Mesalamine Delayed-release Tablets
4e3b6325-a5bf-4c47-931c-142c0e4d7c3a
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Mesalamine delayed-release tablets are indicated for the: induction and maintenance of remission in adult patients with mildly to moderately active ulcerative colitis. treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg.
Dosage and Administration
Administration Instructions Evaluate renal function prior to initiation of mesalamine delayed-release tablets and periodically while on therapy. ( 2 , 5.1 ) Swallow mesalamine delayed-release tablets whole; do not split or crush. ( 2 ) Administer mesalamine delayed-release tablets with food. ( 2 ) Drink an adequate amount of fluids. ( 2 , 5.8 ) Recommended Dosage in Adults For induction of remission : 2.4 g to 4.8 g (two to four 1.2-g tablets) once daily. ( 2 ) For maintenance of remission : 2.4 g (two 1.2-g tablets) once daily. ( 2 ) Recommended Dosage in Pediatric Patients The recommended dosage for treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg who can swallow tablets whole is shown below: ( 2 ) Weight of Pediatric Patient Once Daily Mesalamine delayed-release tablets Dosage Week 0 to Week 8 After Week 8 24 kg to 35 kg 2.4 g (two 1.2-g tablets) 1.2 g (one 1.2-g tablet) Greater than 35 kg to 50 kg 3.6 g (three 1.2-g tablets) 2.4 g (two 1.2-g tablets) Greater than 50 kg 4.8 g (four 1.2-g tablets) 2.4 g (two 1.2-g tablets)
Contraindications
Mesalamine delayed-release tablets are contraindicated in patients with known or suspected hypersensitivity to salicylates, aminosalicylates, or to any of the ingredients of mesalamine delayed-release tablets [see Warnings and Precautions (5.3) , Adverse Reactions (6.2) , Description (11) ] .
Warnings and Precautions
Renal Impairment : Assess renal function at the beginning of treatment and periodically during treatment. Evaluate the risks and benefits of mesalamine delayed-release tablets in patients with known renal impairment or taking nephrotoxic drugs. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy. ( 5.1 , 7.1 , 8.6 ) Mesalamine-Induced Acute Intolerance Syndrome : Symptoms may be difficult to distinguish from an ulcerative colitis exacerbation. Monitor for worsening symptoms while on treatment. Discontinue treatment if acute intolerance syndrome is suspected. ( 5.2 ) Hypersensitivity Reactions, including myocarditis and pericarditis : Evaluate patients immediately and discontinue mesalamine delayed-release tablets if a hypersensitivity reaction is suspected. ( 5.3 ) Hepatic Failure : Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known liver impairment. ( 5.4 ) Severe Cutaneous Adverse Reactions : Discontinue at the first signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation. ( 5.5 ) Upper Gastrointestinal Tract Obstruction : Avoid in patients with pyloric stenosis or other organic or functional obstruction. ( 5.6 ) Photosensitivity : Advise patients with pre-existing skin conditions to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors. ( 5.7 ) Nephrolithiasis : Cases of nephrolithiasis have been reported with the use of mesalamine. Mesalamine-containing stones are undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment. ( 5.8 ) Interference With Laboratory Tests : Use of mesalamine may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection. ( 5.9 )
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in labeling: Renal impairment, including renal failure [see Warnings and Precautions (5.1) ] Mesalamine-induced acute intolerance syndrome [see Warnings and Precautions (5.2) ] Hypersensitivity reactions [see Warnings and Precautions (5.3) ] Hepatic failure [see Warnings and Precautions (5.4) ] Severe cutaneous adverse reactions [see Warnings and Precautions (5.5) ] Upper gastrointestinal tract obstruction [see Warnings and Precautions (5.6) ] Photosensitivity [see Warnings and Precautions (5.7) ] Nephrolithiasis [see Warnings and Precautions (5.8) ]
Drug Interactions
Nephrotoxic Agents including NSAIDs : Increased risk of nephrotoxicity; monitor for changes in renal function and mesalamine-related adverse reactions. ( 7.1 ) Azathioprine or 6-Mercaptopurine : Increased risk of blood dyscrasias; monitor complete blood cell counts and platelet counts. ( 7.2 )
How Supplied
Mesalamine delayed-release tablets are available as red-brown, ellipsoidal, film-coated delayed-release tablets containing 1.2 g mesalamine, and debossed on one side imprinted with S476. NDC 54092-100-01 HDPE Bottle with a child-resistant closure of 120 delayed-release tablets.
Storage and Handling
Mesalamine delayed-release tablets are available as red-brown, ellipsoidal, film-coated delayed-release tablets containing 1.2 g mesalamine, and debossed on one side imprinted with S476. NDC 54092-100-01 HDPE Bottle with a child-resistant closure of 120 delayed-release tablets.
Description
Warnings and Precautions, Renal Impairment ( 5.1 ) 11/2022
Medication Information
Warnings and Precautions
Renal Impairment : Assess renal function at the beginning of treatment and periodically during treatment. Evaluate the risks and benefits of mesalamine delayed-release tablets in patients with known renal impairment or taking nephrotoxic drugs. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy. ( 5.1 , 7.1 , 8.6 ) Mesalamine-Induced Acute Intolerance Syndrome : Symptoms may be difficult to distinguish from an ulcerative colitis exacerbation. Monitor for worsening symptoms while on treatment. Discontinue treatment if acute intolerance syndrome is suspected. ( 5.2 ) Hypersensitivity Reactions, including myocarditis and pericarditis : Evaluate patients immediately and discontinue mesalamine delayed-release tablets if a hypersensitivity reaction is suspected. ( 5.3 ) Hepatic Failure : Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known liver impairment. ( 5.4 ) Severe Cutaneous Adverse Reactions : Discontinue at the first signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation. ( 5.5 ) Upper Gastrointestinal Tract Obstruction : Avoid in patients with pyloric stenosis or other organic or functional obstruction. ( 5.6 ) Photosensitivity : Advise patients with pre-existing skin conditions to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors. ( 5.7 ) Nephrolithiasis : Cases of nephrolithiasis have been reported with the use of mesalamine. Mesalamine-containing stones are undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment. ( 5.8 ) Interference With Laboratory Tests : Use of mesalamine may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection. ( 5.9 )
Indications and Usage
Mesalamine delayed-release tablets are indicated for the: induction and maintenance of remission in adult patients with mildly to moderately active ulcerative colitis. treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg.
