vasotec®
39631f1f-5d19-43c1-b504-bf56d991ed97
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Contraindications
VASOTEC is contraindicated in patients who are hypersensitive to this product and in patients with a history of angioedema related to previous treatment with an angiotensin-converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema. Do not coadminister aliskiren with VASOTEC in patients with diabetes (see PRECAUTIONS , Drug Interactions ). VASOTEC is contraindicated in combination with a neprilysin inhibitor (e.g., sacubitril). Do not administer VASOTEC within 36 hours of switching to or from sacubitril/valsartan, a neprilysin inhibitor (see WARNINGS , Head and Neck Angioedema ).
Adverse Reactions
VASOTEC has been evaluated for safety in more than 10,000 patients, including over 1000 patients treated for one year or more. VASOTEC has been found to be generally well tolerated in controlled clinical trials involving 2987 patients. For the most part, adverse experiences were mild and transient in nature. In clinical trials, discontinuation of therapy due to clinical adverse experiences was required in 3.3 percent of patients with hypertension and in 5.7 percent of patients with heart failure. The frequency of adverse experiences was not related to total daily dosage within the usual dosage ranges. In patients with hypertension the overall percentage of patients treated with VASOTEC reporting adverse experiences was comparable to placebo.
How Supplied
VASOTEC (enalapril maleate) Tablets NDC Strength Quantity Description 0187-0140-30 0187-0140-90 2.5 mg Bottles of 30 (with desiccant) Bottles of 90 (with desiccant) White, oval shaped tablet imprinted with “VASO 2.5” and scored on one side and scored on the other. 0187-0141-30 0187-0141-90 5 mg Bottles of 30 (with desiccant) Bottles of 90 (with desiccant) White, rounded triangle shaped tablet imprinted with “VASO 5” on one side and scored on the other. 0187-0142-30 0187-0142-90 0187-0142-10 10 mg Bottles of 30 (with desiccant) Bottles of 90 (with desiccant) Bottles of 1,000 (with desiccant) Rust red, rounded triangle shaped tablet imprinted with “VASO 10” on one side and scored on the other. 0187-0143-30 0187-0143-90 0187-0143-10 20 mg Bottles of 30 (with desiccant) Bottles of 90 (with desiccant) Bottles of 1,000 (with desiccant) Peach, rounded triangle shaped tablet imprinted with “VASO 20” on one side and scored on the other.
Description
See full prescribing information for complete boxed warning. • When pregnancy is detected, discontinue VASOTEC ® as soon as possible. • Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus (see WARNINGS, Fetal Toxicity ).
Medication Information
Contraindications
VASOTEC is contraindicated in patients who are hypersensitive to this product and in patients with a history of angioedema related to previous treatment with an angiotensin-converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema.
Do not coadminister aliskiren with VASOTEC in patients with diabetes (see PRECAUTIONS, Drug Interactions ).
VASOTEC is contraindicated in combination with a neprilysin inhibitor (e.g., sacubitril). Do not administer VASOTEC within 36 hours of switching to or from sacubitril/valsartan, a neprilysin inhibitor (see WARNINGS, Head and Neck Angioedema ).
Adverse Reactions
VASOTEC has been evaluated for safety in more than 10,000 patients, including over 1000 patients treated for one year or more. VASOTEC has been found to be generally well tolerated in controlled clinical trials involving 2987 patients. For the most part, adverse experiences were mild and transient in nature. In clinical trials, discontinuation of therapy due to clinical adverse experiences was required in 3.3 percent of patients with hypertension and in 5.7 percent of patients with heart failure. The frequency of adverse experiences was not related to total daily dosage within the usual dosage ranges. In patients with hypertension the overall percentage of patients treated with VASOTEC reporting adverse experiences was comparable to placebo.
