These Highlights Do Not Include All The Information Needed To Use Nexlizet®
3fa2108c-0300-47b8-9d34-f762af7c93c6
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
NEXLIZET, a combination of bempedoic acid and ezetimibe, is indicated: as an adjunct to diet and exercise to reduce LDL-C in adults with hypercholesterolemia, including heterozygous familial hypercholesterolemia (HeFH). Bempedoic acid, a component of NEXLIZET, is indicated: to reduce the risk of major adverse cardiovascular events (cardiovascular death, myocardial infarction, stroke, or coronary revascularization) in adults at increased risk for these events who are unable to take recommended statin therapy (including those not taking a statin).
Dosage and Administration
Administer one tablet (180 mg bempedoic acid and 10 mg ezetimibe) orally once daily with or without food. ( 2.1 ) Swallow the tablet whole. ( 2.1 ) Coadministration with Bile Acid Sequestrants: Administer at least 2 hours before or at least 4 hours after bile acid sequestrants. ( 2.2 )
Contraindications
NEXLIZET is contraindicated in patients with a prior hypersensitivity to ezetimibe or bempedoic acid or any of the excipients in NEXLIZET [see Adverse Reactions (6.2) ] . Serious hypersensitivity reactions, such as anaphylaxis, angioedema, rash and urticaria have been reported with ezetimibe or bempedoic acid.
Warnings and Precautions
Hyperuricemia: Elevations in serum uric acid have occurred. Assess uric acid levels periodically as clinically indicated. Monitor for signs and symptoms of hyperuricemia, and initiate treatment with urate-lowering drugs as appropriate. ( 5.1 ) Tendon Rupture: Tendon rupture has occurred. Discontinue NEXLIZET at the first sign of tendon rupture. Avoid NEXLIZET in patients who have a history of tendon disorders or tendon rupture. ( 5.2 )
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: Hyperuricemia [see Warnings and Precautions (5.1) ] Tendon Rupture [see Warnings and Precautions (5.2) ]
Drug Interactions
No specific pharmacokinetic drug interaction studies with NEXLIZET have been conducted. Table 4 lists drug interactions with NEXLIZET that have been identified in studies with bempedoic acid or ezetimibe. Table 4. Clinically Important Drug Interactions with NEXLIZET Simvastatin Clinical Impact: Concomitant use of NEXLIZET with simvastatin causes an increase in simvastatin concentration and may increase the risk of simvastatin-related myopathy [see Clinical Pharmacology (12.3) ] . Intervention: Avoid concomitant use of NEXLIZET with simvastatin greater than 20 mg. Pravastatin Clinical Impact: Concomitant use of NEXLIZET with pravastatin causes an increase in pravastatin concentration and may increase the risk of pravastatin-related myopathy [see Clinical Pharmacology (12.3) ] . Intervention: Avoid concomitant use of NEXLIZET with pravastatin greater than 40 mg. Cyclosporine Clinical Impact: Concomitant use of NEXLIZET and cyclosporine increases ezetimibe and cyclosporine concentrations. The degree of increase in ezetimibe exposure may be greater in patients with severe renal insufficiency [see Clinical Pharmacology (12.3) ] . Intervention: Monitor cyclosporine concentrations in patients receiving NEXLIZET and cyclosporine. In patients treated with cyclosporine, weigh the potential effects of the increased exposure to ezetimibe from concomitant use against the benefits of alterations in lipid levels provided by NEXLIZET. Fibrates Clinical Impact: Both fenofibrate and ezetimibe (a component of NEXLIZET) may increase cholesterol excretion into the bile, leading to cholelithiasis. Coadministration of NEXLIZET with fibrates other than fenofibrate is not recommended [see Adverse Reactions (6.1) ] . Intervention: If cholelithiasis is suspected in a patient receiving NEXLIZET and fenofibrate, gallbladder studies are indicated and alternative lipid-lowering therapy should be considered. Clinical Impact: Concomitant administration of fibrates with bempedoic acid (a component of NEXLIZET) resulted in increased triglycerides and decreased high-density lipoprotein cholesterol (HDL-C) in some patients in clinical studies and post-marketing reports. Reversibility of both increased triglycerides and decreased HDL-C levels was observed when either bempedoic acid or fibrate therapy was discontinued. Intervention: Monitor triglycerides and HDL-C four weeks after initial concomitant use of NEXLIZET and a fibrate and periodically thereafter. If increased triglycerides or decreased HDL-C levels are detected, discontinue NEXLIZET or fibrate therapy based on clinical judgment. Monitor triglycerides and HDL-C levels until levels return to baseline. Cholestyramine Clinical Impact: Concomitant use of NEXLIZET and cholestyramine decreases ezetimibe concentration. This may result in a reduction of efficacy [see Clinical Pharmacology (12.3) ]. Intervention: Administer NEXLIZET either at least 2 hours before or at least 4 hours after bile acid sequestrants [see Dosage and Administration (2.2) ] .
Description
Indications and Usage ( 1 ) 11/2025
Medication Information
Warnings and Precautions
Hyperuricemia: Elevations in serum uric acid have occurred. Assess uric acid levels periodically as clinically indicated. Monitor for signs and symptoms of hyperuricemia, and initiate treatment with urate-lowering drugs as appropriate. ( 5.1 ) Tendon Rupture: Tendon rupture has occurred. Discontinue NEXLIZET at the first sign of tendon rupture. Avoid NEXLIZET in patients who have a history of tendon disorders or tendon rupture. ( 5.2 )
Indications and Usage
NEXLIZET, a combination of bempedoic acid and ezetimibe, is indicated: as an adjunct to diet and exercise to reduce LDL-C in adults with hypercholesterolemia, including heterozygous familial hypercholesterolemia (HeFH). Bempedoic acid, a component of NEXLIZET, is indicated: to reduce the risk of major adverse cardiovascular events (cardiovascular death, myocardial infarction, stroke, or coronary revascularization) in adults at increased risk for these events who are unable to take recommended statin therapy (including those not taking a statin).
Dosage and Administration
Administer one tablet (180 mg bempedoic acid and 10 mg ezetimibe) orally once daily with or without food. ( 2.1 ) Swallow the tablet whole. ( 2.1 ) Coadministration with Bile Acid Sequestrants: Administer at least 2 hours before or at least 4 hours after bile acid sequestrants. ( 2.2 )
Dosage Forms and Strengths
How Supplied
NEXLIZET tablets are supplied as follows:
| Tablet Strength | Description | Package Configuration | NDC No. |
|---|---|---|---|
| 180 mg of bempedoic acid and 10 mg of ezetimibe | blue, oval shaped, debossed with "818" on one side and "ESP" on the other side | Bottle of 30 tablets with child-resistant cap | 72426-818-03 |
Contraindications
NEXLIZET is contraindicated in patients with a prior hypersensitivity to ezetimibe or bempedoic acid or any of the excipients in NEXLIZET [see Adverse Reactions (6.2) ] . Serious hypersensitivity reactions, such as anaphylaxis, angioedema, rash and urticaria have been reported with ezetimibe or bempedoic acid.
Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling: Hyperuricemia [see Warnings and Precautions (5.1) ] Tendon Rupture [see Warnings and Precautions (5.2) ]
Drug Interactions
No specific pharmacokinetic drug interaction studies with NEXLIZET have been conducted. Table 4 lists drug interactions with NEXLIZET that have been identified in studies with bempedoic acid or ezetimibe. Table 4. Clinically Important Drug Interactions with NEXLIZET Simvastatin Clinical Impact: Concomitant use of NEXLIZET with simvastatin causes an increase in simvastatin concentration and may increase the risk of simvastatin-related myopathy [see Clinical Pharmacology (12.3) ] . Intervention: Avoid concomitant use of NEXLIZET with simvastatin greater than 20 mg. Pravastatin Clinical Impact: Concomitant use of NEXLIZET with pravastatin causes an increase in pravastatin concentration and may increase the risk of pravastatin-related myopathy [see Clinical Pharmacology (12.3) ] . Intervention: Avoid concomitant use of NEXLIZET with pravastatin greater than 40 mg. Cyclosporine Clinical Impact: Concomitant use of NEXLIZET and cyclosporine increases ezetimibe and cyclosporine concentrations. The degree of increase in ezetimibe exposure may be greater in patients with severe renal insufficiency [see Clinical Pharmacology (12.3) ] . Intervention: Monitor cyclosporine concentrations in patients receiving NEXLIZET and cyclosporine. In patients treated with cyclosporine, weigh the potential effects of the increased exposure to ezetimibe from concomitant use against the benefits of alterations in lipid levels provided by NEXLIZET. Fibrates Clinical Impact: Both fenofibrate and ezetimibe (a component of NEXLIZET) may increase cholesterol excretion into the bile, leading to cholelithiasis. Coadministration of NEXLIZET with fibrates other than fenofibrate is not recommended [see Adverse Reactions (6.1) ] . Intervention: If cholelithiasis is suspected in a patient receiving NEXLIZET and fenofibrate, gallbladder studies are indicated and alternative lipid-lowering therapy should be considered. Clinical Impact: Concomitant administration of fibrates with bempedoic acid (a component of NEXLIZET) resulted in increased triglycerides and decreased high-density lipoprotein cholesterol (HDL-C) in some patients in clinical studies and post-marketing reports. Reversibility of both increased triglycerides and decreased HDL-C levels was observed when either bempedoic acid or fibrate therapy was discontinued. Intervention: Monitor triglycerides and HDL-C four weeks after initial concomitant use of NEXLIZET and a fibrate and periodically thereafter. If increased triglycerides or decreased HDL-C levels are detected, discontinue NEXLIZET or fibrate therapy based on clinical judgment. Monitor triglycerides and HDL-C levels until levels return to baseline. Cholestyramine Clinical Impact: Concomitant use of NEXLIZET and cholestyramine decreases ezetimibe concentration. This may result in a reduction of efficacy [see Clinical Pharmacology (12.3) ]. Intervention: Administer NEXLIZET either at least 2 hours before or at least 4 hours after bile acid sequestrants [see Dosage and Administration (2.2) ] .
Description
Indications and Usage ( 1 ) 11/2025
Section 42229-5
Bempedoic acid
The data in Table 1 reflect exposure to bempedoic acid in two placebo-controlled primary hypercholesterolemia trials that included 2,009 patients treated with bempedoic acid for 52 weeks (median treatment duration of 52 weeks) [see Clinical Studies (14.1)]. The mean age for bempedoic acid-treated patients was 65 years, 29% were female, 95% were White, 3% were Black or African American, 1% were Asian, and 1% were other races; 3% identified as Hispanic or Latino ethnicity. All patients received bempedoic acid 180 mg orally once daily plus maximally tolerated statin therapy alone or in combination with other lipid-lowering therapies. At baseline, 97% of patients had CVD and about 4% had a diagnosis of HeFH. Patients on simvastatin 40 mg/day or higher were excluded from the trials.
In the primary hypercholesterolemia trials, adverse reactions led to discontinuation of treatment in 11% of bempedoic acid-treated patients and 8% of placebo-treated patients. The most common reasons for bempedoic acid treatment discontinuation were muscle spasms (0.5% versus 0.3% placebo), diarrhea (0.4% versus 0.1% placebo), and pain in extremity (0.3% versus 0.0% placebo). Adverse reactions reported in at least 2% of bempedoic acid-treated patients and more frequently than in placebo-treated patients are shown in Table 1.
| Adverse Reaction | Placebo Background therapy included statin ± other lipid-lowering therapies
(N = 999) % |
Bempedoic acid
(N = 2,009) % |
|---|---|---|
| Upper respiratory tract infection | 4.0 | 4.5 |
| Muscle spasms | 2.3 | 3.6 |
| Hyperuricemia Grouped term that includes other related terms
|
1.1 | 3.5 |
| Back pain | 2.2 | 3.3 |
| Abdominal pain or discomfort | 2.2 | 3.1 |
| Bronchitis | 2.5 | 3.0 |
| Pain in extremity | 1.7 | 3.0 |
| Anemia | 1.9 | 2.8 |
| Elevated liver enzymes | 0.8 | 2.1 |
In the cardiovascular outcomes trial in which 7,001 patients were exposed to bempedoic acid and 6,964 patients were exposed to placebo for a median of 3.1 years [see Clinical Studies (14.2)], adverse reactions led to discontinuation of treatment in 11% of bempedoic acid-treated patients and 10% of placebo-treated patients. Adverse reactions reported in at least 2% of bempedoic acid-treated patients and more frequently than placebo are shown in Table 2.
| Adverse Reaction | Placebo (N=6,964) % |
Bempedoic Acid (N=7,001) % |
|---|---|---|
| Hyperuricemia Grouped term that includes other related terms
|
8 | 16 |
| Renal impairment Renal impairment includes laboratory related terms including glomerular filtration rate decreased, blood creatinine increased and hematuria
|
9 | 11 |
| Anemia | 4 | 5 |
| Elevated liver enzymes | 3 | 4 |
| Muscle spasms | 3 | 4 |
| Gout | 2 | 3 |
| Cholelithiasis | 1 | 2 |
Section 42230-3
| PATIENT INFORMATION NEXLIZET® (NEX-lee-zet) (bempedoic acid and ezetimibe) tablets, for oral use |
|||
|---|---|---|---|
| This Patient Information has been approved by the U.S. Food and Drug Administration | Revised: 01/2026 | ||
|
What is NEXLIZET?