Dosage and Administration
Administration Instructions Evaluate renal function prior to initiation of mesalamine delayed-release tablets and periodically while on therapy. ( 2 , 5.1 ) Swallow mesalamine delayed-release tablets whole; do not split or crush. ( 2 ) Administer mesalamine delayed-release tablets with food. ( 2 ) Drink an adequate amount of fluids. ( 2 , 5.8 ) Recommended Dosage in Adults For induction of remission : 2.4 g to 4.8 g (two to four 1.2-g tablets) once daily. ( 2 ) For maintenance of remission : 2.4 g (two 1.2-g tablets) once daily. ( 2 ) Recommended Dosage in Pediatric Patients The recommended dosage for treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg who can swallow tablets whole is shown below: ( 2 ) Weight of Pediatric Patient Once Daily Mesalamine delayed-release tablets Dosage Week 0 to Week 8 After Week 8 24 kg to 35 kg 2.4 g (two 1.2-g tablets) 1.2 g (one 1.2-g tablet) Greater than 35 kg to 50 kg 3.6 g (three 1.2-g tablets) 2.4 g (two 1.2-g tablets) Greater than 50 kg 4.8 g (four 1.2-g tablets) 2.4 g (two 1.2-g tablets)
Contraindications
Mesalamine delayed-release tablets are contraindicated in patients with known or suspected hypersensitivity to salicylates, aminosalicylates, or to any of the ingredients of mesalamine delayed-release tablets [see Warnings and Precautions (5.3) , Adverse Reactions (6.2) , Description (11) ] .
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in labeling: Renal impairment, including renal failure [see Warnings and Precautions (5.1) ] Mesalamine-induced acute intolerance syndrome [see Warnings and Precautions (5.2) ] Hypersensitivity reactions [see Warnings and Precautions (5.3) ] Hepatic failure [see Warnings and Precautions (5.4) ] Severe cutaneous adverse reactions [see Warnings and Precautions (5.5) ] Upper gastrointestinal tract obstruction [see Warnings and Precautions (5.6) ] Photosensitivity [see Warnings and Precautions (5.7) ] Nephrolithiasis [see Warnings and Precautions (5.8) ]
Drug Interactions
Nephrotoxic Agents including NSAIDs : Increased risk of nephrotoxicity; monitor for changes in renal function and mesalamine-related adverse reactions. ( 7.1 ) Azathioprine or 6-Mercaptopurine : Increased risk of blood dyscrasias; monitor complete blood cell counts and platelet counts. ( 7.2 )
Storage and Handling
Mesalamine delayed-release tablets are available as red-brown, ellipsoidal, film-coated delayed-release tablets containing 1.2 g mesalamine, and debossed on one side imprinted with S476. NDC 54092-100-01 HDPE Bottle with a child-resistant closure of 120 delayed-release tablets.
How Supplied
Mesalamine delayed-release tablets are available as red-brown, ellipsoidal, film-coated delayed-release tablets containing 1.2 g mesalamine, and debossed on one side imprinted with S476. NDC 54092-100-01 HDPE Bottle with a child-resistant closure of 120 delayed-release tablets.
Description
Warnings and Precautions, Renal Impairment ( 5.1 ) 11/2022
Section 42229-5
Administration Instructions
- Evaluate renal function prior to initiation of mesalamine delayed-release tablets and periodically while on therapy.
- Swallow mesalamine delayed-release tablets whole; do not split or crush.
- Administer mesalamine delayed-release tablets with food [see Clinical Pharmacology (12.3)].
- Drink an adequate amount of fluids [see Warnings and Precautions (5.8)].
Section 43683-2
| Warnings and Precautions, Renal Impairment (5.1) | 11/2022 |
Section 44425-7
Store at room temperature 15°C to 25°C (59°F to 77°F); excursions permitted to 30°C (86°F).
See USP Controlled Room Temperature.
10 Overdosage
Mesalamine delayed-release tablets are an aminosalicylate, and symptoms of salicylate toxicity may include nausea, vomiting, abdominal pain, tachypnea, hyperpnea, tinnitus, and neurologic symptoms (headache, dizziness, confusion, seizures). Severe intoxication with salicylates may lead to electrolyte and blood pH imbalance, and potentially end organ (e.g., renal and liver) damage.
There is no specific known antidote for mesalamine overdose; however, conventional therapy for salicylate toxicity may be beneficial in the event of acute overdosage and may include gastrointestinal tract decontamination to prevent further absorption. Correct fluid and electrolyte imbalance by the administration of appropriate intravenous therapy and maintain adequate renal function.
Mesalamine delayed-release tablets are a pH-dependent, delayed-release product and this factor should be considered when treating a suspected overdose.
11 Description
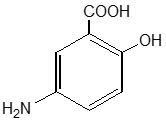
Each mesalamine delayed-release tablet for oral administration contains 1.2 g 5-aminosalicylic acid (5-ASA; mesalamine), an anti-inflammatory agent. Mesalamine also has the chemical name 5-amino-2-hydroxybenzoic acid and its structural formula is:
| Molecular formula: | C7H7NO3 |
| Molecular weight: | 153.14 |
The tablet is coated with a pH-dependent polymer film, which breaks down at or above pH 6.8, normally in the terminal ileum where mesalamine then begins to be released from the tablet core. The tablet core contains mesalamine with hydrophilic and lipophilic excipients and provides for extended release of mesalamine.
The inactive ingredients of a mesalamine delayed-release tablet are sodium carboxymethylcellulose, carnauba wax, stearic acid, silica (colloidal hydrated), sodium starch glycolate (type A), talc, magnesium stearate, methacrylic acid copolymer types A and B, triethylcitrate, titanium dioxide, red ferric oxide, and polyethylene glycol 6000.