How Supplied
|
VASOTEC (enalapril maleate) Tablets |
|||
|
NDC |
Strength |
Quantity |
Description |
|
0187-0140-30 0187-0140-90 |
2.5 mg |
Bottles of 30 Bottles of 90 |
White, oval shaped tablet imprinted with “VASO 2.5” and scored on one side and scored on the other. |
|
0187-0141-30 0187-0141-90 |
5 mg |
Bottles of 30 Bottles of 90 |
White, rounded triangle shaped tablet imprinted with “VASO 5” on one side and scored on the other. |
|
0187-0142-30 0187-0142-90 0187-0142-10 |
10 mg |
Bottles of 30 Bottles of 90 Bottles of 1,000 |
Rust red, rounded triangle shaped tablet imprinted with “VASO 10” on one side and scored on the other. |
|
0187-0143-30 0187-0143-90 0187-0143-10 |
20 mg |
Bottles of 30 Bottles of 90 Bottles of 1,000 |
Peach, rounded triangle shaped tablet imprinted with “VASO 20” on one side and scored on the other. |
Description
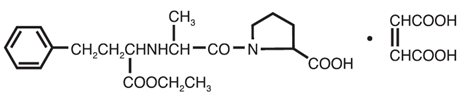
VASOTEC® (enalapril maleate) is the maleate salt of enalapril, the ethyl ester of a long-acting angiotensin-converting enzyme inhibitor, enalaprilat. Enalapril maleate is chemically described as (S)-1-[N-[1-(ethoxycarbonyl)-3-phenylpropyl]-L-alanyl]-L-proline, (Z)-2-butenedioate salt (1:1). Its empirical formula is C20H28N2O5•C4H4O4, and its structural formula is:
Enalapril maleate is a white to off-white, crystalline powder with a molecular weight of 492.53. It is sparingly soluble in water, soluble in ethanol, and freely soluble in methanol.
Enalapril is a pro-drug; following oral administration, it is bioactivated by hydrolysis of the ethyl ester to enalaprilat, which is the active angiotensin-converting enzyme inhibitor.
Enalapril maleate is supplied as 2.5 mg, 5 mg, 10 mg, and 20 mg tablets for oral administration. In addition to the active ingredient enalapril maleate, each tablet contains the following inactive ingredients: lactose, magnesium stearate, sodium bicarbonate, and starch. The 10 mg and 20 mg tablets also contain iron oxides.
Section 34072-9
General
Section 34073-7
Drug Interactions
Neprilysin Inhibitors
Patients taking concomitant neprilysin inhibitors may be at increased risk for angioedema (see WARNINGS ).
Section 34076-0
Information for Patients
Section 34080-2
Nursing Mothers
Enalapril and enalaprilat have been detected in human breast milk. Because of the potential for serious adverse reactions in nursing infants from enalapril, a decision should be made whether to discontinue nursing or to discontinue VASOTEC, taking into account the importance of the drug to the mother.
Section 34081-0
Pediatric Use
Section 34083-6
Carcinogenesis, Mutagenesis, Impairment of Fertility
There was no evidence of a tumorigenic effect when enalapril was administered for 106 weeks to male and female rats at doses up to 90 mg/kg/day or for 94 weeks to male and female mice at doses up to 90 and 180 mg/kg/day, respectively. These doses are 26 times (in rats and female mice) and 13 times (in male mice) the maximum recommended human daily dose (MRHDD) when compared on a body surface area basis.
Neither enalapril maleate nor the active diacid was mutagenic in the Ames microbial mutagen test with or without metabolic activation. Enalapril was also negative in the following genotoxicity studies: rec-assay, reverse mutation assay with E. coli, sister chromatid exchange with cultured mammalian cells, and the micronucleus test with mice, as well as in an in vivo cytogenic study using mouse bone marrow.
There were no adverse effects on reproductive performance of male and female rats treated with up to 90 mg/kg/day of enalapril (26 times the MRHDD when compared on a body surface area basis).
Section 42228-7
Pregnancy
Section 42229-5
Hypertension
Administration of VASOTEC to patients with hypertension of severity ranging from mild to severe results in a reduction of both supine and standing blood pressure usually with no orthostatic component. Symptomatic postural hypotension is therefore infrequent, although it might be anticipated in volume-depleted patients (see WARNINGS, Hypotension ).