NEXLIZET is a prescription medicine that contains 2 cholesterol-lowering medicines, bempedoic acid and ezetimibe.
|
|||
| Do not take NEXLIZET if you are allergic to ezetimibe, bempedoic acid, or any of the ingredients in NEXLIZET. See the end of this leaflet for a complete list of ingredients in NEXLIZET. Stop taking NEXLIZET, call your healthcare provider or go to the nearest hospital emergency room right away if you have any signs or symptoms of an allergic reaction including: | |||
|
|
||
Before you start taking NEXLIZET, tell your healthcare provider about all your medical conditions, including if you:
Especially tell your healthcare provider if you take or plan to take:
|
|||
How should I take NEXLIZET?
|
|||
|
What are possible side effects of NEXLIZET? NEXLIZET may cause serious side effects, including:
|
|||
|
|
||
|
|||
|
|
||
|
|||
| The most common side effects of NEXLIZET in people with primary hypercholesterolemia include: | |||
|
|
||
| The most common side effects of bempedoic acid in people with heart problems include: | |||
|
|
||
| Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of NEXLIZET. Ask your healthcare provider or pharmacist for more information. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|||
How should I store NEXLIZET?
|
|||
|
General information about the safe and effective use of NEXLIZET.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use NEXLIZET for a condition for which it was not prescribed. Do not give NEXLIZET to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about NEXLIZET that is written for healthcare professionals. |
|||
What are the ingredients in NEXLIZET?
|
|||
| Manufactured for: Esperion Therapeutics, Inc. 3891 Ranchero Drive, Suite 150 Ann Arbor, MI 48108 © 2026 Esperion Therapeutics, Inc. |
Section 43683-2
| Indications and Usage (1) | 11/2025 |
Section 44425-7
Storage and Handling
Store at 68°F to 77°F (20°C to 25°C); excursions permitted to 59°F to 86°F (15°C to 30°C) [see USP Controlled Room Temperature]. Store and dispense in the original package protected from extreme heat and humidity. Do not discard desiccant.
10 Overdosage
There is no clinical experience with NEXLIZET overdosage. In the event of an overdosage, consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdosage management recommendations.
11 Description
NEXLIZET tablets, for oral use, contain bempedoic acid, an adenosine triphosphate-citrate lyase (ACL) inhibitor, and ezetimibe, a dietary cholesterol absorption inhibitor.
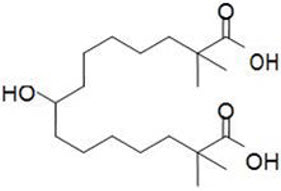
The chemical name for bempedoic acid is 8-hydroxy-2,2,14,14-tetramethyl-pentadecanedioic acid. The molecular formula is C19H36O5, and the molecular weight is 344.5 grams per mole. Bempedoic acid is a white to off-white crystalline powder that is highly soluble in ethanol, isopropanol and pH 8.0 phosphate buffer, and insoluble in water and aqueous solutions below pH 5.
Structural formula:
The chemical name for ezetimibe is 1-(4-fluorophenyl)-3(R)-[3-(4-fluorophenyl)-3(S)- hydroxypropyl]-4(S)-(4-hydroxyphenyl)-2-azetidinone. The molecular formula is C24H21F2NO3 and the molecular weight is 409.4 grams per mole. Ezetimibe is a white, crystalline powder that is freely to very soluble in ethanol, methanol, and acetone and practically insoluble in water.
Structural formula:
Each film-coated tablet of NEXLIZET contains 180 mg of bempedoic acid and 10 mg of ezetimibe, and the following inactive ingredients: colloidal silicon dioxide, hydroxy propyl cellulose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone K30, sodium lauryl sulfate, sodium starch glycolate. The film coating comprises of FD&C Blue #1/Brilliant Blue FCF Aluminum Lake, FD&C Blue #2/Indigo Carmine Aluminum Lake, glyceryl monocaprylocaprate, partially hydrolyzed polyvinyl alcohol, sodium lauryl sulfate, talc, and titanium dioxide.
Unmapped Section
Simvastatin: Administration of simvastatin 20 mg with 240 mg of bempedoic acid or 40 mg with 180 mg of bempedoic acid in healthy subjects at steady-state resulted in approximately 2-fold (91% for 20 mg and 96% for 40 mg) and 1.5-fold (54% for 20 mg and 52% for 40 mg) increases in simvastatin acid AUC and Cmax, respectively [see Drug Interactions (7)].
5.1 Hyperuricemia
Bempedoic acid, a component of NEXLIZET, inhibits renal tubular OAT2 and may increase blood uric acid levels [see Clinical Pharmacology (12.3)]. In the primary hypercholesterolemia trials [see Clinical Studies (14.1)], 26% of bempedoic acid-treated patients with normal baseline uric acid values (versus 9.5% placebo) experienced hyperuricemia one or more times, and 3.5% of patients experienced clinically significant hyperuricemia reported as an adverse reaction (versus 1.1% placebo). Increases in uric acid levels usually occurred within the first 4 weeks of treatment initiation, persisted throughout treatment, and returned to baseline following discontinuation of treatment. After 12 weeks of treatment, the mean placebo-adjusted increase in uric acid compared to baseline was 0.8 mg/dL for patients treated with bempedoic acid. In the cardiovascular outcomes trial [see Clinical Studies (14.2)], 16.4% of bempedoic acid-treated patients experienced clinically significant hyperuricemia reported as an adverse reaction (versus 8.2% placebo).
Elevated blood uric acid may lead to the development of gout. In the primary hypercholesterolemia trials, gout was reported in 1.5% of patients treated with bempedoic acid versus 0.4% of patients treated with placebo. In the cardiovascular outcomes trial, gout was reported in 3.2% of patients treated with bempedoic acid and 2.2% treated with placebo.
Advise patients to contact their healthcare provider if symptoms of hyperuricemia occur. Assess serum uric acid when clinically indicated. Monitor patients for signs and symptoms of hyperuricemia, and initiate treatment with urate-lowering drugs as appropriate.
8.4 Pediatric Use
The safety and effectiveness of NEXLIZET have not been established in pediatric patients.