8.4 Pediatric Use
The safety and effectiveness of mesalamine delayed-release tablets have been established for the treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg. Use of mesalamine delayed-release tablets in this population is supported by evidence from adequate and well-controlled trials in adults, a multicenter, randomized, double-blind, parallel group trial in 105 pediatric patients 5 to 17 years of age, and additional pharmacokinetic analyses. The safety profile in pediatric patients was similar to that observed in adults [see Adverse Reactions (6.1), Clinical Pharmacology (12.3), Clinical Studies (14.2)].
The safety and effectiveness of mesalamine delayed-release tablets have not been established in patients weighing less than 24 kg.
8.5 Geriatric Use
Clinical trials of mesalamine delayed-release tablets did not include sufficient numbers of patients aged 65 years and over to determine whether they respond differently from younger patients. Reports from uncontrolled clinical studies and postmarketing reporting systems suggested a higher incidence of blood dyscrasias (i.e., agranulocytosis, neutropenia, and pancytopenia) in patients who were 65 years or older who were taking mesalamine-containing products such as mesalamine delayed-release tablets compared to younger patients. Monitor complete blood cell counts and platelet counts in elderly patients during treatment with mesalamine delayed-release tablets.
Systemic exposures are increased in elderly subjects [see Clinical Pharmacology (12.3)].
In general, consider the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy in elderly patients when prescribing mesalamine delayed-release tablets. Consider starting at the low end of the dosing range for induction in elderly patients [see Dosage and Administration (2), Use in Specific Populations (8.6)].
4 Contraindications
Mesalamine delayed-release tablets are contraindicated in patients with known or suspected hypersensitivity to salicylates, aminosalicylates, or to any of the ingredients of mesalamine delayed-release tablets [see Warnings and Precautions (5.3), Adverse Reactions (6.2), Description (11)].
5.4 Hepatic Failure
There have been reports of hepatic failure in patients with pre-existing liver disease who have been administered mesalamine. Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known liver impairment.
5.8 Nephrolithiasis
Cases of nephrolithiasis have been reported with the use of mesalamine, including stones with a 100% mesalamine content. Mesalamine-containing stones are radiotransparent and undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment with mesalamine delayed-release tablets.
6 Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in labeling:
- Renal impairment, including renal failure [see Warnings and Precautions (5.1)]
- Mesalamine-induced acute intolerance syndrome [see Warnings and Precautions (5.2)]
- Hypersensitivity reactions [see Warnings and Precautions (5.3)]
- Hepatic failure [see Warnings and Precautions (5.4)]
- Severe cutaneous adverse reactions [see Warnings and Precautions (5.5)]
- Upper gastrointestinal tract obstruction [see Warnings and Precautions (5.6)]
- Photosensitivity [see Warnings and Precautions (5.7)]
- Nephrolithiasis [see Warnings and Precautions (5.8)]
7 Drug Interactions
5.1 Renal Impairment
Renal impairment, including minimal change disease, acute and chronic interstitial nephritis, and, rarely, renal failure, has been reported in patients given products such as mesalamine that contain mesalamine or are converted to mesalamine. In animal studies, the kidney was the principal organ of mesalamine toxicity [see Adverse Reactions (6.2), Nonclinical Toxicology (13.2)].
Evaluate renal function prior to initiation of mesalamine delayed-release tablets therapy and periodically while on therapy. Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known renal impairment, history of renal disease, or taking concomitant nephrotoxic drugs. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy [see Drug Interactions (7.1), Use in Specific Populations (8.6)].
5.7 Photosensitivity
Patients with pre-existing skin conditions such as atopic dermatitis and atopic eczema have reported more severe photosensitivity reactions. Advise patients to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors.
8.6 Renal Impairment
Mesalamine is known to be substantially excreted by the kidney, and the risk of toxic reactions may be greater in patients with impaired renal function. Evaluate renal function in all patients prior to initiation and periodically while on mesalamine delayed-release tablets therapy. Monitor patients with known renal impairment or history of renal disease or taking nephrotoxic drugs for decreased renal function and mesalamine-related adverse reactions. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy [see Warnings and Precautions (5.1), Adverse Reactions (6.2), Drug Interactions (7.1)].
1 Indications and Usage
Mesalamine delayed-release tablets are indicated for the:
- induction and maintenance of remission in adult patients with mildly to moderately active ulcerative colitis.
- treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg.
12.1 Mechanism of Action
The mechanism of action of mesalamine is not fully understood, but it appears to have a topical anti-inflammatory effect on the colonic epithelial cells. Mucosal production of arachidonic acid metabolites, both through the cyclooxygenase and lipoxygenase pathways, is increased in patients with ulcerative colitis, and it is possible that mesalamine diminishes inflammation by blocking cyclooxygenase and inhibiting prostaglandin production in the colon.