In most patients studied, after oral administration of a single dose of enalapril, onset of antihypertensive activity was seen at one hour with peak reduction of blood pressure achieved by four to six hours.
At recommended doses, antihypertensive effects have been maintained for at least 24 hours. In some patients the effects may diminish toward the end of the dosing interval (see DOSAGE AND ADMINISTRATION , Hypertension ).
In some patients achievement of optimal blood pressure reduction may require several weeks of therapy.
The antihypertensive effects of VASOTEC have continued during long-term therapy. Abrupt withdrawal of VASOTEC has not been associated with a rapid increase in blood pressure.
In hemodynamic studies in patients with essential hypertension, blood pressure reduction was accompanied by a reduction in peripheral arterial resistance with an increase in cardiac output and little or no change in heart rate. Following administration of VASOTEC, there is an increase in renal blood flow; glomerular filtration rate is usually unchanged. The effects appear to be similar in patients with renovascular hypertension.
When given together with thiazide-type diuretics, the blood pressure lowering effects of VASOTEC are approximately additive.
In a clinical pharmacology study, indomethacin or sulindac was administered to hypertensive patients receiving VASOTEC. In this study there was no evidence of a blunting of the antihypertensive action of VASOTEC (see PRECAUTIONS, Drug Interactions ).
Section 43679-0
Mechanism of Action
Enalapril, after hydrolysis to enalaprilat, inhibits angiotensin-converting enzyme (ACE) in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. The beneficial effects of enalapril in hypertension and heart failure appear to result primarily from suppression of the renin-angiotensin-aldosterone system. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. Although the latter decrease is small, it results in small increases of serum potassium. In hypertensive patients treated with VASOTEC alone for up to 48 weeks, mean increases in serum potassium of approximately 0.2 mEq/L were observed. In patients treated with VASOTEC plus a thiazide diuretic, there was essentially no change in serum potassium (see PRECAUTIONS ). Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of VASOTEC remains to be elucidated.
While the mechanism through which VASOTEC lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, VASOTEC is antihypertensive even in patients with low-renin hypertension. Although VASOTEC was antihypertensive in all races studied, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to enalapril monotherapy than non-black patients.
Section 43681-6
Pharmacodynamics and Clinical Effects
Section 43682-4
Pharmacokinetics and Metabolism
Following oral administration of VASOTEC, peak serum concentrations of enalapril occur within about one hour. Based on urinary recovery, the extent of absorption of enalapril is approximately 60 percent. Enalapril absorption is not influenced by the presence of food in the gastrointestinal tract. Following absorption, enalapril is hydrolyzed to enalaprilat, which is a more potent angiotensin-converting enzyme inhibitor than enalapril; enalaprilat is poorly absorbed when administered orally. Peak serum concentrations of enalaprilat occur three to four hours after an oral dose of enalapril maleate. Excretion of VASOTEC is primarily renal. Approximately 94 percent of the dose is recovered in the urine and feces as enalaprilat or enalapril. The principal components in urine are enalaprilat, accounting for about 40 percent of the dose, and intact enalapril. There is no evidence of metabolites of enalapril, other than enalaprilat.
The serum concentration profile of enalaprilat exhibits a prolonged terminal phase, apparently representing a small fraction of the administered dose that has been bound to ACE. The amount bound does not increase with dose, indicating a saturable site of binding. The effective half-life for accumulation of enalaprilat following multiple doses of enalapril maleate is 11 hours. The disposition of enalapril and enalaprilat in patients with renal insufficiency is similar to that in patients with normal renal function until the glomerular filtration rate is 30 mL/min or less. With glomerular filtration rate ≤30 mL/min, peak and trough enalaprilat levels increase, time to peak concentration increases and time to steady state may be delayed. The effective half-life of enalaprilat following multiple doses of enalapril maleate is prolonged at this level of renal insufficiency (see DOSAGE AND ADMINISTRATION ). Enalaprilat is dialyzable at the rate of 62 mL/min.