8.5 Geriatric Use
Of the 301 patients in the clinical trial of NEXLIZET, 149 (50%) were 65 years of age and older, while 49 (16%) were 75 years of age and over. No overall differences in safety or effectiveness of NEXLIZET have been observed between patients 65 years of age and older and younger adult patients.
5.2 Tendon Rupture
Bempedoic acid, a component of NEXLIZET, is associated with an increased risk of tendon rupture or injury. In the primary hypercholesterolemia trials [see Clinical Studies (14.1)], tendon rupture occurred in 0.5% of patients treated with bempedoic acid versus 0% of placebo-treated patients and involved the rotator cuff (the shoulder), biceps tendon, or Achilles tendon. Tendon rupture occurred within weeks to months of starting bempedoic acid. In the cardiovascular outcomes trial [see Clinical Studies (14.2)], tendon rupture events occurred in 1.2% of bempedoic acid-treated patients versus 0.9% of placebo-treated patients. Tendon rupture may occur more frequently in patients over 60 years of age, in those taking corticosteroid or fluoroquinolone drugs, in patients with renal failure, and in patients with previous tendon disorders.
Discontinue NEXLIZET immediately if the patient experiences rupture of a tendon. Consider discontinuing NEXLIZET if the patient experiences joint pain, swelling, or inflammation. Advise patients to rest at the first sign of tendinitis or tendon rupture and to contact their healthcare provider if tendinitis or tendon rupture symptoms occur. Consider alternative therapy in patients with a history of tendon disorders or tendon rupture.
4 Contraindications
NEXLIZET is contraindicated in patients with a prior hypersensitivity to ezetimibe or bempedoic acid or any of the excipients in NEXLIZET [see Adverse Reactions (6.2)]. Serious hypersensitivity reactions, such as anaphylaxis, angioedema, rash and urticaria have been reported with ezetimibe or bempedoic acid.
6 Adverse Reactions
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hyperuricemia [see Warnings and Precautions (5.1)]
- Tendon Rupture [see Warnings and Precautions (5.2)]
7 Drug Interactions
No specific pharmacokinetic drug interaction studies with NEXLIZET have been conducted. Table 4 lists drug interactions with NEXLIZET that have been identified in studies with bempedoic acid or ezetimibe.
| Simvastatin | |
| Clinical Impact: | Concomitant use of NEXLIZET with simvastatin causes an increase in simvastatin concentration and may increase the risk of simvastatin-related myopathy [see Clinical Pharmacology (12.3)]. |
| Intervention: | Avoid concomitant use of NEXLIZET with simvastatin greater than 20 mg. |
| Pravastatin | |
| Clinical Impact: | Concomitant use of NEXLIZET with pravastatin causes an increase in pravastatin concentration and may increase the risk of pravastatin-related myopathy [see Clinical Pharmacology (12.3)]. |
| Intervention: | Avoid concomitant use of NEXLIZET with pravastatin greater than 40 mg. |
| Cyclosporine | |
| Clinical Impact: | Concomitant use of NEXLIZET and cyclosporine increases ezetimibe and cyclosporine concentrations. The degree of increase in ezetimibe exposure may be greater in patients with severe renal insufficiency [see Clinical Pharmacology (12.3)]. |
| Intervention: | Monitor cyclosporine concentrations in patients receiving NEXLIZET and cyclosporine. In patients treated with cyclosporine, weigh the potential effects of the increased exposure to ezetimibe from concomitant use against the benefits of alterations in lipid levels provided by NEXLIZET. |
| Fibrates | |
| Clinical Impact: | Both fenofibrate and ezetimibe (a component of NEXLIZET) may increase cholesterol excretion into the bile, leading to cholelithiasis. Coadministration of NEXLIZET with fibrates other than fenofibrate is not recommended [see Adverse Reactions (6.1)]. |
| Intervention: | If cholelithiasis is suspected in a patient receiving NEXLIZET and fenofibrate, gallbladder studies are indicated and alternative lipid-lowering therapy should be considered. |
| Clinical Impact: | Concomitant administration of fibrates with bempedoic acid (a component of NEXLIZET) resulted in increased triglycerides and decreased high-density lipoprotein cholesterol (HDL-C) in some patients in clinical studies and post-marketing reports. Reversibility of both increased triglycerides and decreased HDL-C levels was observed when either bempedoic acid or fibrate therapy was discontinued. |
| Intervention: | Monitor triglycerides and HDL-C four weeks after initial concomitant use of NEXLIZET and a fibrate and periodically thereafter. If increased triglycerides or decreased HDL-C levels are detected, discontinue NEXLIZET or fibrate therapy based on clinical judgment. Monitor triglycerides and HDL-C levels until levels return to baseline. |
| Cholestyramine | |
| Clinical Impact: | Concomitant use of NEXLIZET and cholestyramine decreases ezetimibe concentration. This may result in a reduction of efficacy [see Clinical Pharmacology (12.3)]. |
| Intervention: | Administer NEXLIZET either at least 2 hours before or at least 4 hours after bile acid sequestrants [see Dosage and Administration (2.2)]. |
12.2 Pharmacodynamics
Administration of bempedoic acid and ezetimibe in combination with other lipid modifying agents, decreases LDL-C, non-high density lipoprotein cholesterol (non-HDL-C), apolipoprotein B (apo B), and total cholesterol (TC) in patients with hypercholesterolemia.
8.7 Hepatic Impairment
No dosage adjustment is necessary in patients with mild hepatic impairment (Child-Pugh A) [see Clinical Pharmacology (12.3)]. NEXLIZET is not recommended in patients with moderate or severe hepatic impairment (Child-Pugh B or C) due to the unknown effects of the increased exposure to ezetimibe [see Clinical Pharmacology (12.3)].
1 Indications and Usage
NEXLIZET, a combination of bempedoic acid and ezetimibe, is indicated:
- as an adjunct to diet and exercise to reduce LDL-C in adults with hypercholesterolemia, including heterozygous familial hypercholesterolemia (HeFH).
Bempedoic acid, a component of NEXLIZET, is indicated:
- to reduce the risk of major adverse cardiovascular events (cardiovascular death, myocardial infarction, stroke, or coronary revascularization) in adults at increased risk for these events who are unable to take recommended statin therapy (including those not taking a statin).
12.1 Mechanism of Action
NEXLIZET contains bempedoic acid and ezetimibe. NEXLIZET reduces elevated LDL-C through inhibition of cholesterol synthesis in the liver and absorption in the intestine.