5 Warnings and Precautions
- Renal Impairment: Assess renal function at the beginning of treatment and periodically during treatment. Evaluate the risks and benefits of mesalamine delayed-release tablets in patients with known renal impairment or taking nephrotoxic drugs. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy. (5.1, 7.1, 8.6)
- Mesalamine-Induced Acute Intolerance Syndrome: Symptoms may be difficult to distinguish from an ulcerative colitis exacerbation. Monitor for worsening symptoms while on treatment. Discontinue treatment if acute intolerance syndrome is suspected. (5.2)
- Hypersensitivity Reactions, including myocarditis and pericarditis: Evaluate patients immediately and discontinue mesalamine delayed-release tablets if a hypersensitivity reaction is suspected. (5.3)
- Hepatic Failure: Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known liver impairment. (5.4)
- Severe Cutaneous Adverse Reactions: Discontinue at the first signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation. (5.5)
- Upper Gastrointestinal Tract Obstruction: Avoid in patients with pyloric stenosis or other organic or functional obstruction. (5.6)
- Photosensitivity: Advise patients with pre-existing skin conditions to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors. (5.7)
- Nephrolithiasis: Cases of nephrolithiasis have been reported with the use of mesalamine. Mesalamine-containing stones are undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment. (5.8)
- Interference With Laboratory Tests: Use of mesalamine may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection. (5.9)
2 Dosage and Administration
Administration Instructions
- Evaluate renal function prior to initiation of mesalamine delayed-release tablets and periodically while on therapy. (2, 5.1)
- Swallow mesalamine delayed-release tablets whole; do not split or crush. (2)
- Administer mesalamine delayed-release tablets with food. (2)
- Drink an adequate amount of fluids. (2, 5.8)
Recommended Dosage in Adults
- For induction of remission: 2.4 g to 4.8 g (two to four 1.2-g tablets) once daily. (2)
- For maintenance of remission: 2.4 g (two 1.2-g tablets) once daily. (2)
Recommended Dosage in Pediatric Patients
- The recommended dosage for treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg who can swallow tablets whole is shown below: (2)
| Weight of Pediatric Patient | Once Daily Mesalamine delayed-release tablets Dosage | |
|---|---|---|
| Week 0 to Week 8 | After Week 8 | |
| 24 kg to 35 kg | 2.4 g (two 1.2-g tablets) |
1.2 g (one 1.2-g tablet) |
| Greater than 35 kg to 50 kg | 3.6 g (three 1.2-g tablets) |
2.4 g (two 1.2-g tablets) |
| Greater than 50 kg | 4.8 g (four 1.2-g tablets) |
2.4 g (two 1.2-g tablets) |
3 Dosage Forms and Strengths
The red-brown ellipsoidal delayed-release tablet containing 1.2 g mesalamine is debossed on one side and imprinted with S476.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of mesalamine delayed-release tablets or other mesalamine-containing products. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Body as a Whole: lupus-like syndrome, drug fever
Cardiac Disorders: pericarditis, pericardial effusion, myocarditis [see Warnings and Precautions (5.3)]
Gastrointestinal: cholecystitis, gastritis, gastroenteritis, gastrointestinal bleeding, perforated peptic ulcer
Hepatic: jaundice, cholestatic jaundice, hepatitis, liver necrosis, liver failure, hepatotoxicity, Kawasaki-like syndrome including changes in liver enzymes
Hematologic: agranulocytosis, aplastic anemia
Immune System Disorders: anaphylactic reaction, angioedema
Musculoskeletal and Connective Tissue Disorders: myalgia, lupus-like syndrome
Neurological/Psychiatric: peripheral neuropathy, Guillain-Barré syndrome, transverse myelitis, intracranial hypertension
Renal Disorders: renal failure, interstitial nephritis, nephrogenic diabetes insipidus, nephrolithiasis [see Warnings and Precautions (5.1, 5.8)]
- Urine discoloration occurring ex-vivo caused by contact of mesalamine, including inactive metabolite, with surfaces or water treated with hypochlorite-containing bleach
Respiratory, Thoracic and Mediastinal Disorders: interstitial lung disease, hypersensitivity pneumonitis (including interstitial pneumonitis, allergic alveolitis, eosinophilic pneumonitis), pleurisy/pleuritis
Skin: psoriasis, pyoderma gangrenosum, erythema nodosum, photosensitivity, SJS/TEN, DRESS, and AGEP [ see Warnings and Precautions (5.5)]
Urogenital: reversible oligospermia
8 Use in Specific Populations
Geriatric Patients: Increased risk of blood dyscrasias; monitor complete blood cell counts and platelet counts. (8.5)
5.3 Hypersensitivity Reactions
Hypersensitivity reactions have been reported in patients taking sulfasalazine. Some of these patients may have a similar reaction to mesalamine delayed-release tablets or to other compounds that contain or are converted to mesalamine.
As with sulfasalazine, mesalamine-induced hypersensitivity reactions may present as internal organ involvement, including myocarditis, pericarditis, nephritis, hepatitis, pneumonitis, and hematologic abnormalities. Evaluate patients immediately if signs or symptoms of a hypersensitivity reaction are present. Discontinue mesalamine delayed-release tablets if an alternative etiology for the signs or symptoms cannot be established.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
16 How Supplied/storage and Handling
Mesalamine delayed-release tablets are available as red-brown, ellipsoidal, film-coated delayed-release tablets containing 1.2 g mesalamine, and debossed on one side imprinted with S476.
NDC 54092-100-01 HDPE Bottle with a child-resistant closure of 120 delayed-release tablets.
7.2 Azathioprine and 6 Mercaptopurine
The concurrent use of mesalamine with azathioprine or 6-mercaptopurine and/or any other drugs known to cause myelotoxicity may increase the risk for blood disorders, bone marrow failure, and associated complications. If concomitant use of mesalamine delayed-release tablets and azathioprine or 6-mercaptopurine cannot be avoided, monitor blood tests, including complete blood cell counts and platelet counts.
5.5 Severe Cutaneous Adverse Reactions
Severe cutaneous adverse reactions, such as Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS), and acute generalized exanthematous pustulosis (AGEP) have been reported with the use of mesalamine [see Adverse Reactions (6.2)]. Discontinue mesalamine delayed-release tablets at the first appearance of signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation.
5.9 Interference With Laboratory Tests
Use of mesalamine delayed-release tablets may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection because of the similarity in the chromatograms of normetanephrine and the main metabolite of mesalamine, N-acetyl-5-aminosalicylic acid (N-Ac-5-ASA). Consider an alternative, selective assay for normetanephrine.
13.2 Animal Toxicology And/or Pharmacology
In animal studies with mesalamine, a 13-week oral toxicity study in mice and 13-week and 52-week oral toxicity studies in rats and cynomolgus monkeys have shown the kidney to be the major target organ of mesalamine toxicity. Oral daily doses of 2400 mg/kg in mice and 1150 mg/kg in rats produced renal lesions including granular and hyaline casts, tubular degeneration, tubular dilation, renal infarct, papillary necrosis, tubular necrosis, and interstitial nephritis. In cynomolgus monkeys, oral daily doses of 250 mg/kg or higher produced nephrosis, papillary edema, and interstitial fibrosis.
5.6 Upper Gastrointestinal Tract Obstruction
Pyloric stenosis or other organic or functional obstruction in the upper gastrointestinal tract may cause prolonged gastric retention of mesalamine delayed-release tablets, which would delay mesalamine release in the colon. Avoid mesalamine delayed-release tablets in patients at risk of upper gastrointestinal tract obstruction.