Studies in dogs indicate that enalapril crosses the blood-brain barrier poorly, if at all; enalaprilat does not enter the brain. Multiple doses of enalapril maleate in rats do not result in accumulation in any tissues. Milk of lactating rats contains radioactivity following administration of 14C-enalapril maleate. Radioactivity was found to cross the placenta following administration of labeled drug to pregnant hamsters.
Section 44425-7
Storage
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Keep container tightly closed.
Protect from moisture.
Dispense in a tight container as per USP, if product package is subdivided.
Overdosage
Limited data are available in regard to overdosage in humans.
Single oral doses of enalapril above 1,000 mg/kg and ≥1,775 mg/kg were associated with lethality in mice and rats, respectively.
The most likely manifestation of overdosage would be hypotension, for which the usual treatment would be intravenous infusion of normal saline solution.
Enalaprilat may be removed from general circulation by hemodialysis and has been removed from neonatal circulation by peritoneal dialysis (see WARNINGS, Anaphylactoid Reactions During Membrane Exposure ).
Fetal Toxicity
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue VASOTEC as soon as possible. These adverse outcomes are usually associated with use of these drugs in the second and third trimester of pregnancy. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents. Appropriate management of maternal hypertension during pregnancy is important to optimize outcomes for both mother and fetus.
In the unusual case that there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system for a particular patient, apprise the mother of the potential risk to the fetus. Perform serial ultrasound examinations to assess the intra-amniotic environment. If oligohydramnios is observed, discontinue VASOTEC, unless it is considered lifesaving for the mother. Fetal testing may be appropriate, based on the week of pregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury. Closely observe infants with histories of in utero exposure to VASOTEC for hypotension, oliguria, and hyperkalemia (see PRECAUTIONS, Pediatric Use ).
No teratogenic effects of enalapril were seen in studies of pregnant rats and rabbits. On a body surface area basis, the doses used were 57 times and 12 times, respectively, the maximum recommended human daily dose (MRHDD).
Warning: Fetal Toxicity
See full prescribing information for complete boxed warning.
-
•When pregnancy is detected, discontinue VASOTEC® as soon as possible.
-
•Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus (see WARNINGS, Fetal Toxicity).
Principal Display Panel 5 Mg Bottle Label
NDC 0187-0141-30
Rx only
Vasotec
®
(enalapril maleate)
Tablets
5 mg
30 Tablets
BAUSCH Health
Principal Display Panel 10 Mg Bottle Label
NDC 0187-0142-30
Vasotec
®
(enalapril maleate)
Tablets
10 mg
30 Tablets
BAUSCH Health
Principal Display Panel 20 Mg Bottle Label
NDC 0187-0143-30
Rx only
Vasotec
®
(enalapril maleate)
Tablets
20 mg
30 Tablets
BAUSCH Health
Principal Display Panel 2.5 Mg Bottle Label
NDC 0187-0140-30
Rx Only
Vasotec
®
(enalapril maleate)
Tablets
2.5 mg
30 Tablets
BAUSCH Health
Dual Blockade of the Renin Angiotensin System (ras)
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Most patients receiving the combination of two RAS inhibitors do not obtain any additional benefit compared to monotherapy. In general, avoid combined use of RAS inhibitors. Closely monitor blood pressure, renal function, and electrolytes in patients on VASOTEC and other agents that affect the RAS.
Do not coadminister aliskiren with VASOTEC in patients with diabetes. Avoid use of aliskiren with VASOTEC in patients with renal impairment (GFR <60 mL/min).
Structured Label Content
Contraindications (CONTRAINDICATIONS)
VASOTEC is contraindicated in patients who are hypersensitive to this product and in patients with a history of angioedema related to previous treatment with an angiotensin-converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema.
Do not coadminister aliskiren with VASOTEC in patients with diabetes (see PRECAUTIONS, Drug Interactions ).