5 Warnings and Precautions
Hyperuricemia: Elevations in serum uric acid have occurred. Assess uric acid levels periodically as clinically indicated. Monitor for signs and symptoms of hyperuricemia, and initiate treatment with urate-lowering drugs as appropriate. (5.1)
Tendon Rupture: Tendon rupture has occurred. Discontinue NEXLIZET at the first sign of tendon rupture. Avoid NEXLIZET in patients who have a history of tendon disorders or tendon rupture. (5.2)
2 Dosage and Administration
3 Dosage Forms and Strengths
NEXLIZET is available as:
- Tablets: 180 mg/10 mg, blue, oval shaped, debossed with "818" on one side and "ESP" on the other side.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of ezetimibe and/or bempedoic acid. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood Disorders: thrombocytopenia
Gastrointestinal Disorders: abdominal pain; pancreatitis; nausea
Hepatobiliary Disorders: elevations in liver transaminases, including elevations more than 5× ULN; hepatitis; cholelithiasis; cholecystitis
Immune System Disorders: Hypersensitivity reactions including: anaphylaxis, angioedema, wheezing, rash, and urticaria
Musculoskeletal Disorders: elevated creatine phosphokinase; myopathy/rhabdomyolysis
Nervous System Disorders: dizziness; paresthesia; depression; headache
Skin and Subcutaneous Tissue Disorders: erythema multiforme
8 Use in Specific Populations
- Pregnancy: Based on mechanism of action, may cause fetal harm. (8.1)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
17 Patient Counseling Information
Advise patients to read the FDA-approved patient labeling (Patient Information).
2.1 Recommended Dosage and Administration
- The recommended dosage of NEXLIZET is one tablet orally once daily. One tablet of NEXLIZET contains 180 mg of bempedoic acid and 10 mg of ezetimibe.
- Swallow the tablet whole. NEXLIZET can be taken with or without food.
- If a dose is missed, take the missed dose as soon as possible. Do not double the next dose.
- After initiation of NEXLIZET, analyze lipid levels within 8 to 12 weeks.
2.2 Coadministration With Bile Acid Sequestrants
Administer NEXLIZET either at least 2 hours before or at least 4 hours after administration of a bile acid sequestrant [see Drug Interactions (7)].
14.1 Primary Hypercholesterolemia Trials in Adults
The efficacy of NEXLIZET was investigated in a single, multi-center, randomized, double-blind, placebo-controlled, parallel group trial that enrolled 301 patients with HeFH, established CVD, or multiple risk factors for CVD on maximally tolerated statin therapy.
Trial 1 (NCT03337308) was a 4-arm, 12-week trial that assessed the efficacy of NEXLIZET in 301 patients randomized 2:2:2:1 to receive either oral NEXLIZET (180 mg of bempedoic acid and 10 mg of ezetimibe) (n = 86), bempedoic acid 180 mg (n = 88), ezetimibe 10 mg (n = 86), or placebo (n = 41) once daily as add-on to maximally tolerated statin therapy. Patients were stratified by cardiovascular risk and baseline statin intensity. Patients on simvastatin 40 mg per day or higher and patients taking non-statin lipid-lowering therapy (including fibrates, niacin, bile acid sequestrants, ezetimibe, and PCSK9 inhibitors) were excluded from the trial.
Principal Display Panel 180 Mg/10 Mg Tablet Bottle Label
NDC 72426-818-03
Rx only
NEXLIZET®
(bempedoic acid
and ezetimibe) tablets
Contains
30 Tablets
180 mg/10 mg
14.2 Cardiovascular Outcomes Trial in Adults With Cvd Or At High Risk for Cvd
Trial 4 (NCT02993406) was a randomized, double-blind, placebo-controlled, event-driven trial in 13,970 adult patients with established CVD (70%) or at high risk for a CVD event but without CVD (30%) who were not receiving recommended statin dosages. Patients with established CVD had documented history of coronary artery disease, symptomatic peripheral arterial disease, and/or cerebrovascular atherosclerotic disease. Patients without established CVD were considered at high risk for CVD based on meeting at least one of the following criteria:
-
(1) Diabetes mellitus (type 1 or type 2) in females over 65 years of age or males over 60 years of age;
(2) A Reynolds Risk score > 30% or a SCORE Risk score > 7.5% over 10 years. Reynolds risk score and SCORE risk score evaluate a 10-year risk of having a cardiovascular (CV) event. The Reynolds risk score is based on the following risk factors: sex, age, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, high sensitivity C-reactive protein (hsCRP), and familial history of CVD events. LDL-C is an additional risk factor considered in SCORE risk score; or
(3) A coronary artery calcium score >400 Agatston units at any time in the past.
Patients were randomized 1:1 to receive either oral bempedoic acid 180 mg per day (n = 6,992) or placebo (n = 6,978), alone or as an add on to other background lipid-lowering therapies. Background therapy could include less than low-intensity statin dosages. Overall, 95.3% of adult patients were followed until the end of the trial or death. The median follow-up duration was 3.4 years.
Structured Label Content
Dosage Forms and Strengths (34069-5)
How Supplied
NEXLIZET tablets are supplied as follows:
| Tablet Strength | Description | Package Configuration | NDC No. |
|---|---|---|---|
| 180 mg of bempedoic acid and 10 mg of ezetimibe | blue, oval shaped, debossed with "818" on one side and "ESP" on the other side | Bottle of 30 tablets with child-resistant cap | 72426-818-03 |
Section 42229-5 (42229-5)
Bempedoic acid
The data in Table 1 reflect exposure to bempedoic acid in two placebo-controlled primary hypercholesterolemia trials that included 2,009 patients treated with bempedoic acid for 52 weeks (median treatment duration of 52 weeks) [see Clinical Studies (14.1)]. The mean age for bempedoic acid-treated patients was 65 years, 29% were female, 95% were White, 3% were Black or African American, 1% were Asian, and 1% were other races; 3% identified as Hispanic or Latino ethnicity. All patients received bempedoic acid 180 mg orally once daily plus maximally tolerated statin therapy alone or in combination with other lipid-lowering therapies. At baseline, 97% of patients had CVD and about 4% had a diagnosis of HeFH. Patients on simvastatin 40 mg/day or higher were excluded from the trials.