5.2 Mesalamine Induced Acute Intolerance Syndrome
Mesalamine has been associated with an acute intolerance syndrome that may be difficult to distinguish from an exacerbation of ulcerative colitis. Although the exact frequency of occurrence has not been determined, it has occurred in 3% of patients in controlled clinical trials of mesalamine or sulfasalazine. Symptoms include cramping, acute abdominal pain and bloody diarrhea, and sometimes fever, headache, and rash. Monitor patients closely for worsening of these symptoms while on treatment. If acute intolerance syndrome is suspected, promptly discontinue treatment with mesalamine delayed-release tablets.
Principal Display Panel 1.2 G Tablet Bottle Label
ONCE-DAILY
NDC 54092-100-01
Mesalamine
delayed-release
tablets
1.2 g per tablet
Rx Only
120 Tablets
Takeda
7.3 Interference With Urinary Normetanephrine Measurements
Use of mesalamine delayed-release tablets may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection [see Warnings and Precautions (5.9)]. Consider an alternative, selective assay for normetanephrine.
7.1 Nephrotoxic Agents, Including Non Steroidal Anti Inflammatory Drugs
The concurrent use of mesalamine with known nephrotoxic agents, including non-steroidal anti-inflammatory drugs (NSAIDs), may increase the risk of nephrotoxicity. Monitor patients taking nephrotoxic drugs for changes in renal function and mesalamine-related adverse reactions [see Warnings and Precautions (5.1)].
14.2 Pediatric Patients With Mildly to Moderately Active Ulcerative Colitis Weighing At Least 24 Kg
A multicenter, randomized, double-blind, parallel-group study (NCT02093663) was conducted in pediatric patients aged 5 through 17 years with mildly to moderately active ulcerative colitis to determine the safety and effectiveness of mesalamine delayed-release tablets. The study consisted of two treatment phases, an initial 8-week phase and a 26-week phase. The overall population consisted of 105 patients, of whom 27 patients participated in both the 8-week and 26-week phases.
Each phase included two dosage arms and patients were randomized at the beginning of each phase in a 1:1 ratio, stratified by body weight group. Patients received a low or a high weight-based dosage of mesalamine delayed-release tablets in four weight groups. Because of the small number of patients in the lowest body weight group (0 in the 8-week phase and 3 in the 26-week phase), the safety and effectiveness of mesalamine delayed-release tablets in patients weighing less than 24 kg have not been established.
Patients were eligible for the initial 8-week phase if they had mildly to moderately active ulcerative colitis as defined by the UC-DAI score of at least 4 with an endoscopic subscore of 2 or 3.
In the 53 patients enrolled in the initial phase, the mean age and weight of patients was 14 years and 53 kg, the mean (SD) baseline UC-DAI score was 5.8 (1.8), 93% were white, and 59% were male. The primary endpoint was defined by the partial UC-DAI less than or equal to 1 (with rectal bleeding equal to 0, stool frequency less than or equal to 1, and Physician's Global Assessment [PGA] equal to 0). Of the 26 patients in the recommended mesalamine delayed-release tablets dosage arm, 65% achieved the primary endpoint after 8 weeks of treatment. During the initial 8-week phase, fewer patients who received the recommended mesalamine delayed-release tablets dosage were discontinued from the study due to ulcerative colitis (0/26, 0%) compared to patients who received a lower than recommended mesalamine delayed-release tablets dosage (8/27, 30%).
Patients who met the primary endpoint at 8 weeks were eligible to continue treatment in the 26-week phase. Patients were also eligible to enter the 26-week phase without having participated in the 8-week phase if they had a UC-DAI score of less than or equal to 2 with an endoscopic subscore of 0 or 1 (modified to exclude friability).
There were 87 patients enrolled in the 26-week phase. The mean age and weight of patients were 14 years and 54 kg; 97% were white and 55% were female. Of the 42 patients in the recommended mesalamine delayed-release tablets dosage arm, 55% achieved the primary endpoint, which was defined the same as in the 8-week phase. In the 26-week phase, the arm with a higher than recommended mesalamine delayed-release tablets dosage was not more effective and is not recommended [see Dosage and Administration (2)].
Structured Label Content
Section 42229-5 (42229-5)
Administration Instructions
- Evaluate renal function prior to initiation of mesalamine delayed-release tablets and periodically while on therapy.
- Swallow mesalamine delayed-release tablets whole; do not split or crush.
- Administer mesalamine delayed-release tablets with food [see Clinical Pharmacology (12.3)].
- Drink an adequate amount of fluids [see Warnings and Precautions (5.8)].
Section 43683-2 (43683-2)
| Warnings and Precautions, Renal Impairment (5.1) | 11/2022 |
Section 44425-7 (44425-7)
Store at room temperature 15°C to 25°C (59°F to 77°F); excursions permitted to 30°C (86°F).
See USP Controlled Room Temperature.
10 Overdosage (10 OVERDOSAGE)
Mesalamine delayed-release tablets are an aminosalicylate, and symptoms of salicylate toxicity may include nausea, vomiting, abdominal pain, tachypnea, hyperpnea, tinnitus, and neurologic symptoms (headache, dizziness, confusion, seizures). Severe intoxication with salicylates may lead to electrolyte and blood pH imbalance, and potentially end organ (e.g., renal and liver) damage.
There is no specific known antidote for mesalamine overdose; however, conventional therapy for salicylate toxicity may be beneficial in the event of acute overdosage and may include gastrointestinal tract decontamination to prevent further absorption. Correct fluid and electrolyte imbalance by the administration of appropriate intravenous therapy and maintain adequate renal function.
Mesalamine delayed-release tablets are a pH-dependent, delayed-release product and this factor should be considered when treating a suspected overdose.
