Adrenal Insufficiency (5.2 Acute Adrenal Crisis in Patients with Concomitant Adrenal Insufficiency)
Chronic autoimmune thyroiditis, which can lead to myxedema coma, may occur in association with other autoimmune disorders such as adrenal insufficiency. Thyroid hormone increases metabolic clearance of glucocorticoids. Initiation of thyroid hormone therapy prior to initiating glucocorticoid therapy may precipitate an acute adrenal crisis in patients with adrenal insufficiency [see Contraindications (4)]. Treat patients with adrenal insufficiency with replacement glucocorticoids prior to initiating treatment with Levothyroxine Sodium Injection.
5.1 Cardiac Adverse Reactions in the Elderly and in Patients With Underlying Cardiovascular Disease (5.1 Cardiac Adverse Reactions in the Elderly and in Patients with Underlying Cardiovascular Disease)
Overtreatment with Levothyroxine Sodium Injection may cause arrhythmias, tachycardia, myocardial ischemia and infarction, or worsening of congestive heart failure and death, particularly in patients with cardiovascular disease and in elderly patients. Start with lower doses in elderly patients and in patients with underlying cardiovascular disease and monitor patients after administration of Levothyroxine Sodium Injection for cardiac adverse reactions.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:35:37.925167 · Updated: 2026-03-14T21:43:58.672563