In the primary hypercholesterolemia trials, adverse reactions led to discontinuation of treatment in 11% of bempedoic acid-treated patients and 8% of placebo-treated patients. The most common reasons for bempedoic acid treatment discontinuation were muscle spasms (0.5% versus 0.3% placebo), diarrhea (0.4% versus 0.1% placebo), and pain in extremity (0.3% versus 0.0% placebo). Adverse reactions reported in at least 2% of bempedoic acid-treated patients and more frequently than in placebo-treated patients are shown in Table 1.
| Adverse Reaction | Placebo Background therapy included statin ± other lipid-lowering therapies
(N = 999) % |
Bempedoic acid
(N = 2,009) % |
|---|---|---|
| Upper respiratory tract infection | 4.0 | 4.5 |
| Muscle spasms | 2.3 | 3.6 |
| Hyperuricemia Grouped term that includes other related terms
|
1.1 | 3.5 |
| Back pain | 2.2 | 3.3 |
| Abdominal pain or discomfort | 2.2 | 3.1 |
| Bronchitis | 2.5 | 3.0 |
| Pain in extremity | 1.7 | 3.0 |
| Anemia | 1.9 | 2.8 |
| Elevated liver enzymes | 0.8 | 2.1 |
In the cardiovascular outcomes trial in which 7,001 patients were exposed to bempedoic acid and 6,964 patients were exposed to placebo for a median of 3.1 years [see Clinical Studies (14.2)], adverse reactions led to discontinuation of treatment in 11% of bempedoic acid-treated patients and 10% of placebo-treated patients. Adverse reactions reported in at least 2% of bempedoic acid-treated patients and more frequently than placebo are shown in Table 2.
| Adverse Reaction | Placebo (N=6,964) % |
Bempedoic Acid (N=7,001) % |
|---|---|---|
| Hyperuricemia Grouped term that includes other related terms
|
8 | 16 |
| Renal impairment Renal impairment includes laboratory related terms including glomerular filtration rate decreased, blood creatinine increased and hematuria
|
9 | 11 |
| Anemia | 4 | 5 |
| Elevated liver enzymes | 3 | 4 |
| Muscle spasms | 3 | 4 |
| Gout | 2 | 3 |
| Cholelithiasis | 1 | 2 |
Section 42230-3 (42230-3)
| PATIENT INFORMATION NEXLIZET® (NEX-lee-zet) (bempedoic acid and ezetimibe) tablets, for oral use |
|||
|---|---|---|---|
| This Patient Information has been approved by the U.S. Food and Drug Administration | Revised: 01/2026 | ||
|
What is NEXLIZET?
NEXLIZET is a prescription medicine that contains 2 cholesterol-lowering medicines, bempedoic acid and ezetimibe.
|
|||
| Do not take NEXLIZET if you are allergic to ezetimibe, bempedoic acid, or any of the ingredients in NEXLIZET. See the end of this leaflet for a complete list of ingredients in NEXLIZET. Stop taking NEXLIZET, call your healthcare provider or go to the nearest hospital emergency room right away if you have any signs or symptoms of an allergic reaction including: | |||
|
|
||
Before you start taking NEXLIZET, tell your healthcare provider about all your medical conditions, including if you:
Especially tell your healthcare provider if you take or plan to take:
|
|||
How should I take NEXLIZET?
|
|||
|
What are possible side effects of NEXLIZET? NEXLIZET may cause serious side effects, including:
|
|||
|
|
||
|
|||
|
|
||
|
|||
| The most common side effects of NEXLIZET in people with primary hypercholesterolemia include: | |||
|
|
||
| The most common side effects of bempedoic acid in people with heart problems include: | |||
|
|
||
| Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of NEXLIZET. Ask your healthcare provider or pharmacist for more information. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|||
How should I store NEXLIZET?
|
|||
|
General information about the safe and effective use of NEXLIZET.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use NEXLIZET for a condition for which it was not prescribed. Do not give NEXLIZET to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about NEXLIZET that is written for healthcare professionals. |
|||
What are the ingredients in NEXLIZET?
|
|||
| Manufactured for: Esperion Therapeutics, Inc. 3891 Ranchero Drive, Suite 150 Ann Arbor, MI 48108 © 2026 Esperion Therapeutics, Inc. |
Section 43683-2 (43683-2)
| Indications and Usage (1) | 11/2025 |
Section 44425-7 (44425-7)
Storage and Handling
Store at 68°F to 77°F (20°C to 25°C); excursions permitted to 59°F to 86°F (15°C to 30°C) [see USP Controlled Room Temperature]. Store and dispense in the original package protected from extreme heat and humidity. Do not discard desiccant.
10 Overdosage (10 OVERDOSAGE)
There is no clinical experience with NEXLIZET overdosage. In the event of an overdosage, consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdosage management recommendations.
11 Description (11 DESCRIPTION)
NEXLIZET tablets, for oral use, contain bempedoic acid, an adenosine triphosphate-citrate lyase (ACL) inhibitor, and ezetimibe, a dietary cholesterol absorption inhibitor.
The chemical name for bempedoic acid is 8-hydroxy-2,2,14,14-tetramethyl-pentadecanedioic acid. The molecular formula is C19H36O5, and the molecular weight is 344.5 grams per mole. Bempedoic acid is a white to off-white crystalline powder that is highly soluble in ethanol, isopropanol and pH 8.0 phosphate buffer, and insoluble in water and aqueous solutions below pH 5.
Structural formula:
The chemical name for ezetimibe is 1-(4-fluorophenyl)-3(R)-[3-(4-fluorophenyl)-3(S)- hydroxypropyl]-4(S)-(4-hydroxyphenyl)-2-azetidinone. The molecular formula is C24H21F2NO3 and the molecular weight is 409.4 grams per mole. Ezetimibe is a white, crystalline powder that is freely to very soluble in ethanol, methanol, and acetone and practically insoluble in water.
Structural formula:
Each film-coated tablet of NEXLIZET contains 180 mg of bempedoic acid and 10 mg of ezetimibe, and the following inactive ingredients: colloidal silicon dioxide, hydroxy propyl cellulose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, povidone K30, sodium lauryl sulfate, sodium starch glycolate. The film coating comprises of FD&C Blue #1/Brilliant Blue FCF Aluminum Lake, FD&C Blue #2/Indigo Carmine Aluminum Lake, glyceryl monocaprylocaprate, partially hydrolyzed polyvinyl alcohol, sodium lauryl sulfate, talc, and titanium dioxide.
Unmapped Section (UNMAPPED_SECTION)
Simvastatin: Administration of simvastatin 20 mg with 240 mg of bempedoic acid or 40 mg with 180 mg of bempedoic acid in healthy subjects at steady-state resulted in approximately 2-fold (91% for 20 mg and 96% for 40 mg) and 1.5-fold (54% for 20 mg and 52% for 40 mg) increases in simvastatin acid AUC and Cmax, respectively [see Drug Interactions (7)].