11 Description (11 DESCRIPTION)
Each mesalamine delayed-release tablet for oral administration contains 1.2 g 5-aminosalicylic acid (5-ASA; mesalamine), an anti-inflammatory agent. Mesalamine also has the chemical name 5-amino-2-hydroxybenzoic acid and its structural formula is:
| Molecular formula: | C7H7NO3 |
| Molecular weight: | 153.14 |
The tablet is coated with a pH-dependent polymer film, which breaks down at or above pH 6.8, normally in the terminal ileum where mesalamine then begins to be released from the tablet core. The tablet core contains mesalamine with hydrophilic and lipophilic excipients and provides for extended release of mesalamine.
The inactive ingredients of a mesalamine delayed-release tablet are sodium carboxymethylcellulose, carnauba wax, stearic acid, silica (colloidal hydrated), sodium starch glycolate (type A), talc, magnesium stearate, methacrylic acid copolymer types A and B, triethylcitrate, titanium dioxide, red ferric oxide, and polyethylene glycol 6000.
8.4 Pediatric Use
The safety and effectiveness of mesalamine delayed-release tablets have been established for the treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg. Use of mesalamine delayed-release tablets in this population is supported by evidence from adequate and well-controlled trials in adults, a multicenter, randomized, double-blind, parallel group trial in 105 pediatric patients 5 to 17 years of age, and additional pharmacokinetic analyses. The safety profile in pediatric patients was similar to that observed in adults [see Adverse Reactions (6.1), Clinical Pharmacology (12.3), Clinical Studies (14.2)].
The safety and effectiveness of mesalamine delayed-release tablets have not been established in patients weighing less than 24 kg.
8.5 Geriatric Use
Clinical trials of mesalamine delayed-release tablets did not include sufficient numbers of patients aged 65 years and over to determine whether they respond differently from younger patients. Reports from uncontrolled clinical studies and postmarketing reporting systems suggested a higher incidence of blood dyscrasias (i.e., agranulocytosis, neutropenia, and pancytopenia) in patients who were 65 years or older who were taking mesalamine-containing products such as mesalamine delayed-release tablets compared to younger patients. Monitor complete blood cell counts and platelet counts in elderly patients during treatment with mesalamine delayed-release tablets.
Systemic exposures are increased in elderly subjects [see Clinical Pharmacology (12.3)].
In general, consider the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy in elderly patients when prescribing mesalamine delayed-release tablets. Consider starting at the low end of the dosing range for induction in elderly patients [see Dosage and Administration (2), Use in Specific Populations (8.6)].
4 Contraindications (4 CONTRAINDICATIONS)
Mesalamine delayed-release tablets are contraindicated in patients with known or suspected hypersensitivity to salicylates, aminosalicylates, or to any of the ingredients of mesalamine delayed-release tablets [see Warnings and Precautions (5.3), Adverse Reactions (6.2), Description (11)].
5.4 Hepatic Failure
There have been reports of hepatic failure in patients with pre-existing liver disease who have been administered mesalamine. Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known liver impairment.
5.8 Nephrolithiasis
Cases of nephrolithiasis have been reported with the use of mesalamine, including stones with a 100% mesalamine content. Mesalamine-containing stones are radiotransparent and undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment with mesalamine delayed-release tablets.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are described elsewhere in labeling:
- Renal impairment, including renal failure [see Warnings and Precautions (5.1)]
- Mesalamine-induced acute intolerance syndrome [see Warnings and Precautions (5.2)]
- Hypersensitivity reactions [see Warnings and Precautions (5.3)]
- Hepatic failure [see Warnings and Precautions (5.4)]
- Severe cutaneous adverse reactions [see Warnings and Precautions (5.5)]
- Upper gastrointestinal tract obstruction [see Warnings and Precautions (5.6)]
- Photosensitivity [see Warnings and Precautions (5.7)]
- Nephrolithiasis [see Warnings and Precautions (5.8)]
7 Drug Interactions (7 DRUG INTERACTIONS)
5.1 Renal Impairment
Renal impairment, including minimal change disease, acute and chronic interstitial nephritis, and, rarely, renal failure, has been reported in patients given products such as mesalamine that contain mesalamine or are converted to mesalamine. In animal studies, the kidney was the principal organ of mesalamine toxicity [see Adverse Reactions (6.2), Nonclinical Toxicology (13.2)].
Evaluate renal function prior to initiation of mesalamine delayed-release tablets therapy and periodically while on therapy. Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known renal impairment, history of renal disease, or taking concomitant nephrotoxic drugs. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy [see Drug Interactions (7.1), Use in Specific Populations (8.6)].
5.7 Photosensitivity
Patients with pre-existing skin conditions such as atopic dermatitis and atopic eczema have reported more severe photosensitivity reactions. Advise patients to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors.
8.6 Renal Impairment
Mesalamine is known to be substantially excreted by the kidney, and the risk of toxic reactions may be greater in patients with impaired renal function. Evaluate renal function in all patients prior to initiation and periodically while on mesalamine delayed-release tablets therapy. Monitor patients with known renal impairment or history of renal disease or taking nephrotoxic drugs for decreased renal function and mesalamine-related adverse reactions. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy [see Warnings and Precautions (5.1), Adverse Reactions (6.2), Drug Interactions (7.1)].
1 Indications and Usage (1 INDICATIONS AND USAGE)
Mesalamine delayed-release tablets are indicated for the:
- induction and maintenance of remission in adult patients with mildly to moderately active ulcerative colitis.
- treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg.