VASOTEC is contraindicated in combination with a neprilysin inhibitor (e.g., sacubitril). Do not administer VASOTEC within 36 hours of switching to or from sacubitril/valsartan, a neprilysin inhibitor (see WARNINGS, Head and Neck Angioedema ).
Adverse Reactions (ADVERSE REACTIONS)
VASOTEC has been evaluated for safety in more than 10,000 patients, including over 1000 patients treated for one year or more. VASOTEC has been found to be generally well tolerated in controlled clinical trials involving 2987 patients. For the most part, adverse experiences were mild and transient in nature. In clinical trials, discontinuation of therapy due to clinical adverse experiences was required in 3.3 percent of patients with hypertension and in 5.7 percent of patients with heart failure. The frequency of adverse experiences was not related to total daily dosage within the usual dosage ranges. In patients with hypertension the overall percentage of patients treated with VASOTEC reporting adverse experiences was comparable to placebo.
How Supplied (HOW SUPPLIED)
|
VASOTEC (enalapril maleate) Tablets |
|||
|
NDC |
Strength |
Quantity |
Description |
|
0187-0140-30 0187-0140-90 |
2.5 mg |
Bottles of 30 Bottles of 90 |
White, oval shaped tablet imprinted with “VASO 2.5” and scored on one side and scored on the other. |
|
0187-0141-30 0187-0141-90 |
5 mg |
Bottles of 30 Bottles of 90 |
White, rounded triangle shaped tablet imprinted with “VASO 5” on one side and scored on the other. |
|
0187-0142-30 0187-0142-90 0187-0142-10 |
10 mg |
Bottles of 30 Bottles of 90 Bottles of 1,000 |
Rust red, rounded triangle shaped tablet imprinted with “VASO 10” on one side and scored on the other. |
|
0187-0143-30 0187-0143-90 0187-0143-10 |
20 mg |
Bottles of 30 Bottles of 90 Bottles of 1,000 |
Peach, rounded triangle shaped tablet imprinted with “VASO 20” on one side and scored on the other. |
Description (DESCRIPTION)
VASOTEC® (enalapril maleate) is the maleate salt of enalapril, the ethyl ester of a long-acting angiotensin-converting enzyme inhibitor, enalaprilat. Enalapril maleate is chemically described as (S)-1-[N-[1-(ethoxycarbonyl)-3-phenylpropyl]-L-alanyl]-L-proline, (Z)-2-butenedioate salt (1:1). Its empirical formula is C20H28N2O5•C4H4O4, and its structural formula is:
Enalapril maleate is a white to off-white, crystalline powder with a molecular weight of 492.53. It is sparingly soluble in water, soluble in ethanol, and freely soluble in methanol.
Enalapril is a pro-drug; following oral administration, it is bioactivated by hydrolysis of the ethyl ester to enalaprilat, which is the active angiotensin-converting enzyme inhibitor.
Enalapril maleate is supplied as 2.5 mg, 5 mg, 10 mg, and 20 mg tablets for oral administration. In addition to the active ingredient enalapril maleate, each tablet contains the following inactive ingredients: lactose, magnesium stearate, sodium bicarbonate, and starch. The 10 mg and 20 mg tablets also contain iron oxides.
Section 34072-9 (34072-9)
General
Section 34073-7 (34073-7)
Drug Interactions
Neprilysin Inhibitors
Patients taking concomitant neprilysin inhibitors may be at increased risk for angioedema (see WARNINGS ).
Section 34076-0 (34076-0)
Information for Patients
Section 34080-2 (34080-2)
Nursing Mothers
Enalapril and enalaprilat have been detected in human breast milk. Because of the potential for serious adverse reactions in nursing infants from enalapril, a decision should be made whether to discontinue nursing or to discontinue VASOTEC, taking into account the importance of the drug to the mother.