5.1 Hyperuricemia
Bempedoic acid, a component of NEXLIZET, inhibits renal tubular OAT2 and may increase blood uric acid levels [see Clinical Pharmacology (12.3)]. In the primary hypercholesterolemia trials [see Clinical Studies (14.1)], 26% of bempedoic acid-treated patients with normal baseline uric acid values (versus 9.5% placebo) experienced hyperuricemia one or more times, and 3.5% of patients experienced clinically significant hyperuricemia reported as an adverse reaction (versus 1.1% placebo). Increases in uric acid levels usually occurred within the first 4 weeks of treatment initiation, persisted throughout treatment, and returned to baseline following discontinuation of treatment. After 12 weeks of treatment, the mean placebo-adjusted increase in uric acid compared to baseline was 0.8 mg/dL for patients treated with bempedoic acid. In the cardiovascular outcomes trial [see Clinical Studies (14.2)], 16.4% of bempedoic acid-treated patients experienced clinically significant hyperuricemia reported as an adverse reaction (versus 8.2% placebo).
Elevated blood uric acid may lead to the development of gout. In the primary hypercholesterolemia trials, gout was reported in 1.5% of patients treated with bempedoic acid versus 0.4% of patients treated with placebo. In the cardiovascular outcomes trial, gout was reported in 3.2% of patients treated with bempedoic acid and 2.2% treated with placebo.
Advise patients to contact their healthcare provider if symptoms of hyperuricemia occur. Assess serum uric acid when clinically indicated. Monitor patients for signs and symptoms of hyperuricemia, and initiate treatment with urate-lowering drugs as appropriate.
8.4 Pediatric Use
The safety and effectiveness of NEXLIZET have not been established in pediatric patients.
8.5 Geriatric Use
Of the 301 patients in the clinical trial of NEXLIZET, 149 (50%) were 65 years of age and older, while 49 (16%) were 75 years of age and over. No overall differences in safety or effectiveness of NEXLIZET have been observed between patients 65 years of age and older and younger adult patients.
5.2 Tendon Rupture
Bempedoic acid, a component of NEXLIZET, is associated with an increased risk of tendon rupture or injury. In the primary hypercholesterolemia trials [see Clinical Studies (14.1)], tendon rupture occurred in 0.5% of patients treated with bempedoic acid versus 0% of placebo-treated patients and involved the rotator cuff (the shoulder), biceps tendon, or Achilles tendon. Tendon rupture occurred within weeks to months of starting bempedoic acid. In the cardiovascular outcomes trial [see Clinical Studies (14.2)], tendon rupture events occurred in 1.2% of bempedoic acid-treated patients versus 0.9% of placebo-treated patients. Tendon rupture may occur more frequently in patients over 60 years of age, in those taking corticosteroid or fluoroquinolone drugs, in patients with renal failure, and in patients with previous tendon disorders.
Discontinue NEXLIZET immediately if the patient experiences rupture of a tendon. Consider discontinuing NEXLIZET if the patient experiences joint pain, swelling, or inflammation. Advise patients to rest at the first sign of tendinitis or tendon rupture and to contact their healthcare provider if tendinitis or tendon rupture symptoms occur. Consider alternative therapy in patients with a history of tendon disorders or tendon rupture.
4 Contraindications (4 CONTRAINDICATIONS)
NEXLIZET is contraindicated in patients with a prior hypersensitivity to ezetimibe or bempedoic acid or any of the excipients in NEXLIZET [see Adverse Reactions (6.2)]. Serious hypersensitivity reactions, such as anaphylaxis, angioedema, rash and urticaria have been reported with ezetimibe or bempedoic acid.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hyperuricemia [see Warnings and Precautions (5.1)]
- Tendon Rupture [see Warnings and Precautions (5.2)]
7 Drug Interactions (7 DRUG INTERACTIONS)
No specific pharmacokinetic drug interaction studies with NEXLIZET have been conducted. Table 4 lists drug interactions with NEXLIZET that have been identified in studies with bempedoic acid or ezetimibe.
| Simvastatin | |
| Clinical Impact: | Concomitant use of NEXLIZET with simvastatin causes an increase in simvastatin concentration and may increase the risk of simvastatin-related myopathy [see Clinical Pharmacology (12.3)]. |
| Intervention: | Avoid concomitant use of NEXLIZET with simvastatin greater than 20 mg. |
| Pravastatin | |
| Clinical Impact: | Concomitant use of NEXLIZET with pravastatin causes an increase in pravastatin concentration and may increase the risk of pravastatin-related myopathy [see Clinical Pharmacology (12.3)]. |
| Intervention: | Avoid concomitant use of NEXLIZET with pravastatin greater than 40 mg. |
| Cyclosporine | |
| Clinical Impact: | Concomitant use of NEXLIZET and cyclosporine increases ezetimibe and cyclosporine concentrations. The degree of increase in ezetimibe exposure may be greater in patients with severe renal insufficiency [see Clinical Pharmacology (12.3)]. |
| Intervention: | Monitor cyclosporine concentrations in patients receiving NEXLIZET and cyclosporine. In patients treated with cyclosporine, weigh the potential effects of the increased exposure to ezetimibe from concomitant use against the benefits of alterations in lipid levels provided by NEXLIZET. |
| Fibrates | |
| Clinical Impact: | Both fenofibrate and ezetimibe (a component of NEXLIZET) may increase cholesterol excretion into the bile, leading to cholelithiasis. Coadministration of NEXLIZET with fibrates other than fenofibrate is not recommended [see Adverse Reactions (6.1)]. |
| Intervention: | If cholelithiasis is suspected in a patient receiving NEXLIZET and fenofibrate, gallbladder studies are indicated and alternative lipid-lowering therapy should be considered. |
| Clinical Impact: | Concomitant administration of fibrates with bempedoic acid (a component of NEXLIZET) resulted in increased triglycerides and decreased high-density lipoprotein cholesterol (HDL-C) in some patients in clinical studies and post-marketing reports. Reversibility of both increased triglycerides and decreased HDL-C levels was observed when either bempedoic acid or fibrate therapy was discontinued. |
| Intervention: | Monitor triglycerides and HDL-C four weeks after initial concomitant use of NEXLIZET and a fibrate and periodically thereafter. If increased triglycerides or decreased HDL-C levels are detected, discontinue NEXLIZET or fibrate therapy based on clinical judgment. Monitor triglycerides and HDL-C levels until levels return to baseline. |
| Cholestyramine | |
| Clinical Impact: | Concomitant use of NEXLIZET and cholestyramine decreases ezetimibe concentration. This may result in a reduction of efficacy [see Clinical Pharmacology (12.3)]. |
| Intervention: | Administer NEXLIZET either at least 2 hours before or at least 4 hours after bile acid sequestrants [see Dosage and Administration (2.2)]. |
12.2 Pharmacodynamics
Administration of bempedoic acid and ezetimibe in combination with other lipid modifying agents, decreases LDL-C, non-high density lipoprotein cholesterol (non-HDL-C), apolipoprotein B (apo B), and total cholesterol (TC) in patients with hypercholesterolemia.