12.1 Mechanism of Action
The mechanism of action of mesalamine is not fully understood, but it appears to have a topical anti-inflammatory effect on the colonic epithelial cells. Mucosal production of arachidonic acid metabolites, both through the cyclooxygenase and lipoxygenase pathways, is increased in patients with ulcerative colitis, and it is possible that mesalamine diminishes inflammation by blocking cyclooxygenase and inhibiting prostaglandin production in the colon.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Renal Impairment: Assess renal function at the beginning of treatment and periodically during treatment. Evaluate the risks and benefits of mesalamine delayed-release tablets in patients with known renal impairment or taking nephrotoxic drugs. Discontinue mesalamine delayed-release tablets if renal function deteriorates while on therapy. (5.1, 7.1, 8.6)
- Mesalamine-Induced Acute Intolerance Syndrome: Symptoms may be difficult to distinguish from an ulcerative colitis exacerbation. Monitor for worsening symptoms while on treatment. Discontinue treatment if acute intolerance syndrome is suspected. (5.2)
- Hypersensitivity Reactions, including myocarditis and pericarditis: Evaluate patients immediately and discontinue mesalamine delayed-release tablets if a hypersensitivity reaction is suspected. (5.3)
- Hepatic Failure: Evaluate the risks and benefits of using mesalamine delayed-release tablets in patients with known liver impairment. (5.4)
- Severe Cutaneous Adverse Reactions: Discontinue at the first signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation. (5.5)
- Upper Gastrointestinal Tract Obstruction: Avoid in patients with pyloric stenosis or other organic or functional obstruction. (5.6)
- Photosensitivity: Advise patients with pre-existing skin conditions to avoid sun exposure, wear protective clothing, and use a broad-spectrum sunscreen when outdoors. (5.7)
- Nephrolithiasis: Cases of nephrolithiasis have been reported with the use of mesalamine. Mesalamine-containing stones are undetectable by standard radiography or computed tomography (CT). Ensure adequate hydration during treatment. (5.8)
- Interference With Laboratory Tests: Use of mesalamine may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection. (5.9)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
Administration Instructions
- Evaluate renal function prior to initiation of mesalamine delayed-release tablets and periodically while on therapy. (2, 5.1)
- Swallow mesalamine delayed-release tablets whole; do not split or crush. (2)
- Administer mesalamine delayed-release tablets with food. (2)
- Drink an adequate amount of fluids. (2, 5.8)
Recommended Dosage in Adults
- For induction of remission: 2.4 g to 4.8 g (two to four 1.2-g tablets) once daily. (2)
- For maintenance of remission: 2.4 g (two 1.2-g tablets) once daily. (2)
Recommended Dosage in Pediatric Patients
- The recommended dosage for treatment of mildly to moderately active ulcerative colitis in pediatric patients weighing at least 24 kg who can swallow tablets whole is shown below: (2)
| Weight of Pediatric Patient | Once Daily Mesalamine delayed-release tablets Dosage | |
|---|---|---|
| Week 0 to Week 8 | After Week 8 | |
| 24 kg to 35 kg | 2.4 g (two 1.2-g tablets) |
1.2 g (one 1.2-g tablet) |
| Greater than 35 kg to 50 kg | 3.6 g (three 1.2-g tablets) |
2.4 g (two 1.2-g tablets) |
| Greater than 50 kg | 4.8 g (four 1.2-g tablets) |
2.4 g (two 1.2-g tablets) |
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
The red-brown ellipsoidal delayed-release tablet containing 1.2 g mesalamine is debossed on one side and imprinted with S476.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of mesalamine delayed-release tablets or other mesalamine-containing products. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Body as a Whole: lupus-like syndrome, drug fever
Cardiac Disorders: pericarditis, pericardial effusion, myocarditis [see Warnings and Precautions (5.3)]
Gastrointestinal: cholecystitis, gastritis, gastroenteritis, gastrointestinal bleeding, perforated peptic ulcer
Hepatic: jaundice, cholestatic jaundice, hepatitis, liver necrosis, liver failure, hepatotoxicity, Kawasaki-like syndrome including changes in liver enzymes
Hematologic: agranulocytosis, aplastic anemia
Immune System Disorders: anaphylactic reaction, angioedema
Musculoskeletal and Connective Tissue Disorders: myalgia, lupus-like syndrome
Neurological/Psychiatric: peripheral neuropathy, Guillain-Barré syndrome, transverse myelitis, intracranial hypertension
Renal Disorders: renal failure, interstitial nephritis, nephrogenic diabetes insipidus, nephrolithiasis [see Warnings and Precautions (5.1, 5.8)]
- Urine discoloration occurring ex-vivo caused by contact of mesalamine, including inactive metabolite, with surfaces or water treated with hypochlorite-containing bleach
Respiratory, Thoracic and Mediastinal Disorders: interstitial lung disease, hypersensitivity pneumonitis (including interstitial pneumonitis, allergic alveolitis, eosinophilic pneumonitis), pleurisy/pleuritis
Skin: psoriasis, pyoderma gangrenosum, erythema nodosum, photosensitivity, SJS/TEN, DRESS, and AGEP [ see Warnings and Precautions (5.5)]
Urogenital: reversible oligospermia
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
Geriatric Patients: Increased risk of blood dyscrasias; monitor complete blood cell counts and platelet counts. (8.5)
5.3 Hypersensitivity Reactions
Hypersensitivity reactions have been reported in patients taking sulfasalazine. Some of these patients may have a similar reaction to mesalamine delayed-release tablets or to other compounds that contain or are converted to mesalamine.
As with sulfasalazine, mesalamine-induced hypersensitivity reactions may present as internal organ involvement, including myocarditis, pericarditis, nephritis, hepatitis, pneumonitis, and hematologic abnormalities. Evaluate patients immediately if signs or symptoms of a hypersensitivity reaction are present. Discontinue mesalamine delayed-release tablets if an alternative etiology for the signs or symptoms cannot be established.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
Mesalamine delayed-release tablets are available as red-brown, ellipsoidal, film-coated delayed-release tablets containing 1.2 g mesalamine, and debossed on one side imprinted with S476.
NDC 54092-100-01 HDPE Bottle with a child-resistant closure of 120 delayed-release tablets.
7.2 Azathioprine and 6 Mercaptopurine (7.2 Azathioprine and 6-Mercaptopurine)
The concurrent use of mesalamine with azathioprine or 6-mercaptopurine and/or any other drugs known to cause myelotoxicity may increase the risk for blood disorders, bone marrow failure, and associated complications. If concomitant use of mesalamine delayed-release tablets and azathioprine or 6-mercaptopurine cannot be avoided, monitor blood tests, including complete blood cell counts and platelet counts.
5.5 Severe Cutaneous Adverse Reactions
Severe cutaneous adverse reactions, such as Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS), and acute generalized exanthematous pustulosis (AGEP) have been reported with the use of mesalamine [see Adverse Reactions (6.2)]. Discontinue mesalamine delayed-release tablets at the first appearance of signs or symptoms of severe cutaneous adverse reactions or other signs of hypersensitivity and consider further evaluation.