Section 34081-0 (34081-0)
Pediatric Use
Section 34083-6 (34083-6)
Carcinogenesis, Mutagenesis, Impairment of Fertility
There was no evidence of a tumorigenic effect when enalapril was administered for 106 weeks to male and female rats at doses up to 90 mg/kg/day or for 94 weeks to male and female mice at doses up to 90 and 180 mg/kg/day, respectively. These doses are 26 times (in rats and female mice) and 13 times (in male mice) the maximum recommended human daily dose (MRHDD) when compared on a body surface area basis.
Neither enalapril maleate nor the active diacid was mutagenic in the Ames microbial mutagen test with or without metabolic activation. Enalapril was also negative in the following genotoxicity studies: rec-assay, reverse mutation assay with E. coli, sister chromatid exchange with cultured mammalian cells, and the micronucleus test with mice, as well as in an in vivo cytogenic study using mouse bone marrow.
There were no adverse effects on reproductive performance of male and female rats treated with up to 90 mg/kg/day of enalapril (26 times the MRHDD when compared on a body surface area basis).
Section 42228-7 (42228-7)
Pregnancy
Section 42229-5 (42229-5)
Hypertension
Administration of VASOTEC to patients with hypertension of severity ranging from mild to severe results in a reduction of both supine and standing blood pressure usually with no orthostatic component. Symptomatic postural hypotension is therefore infrequent, although it might be anticipated in volume-depleted patients (see WARNINGS, Hypotension ).
In most patients studied, after oral administration of a single dose of enalapril, onset of antihypertensive activity was seen at one hour with peak reduction of blood pressure achieved by four to six hours.
At recommended doses, antihypertensive effects have been maintained for at least 24 hours. In some patients the effects may diminish toward the end of the dosing interval (see DOSAGE AND ADMINISTRATION , Hypertension ).
In some patients achievement of optimal blood pressure reduction may require several weeks of therapy.
The antihypertensive effects of VASOTEC have continued during long-term therapy. Abrupt withdrawal of VASOTEC has not been associated with a rapid increase in blood pressure.
In hemodynamic studies in patients with essential hypertension, blood pressure reduction was accompanied by a reduction in peripheral arterial resistance with an increase in cardiac output and little or no change in heart rate. Following administration of VASOTEC, there is an increase in renal blood flow; glomerular filtration rate is usually unchanged. The effects appear to be similar in patients with renovascular hypertension.
When given together with thiazide-type diuretics, the blood pressure lowering effects of VASOTEC are approximately additive.
In a clinical pharmacology study, indomethacin or sulindac was administered to hypertensive patients receiving VASOTEC. In this study there was no evidence of a blunting of the antihypertensive action of VASOTEC (see PRECAUTIONS, Drug Interactions ).
Section 43679-0 (43679-0)
Mechanism of Action
Enalapril, after hydrolysis to enalaprilat, inhibits angiotensin-converting enzyme (ACE) in human subjects and animals. ACE is a peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor substance, angiotensin II. Angiotensin II also stimulates aldosterone secretion by the adrenal cortex. The beneficial effects of enalapril in hypertension and heart failure appear to result primarily from suppression of the renin-angiotensin-aldosterone system. Inhibition of ACE results in decreased plasma angiotensin II, which leads to decreased vasopressor activity and to decreased aldosterone secretion. Although the latter decrease is small, it results in small increases of serum potassium. In hypertensive patients treated with VASOTEC alone for up to 48 weeks, mean increases in serum potassium of approximately 0.2 mEq/L were observed. In patients treated with VASOTEC plus a thiazide diuretic, there was essentially no change in serum potassium (see PRECAUTIONS ). Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity.
ACE is identical to kininase, an enzyme that degrades bradykinin. Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of VASOTEC remains to be elucidated.
While the mechanism through which VASOTEC lowers blood pressure is believed to be primarily suppression of the renin-angiotensin-aldosterone system, VASOTEC is antihypertensive even in patients with low-renin hypertension. Although VASOTEC was antihypertensive in all races studied, black hypertensive patients (usually a low-renin hypertensive population) had a smaller average response to enalapril monotherapy than non-black patients.