8.7 Hepatic Impairment
No dosage adjustment is necessary in patients with mild hepatic impairment (Child-Pugh A) [see Clinical Pharmacology (12.3)]. NEXLIZET is not recommended in patients with moderate or severe hepatic impairment (Child-Pugh B or C) due to the unknown effects of the increased exposure to ezetimibe [see Clinical Pharmacology (12.3)].
1 Indications and Usage (1 INDICATIONS AND USAGE)
NEXLIZET, a combination of bempedoic acid and ezetimibe, is indicated:
- as an adjunct to diet and exercise to reduce LDL-C in adults with hypercholesterolemia, including heterozygous familial hypercholesterolemia (HeFH).
Bempedoic acid, a component of NEXLIZET, is indicated:
- to reduce the risk of major adverse cardiovascular events (cardiovascular death, myocardial infarction, stroke, or coronary revascularization) in adults at increased risk for these events who are unable to take recommended statin therapy (including those not taking a statin).
12.1 Mechanism of Action
NEXLIZET contains bempedoic acid and ezetimibe. NEXLIZET reduces elevated LDL-C through inhibition of cholesterol synthesis in the liver and absorption in the intestine.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
Hyperuricemia: Elevations in serum uric acid have occurred. Assess uric acid levels periodically as clinically indicated. Monitor for signs and symptoms of hyperuricemia, and initiate treatment with urate-lowering drugs as appropriate. (5.1)
Tendon Rupture: Tendon rupture has occurred. Discontinue NEXLIZET at the first sign of tendon rupture. Avoid NEXLIZET in patients who have a history of tendon disorders or tendon rupture. (5.2)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
NEXLIZET is available as:
- Tablets: 180 mg/10 mg, blue, oval shaped, debossed with "818" on one side and "ESP" on the other side.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of ezetimibe and/or bempedoic acid. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood Disorders: thrombocytopenia
Gastrointestinal Disorders: abdominal pain; pancreatitis; nausea
Hepatobiliary Disorders: elevations in liver transaminases, including elevations more than 5× ULN; hepatitis; cholelithiasis; cholecystitis
Immune System Disorders: Hypersensitivity reactions including: anaphylaxis, angioedema, wheezing, rash, and urticaria
Musculoskeletal Disorders: elevated creatine phosphokinase; myopathy/rhabdomyolysis
Nervous System Disorders: dizziness; paresthesia; depression; headache
Skin and Subcutaneous Tissue Disorders: erythema multiforme
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
- Pregnancy: Based on mechanism of action, may cause fetal harm. (8.1)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise patients to read the FDA-approved patient labeling (Patient Information).
2.1 Recommended Dosage and Administration
- The recommended dosage of NEXLIZET is one tablet orally once daily. One tablet of NEXLIZET contains 180 mg of bempedoic acid and 10 mg of ezetimibe.
- Swallow the tablet whole. NEXLIZET can be taken with or without food.
- If a dose is missed, take the missed dose as soon as possible. Do not double the next dose.
- After initiation of NEXLIZET, analyze lipid levels within 8 to 12 weeks.
2.2 Coadministration With Bile Acid Sequestrants (2.2 Coadministration with Bile Acid Sequestrants)
Administer NEXLIZET either at least 2 hours before or at least 4 hours after administration of a bile acid sequestrant [see Drug Interactions (7)].
14.1 Primary Hypercholesterolemia Trials in Adults
The efficacy of NEXLIZET was investigated in a single, multi-center, randomized, double-blind, placebo-controlled, parallel group trial that enrolled 301 patients with HeFH, established CVD, or multiple risk factors for CVD on maximally tolerated statin therapy.
Trial 1 (NCT03337308) was a 4-arm, 12-week trial that assessed the efficacy of NEXLIZET in 301 patients randomized 2:2:2:1 to receive either oral NEXLIZET (180 mg of bempedoic acid and 10 mg of ezetimibe) (n = 86), bempedoic acid 180 mg (n = 88), ezetimibe 10 mg (n = 86), or placebo (n = 41) once daily as add-on to maximally tolerated statin therapy. Patients were stratified by cardiovascular risk and baseline statin intensity. Patients on simvastatin 40 mg per day or higher and patients taking non-statin lipid-lowering therapy (including fibrates, niacin, bile acid sequestrants, ezetimibe, and PCSK9 inhibitors) were excluded from the trial.
Principal Display Panel 180 Mg/10 Mg Tablet Bottle Label (PRINCIPAL DISPLAY PANEL - 180 mg/10 mg Tablet Bottle Label)
NDC 72426-818-03
Rx only
NEXLIZET®
(bempedoic acid
and ezetimibe) tablets
Contains
30 Tablets
180 mg/10 mg
14.2 Cardiovascular Outcomes Trial in Adults With Cvd Or At High Risk for Cvd (14.2 Cardiovascular Outcomes Trial in Adults With CVD or at High Risk for CVD)
Trial 4 (NCT02993406) was a randomized, double-blind, placebo-controlled, event-driven trial in 13,970 adult patients with established CVD (70%) or at high risk for a CVD event but without CVD (30%) who were not receiving recommended statin dosages. Patients with established CVD had documented history of coronary artery disease, symptomatic peripheral arterial disease, and/or cerebrovascular atherosclerotic disease. Patients without established CVD were considered at high risk for CVD based on meeting at least one of the following criteria:
-
(1) Diabetes mellitus (type 1 or type 2) in females over 65 years of age or males over 60 years of age;
(2) A Reynolds Risk score > 30% or a SCORE Risk score > 7.5% over 10 years. Reynolds risk score and SCORE risk score evaluate a 10-year risk of having a cardiovascular (CV) event. The Reynolds risk score is based on the following risk factors: sex, age, smoking status, systolic blood pressure, total cholesterol, HDL cholesterol, high sensitivity C-reactive protein (hsCRP), and familial history of CVD events. LDL-C is an additional risk factor considered in SCORE risk score; or
(3) A coronary artery calcium score >400 Agatston units at any time in the past.
Patients were randomized 1:1 to receive either oral bempedoic acid 180 mg per day (n = 6,992) or placebo (n = 6,978), alone or as an add on to other background lipid-lowering therapies. Background therapy could include less than low-intensity statin dosages. Overall, 95.3% of adult patients were followed until the end of the trial or death. The median follow-up duration was 3.4 years.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:52:25.942948 · Updated: 2026-03-14T22:43:43.392452