5.9 Interference With Laboratory Tests (5.9 Interference with Laboratory Tests)
Use of mesalamine delayed-release tablets may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection because of the similarity in the chromatograms of normetanephrine and the main metabolite of mesalamine, N-acetyl-5-aminosalicylic acid (N-Ac-5-ASA). Consider an alternative, selective assay for normetanephrine.
13.2 Animal Toxicology And/or Pharmacology (13.2 Animal Toxicology and/or Pharmacology)
In animal studies with mesalamine, a 13-week oral toxicity study in mice and 13-week and 52-week oral toxicity studies in rats and cynomolgus monkeys have shown the kidney to be the major target organ of mesalamine toxicity. Oral daily doses of 2400 mg/kg in mice and 1150 mg/kg in rats produced renal lesions including granular and hyaline casts, tubular degeneration, tubular dilation, renal infarct, papillary necrosis, tubular necrosis, and interstitial nephritis. In cynomolgus monkeys, oral daily doses of 250 mg/kg or higher produced nephrosis, papillary edema, and interstitial fibrosis.
5.6 Upper Gastrointestinal Tract Obstruction
Pyloric stenosis or other organic or functional obstruction in the upper gastrointestinal tract may cause prolonged gastric retention of mesalamine delayed-release tablets, which would delay mesalamine release in the colon. Avoid mesalamine delayed-release tablets in patients at risk of upper gastrointestinal tract obstruction.
5.2 Mesalamine Induced Acute Intolerance Syndrome (5.2 Mesalamine-Induced Acute Intolerance Syndrome)
Mesalamine has been associated with an acute intolerance syndrome that may be difficult to distinguish from an exacerbation of ulcerative colitis. Although the exact frequency of occurrence has not been determined, it has occurred in 3% of patients in controlled clinical trials of mesalamine or sulfasalazine. Symptoms include cramping, acute abdominal pain and bloody diarrhea, and sometimes fever, headache, and rash. Monitor patients closely for worsening of these symptoms while on treatment. If acute intolerance syndrome is suspected, promptly discontinue treatment with mesalamine delayed-release tablets.
Principal Display Panel 1.2 G Tablet Bottle Label (PRINCIPAL DISPLAY PANEL - 1.2 g Tablet Bottle Label)
ONCE-DAILY
NDC 54092-100-01
Mesalamine
delayed-release
tablets
1.2 g per tablet
Rx Only
120 Tablets
Takeda
7.3 Interference With Urinary Normetanephrine Measurements (7.3 Interference with Urinary Normetanephrine Measurements)
Use of mesalamine delayed-release tablets may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection [see Warnings and Precautions (5.9)]. Consider an alternative, selective assay for normetanephrine.
7.1 Nephrotoxic Agents, Including Non Steroidal Anti Inflammatory Drugs (7.1 Nephrotoxic Agents, Including Non-Steroidal Anti-Inflammatory Drugs)
The concurrent use of mesalamine with known nephrotoxic agents, including non-steroidal anti-inflammatory drugs (NSAIDs), may increase the risk of nephrotoxicity. Monitor patients taking nephrotoxic drugs for changes in renal function and mesalamine-related adverse reactions [see Warnings and Precautions (5.1)].
14.2 Pediatric Patients With Mildly to Moderately Active Ulcerative Colitis Weighing At Least 24 Kg (14.2 Pediatric Patients with Mildly to Moderately Active Ulcerative Colitis Weighing at Least 24 kg)
A multicenter, randomized, double-blind, parallel-group study (NCT02093663) was conducted in pediatric patients aged 5 through 17 years with mildly to moderately active ulcerative colitis to determine the safety and effectiveness of mesalamine delayed-release tablets. The study consisted of two treatment phases, an initial 8-week phase and a 26-week phase. The overall population consisted of 105 patients, of whom 27 patients participated in both the 8-week and 26-week phases.
Each phase included two dosage arms and patients were randomized at the beginning of each phase in a 1:1 ratio, stratified by body weight group. Patients received a low or a high weight-based dosage of mesalamine delayed-release tablets in four weight groups. Because of the small number of patients in the lowest body weight group (0 in the 8-week phase and 3 in the 26-week phase), the safety and effectiveness of mesalamine delayed-release tablets in patients weighing less than 24 kg have not been established.
Patients were eligible for the initial 8-week phase if they had mildly to moderately active ulcerative colitis as defined by the UC-DAI score of at least 4 with an endoscopic subscore of 2 or 3.
In the 53 patients enrolled in the initial phase, the mean age and weight of patients was 14 years and 53 kg, the mean (SD) baseline UC-DAI score was 5.8 (1.8), 93% were white, and 59% were male. The primary endpoint was defined by the partial UC-DAI less than or equal to 1 (with rectal bleeding equal to 0, stool frequency less than or equal to 1, and Physician's Global Assessment [PGA] equal to 0). Of the 26 patients in the recommended mesalamine delayed-release tablets dosage arm, 65% achieved the primary endpoint after 8 weeks of treatment. During the initial 8-week phase, fewer patients who received the recommended mesalamine delayed-release tablets dosage were discontinued from the study due to ulcerative colitis (0/26, 0%) compared to patients who received a lower than recommended mesalamine delayed-release tablets dosage (8/27, 30%).
Patients who met the primary endpoint at 8 weeks were eligible to continue treatment in the 26-week phase. Patients were also eligible to enter the 26-week phase without having participated in the 8-week phase if they had a UC-DAI score of less than or equal to 2 with an endoscopic subscore of 0 or 1 (modified to exclude friability).
There were 87 patients enrolled in the 26-week phase. The mean age and weight of patients were 14 years and 54 kg; 97% were white and 55% were female. Of the 42 patients in the recommended mesalamine delayed-release tablets dosage arm, 55% achieved the primary endpoint, which was defined the same as in the 8-week phase. In the 26-week phase, the arm with a higher than recommended mesalamine delayed-release tablets dosage was not more effective and is not recommended [see Dosage and Administration (2)].
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:44:51.290480 · Updated: 2026-03-14T22:21:24.209091