Section 43681-6 (43681-6)
Pharmacodynamics and Clinical Effects
Section 43682-4 (43682-4)
Pharmacokinetics and Metabolism
Following oral administration of VASOTEC, peak serum concentrations of enalapril occur within about one hour. Based on urinary recovery, the extent of absorption of enalapril is approximately 60 percent. Enalapril absorption is not influenced by the presence of food in the gastrointestinal tract. Following absorption, enalapril is hydrolyzed to enalaprilat, which is a more potent angiotensin-converting enzyme inhibitor than enalapril; enalaprilat is poorly absorbed when administered orally. Peak serum concentrations of enalaprilat occur three to four hours after an oral dose of enalapril maleate. Excretion of VASOTEC is primarily renal. Approximately 94 percent of the dose is recovered in the urine and feces as enalaprilat or enalapril. The principal components in urine are enalaprilat, accounting for about 40 percent of the dose, and intact enalapril. There is no evidence of metabolites of enalapril, other than enalaprilat.
The serum concentration profile of enalaprilat exhibits a prolonged terminal phase, apparently representing a small fraction of the administered dose that has been bound to ACE. The amount bound does not increase with dose, indicating a saturable site of binding. The effective half-life for accumulation of enalaprilat following multiple doses of enalapril maleate is 11 hours. The disposition of enalapril and enalaprilat in patients with renal insufficiency is similar to that in patients with normal renal function until the glomerular filtration rate is 30 mL/min or less. With glomerular filtration rate ≤30 mL/min, peak and trough enalaprilat levels increase, time to peak concentration increases and time to steady state may be delayed. The effective half-life of enalaprilat following multiple doses of enalapril maleate is prolonged at this level of renal insufficiency (see DOSAGE AND ADMINISTRATION ). Enalaprilat is dialyzable at the rate of 62 mL/min.
Studies in dogs indicate that enalapril crosses the blood-brain barrier poorly, if at all; enalaprilat does not enter the brain. Multiple doses of enalapril maleate in rats do not result in accumulation in any tissues. Milk of lactating rats contains radioactivity following administration of 14C-enalapril maleate. Radioactivity was found to cross the placenta following administration of labeled drug to pregnant hamsters.
Section 44425-7 (44425-7)
Storage
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Keep container tightly closed.
Protect from moisture.
Dispense in a tight container as per USP, if product package is subdivided.
Overdosage (OVERDOSAGE)
Limited data are available in regard to overdosage in humans.
Single oral doses of enalapril above 1,000 mg/kg and ≥1,775 mg/kg were associated with lethality in mice and rats, respectively.
The most likely manifestation of overdosage would be hypotension, for which the usual treatment would be intravenous infusion of normal saline solution.
Enalaprilat may be removed from general circulation by hemodialysis and has been removed from neonatal circulation by peritoneal dialysis (see WARNINGS, Anaphylactoid Reactions During Membrane Exposure ).
Fetal Toxicity
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue VASOTEC as soon as possible. These adverse outcomes are usually associated with use of these drugs in the second and third trimester of pregnancy. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents. Appropriate management of maternal hypertension during pregnancy is important to optimize outcomes for both mother and fetus.
In the unusual case that there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system for a particular patient, apprise the mother of the potential risk to the fetus. Perform serial ultrasound examinations to assess the intra-amniotic environment. If oligohydramnios is observed, discontinue VASOTEC, unless it is considered lifesaving for the mother. Fetal testing may be appropriate, based on the week of pregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury. Closely observe infants with histories of in utero exposure to VASOTEC for hypotension, oliguria, and hyperkalemia (see PRECAUTIONS, Pediatric Use ).
No teratogenic effects of enalapril were seen in studies of pregnant rats and rabbits. On a body surface area basis, the doses used were 57 times and 12 times, respectively, the maximum recommended human daily dose (MRHDD).
Warning: Fetal Toxicity (WARNING: FETAL TOXICITY)
See full prescribing information for complete boxed warning.
-
•When pregnancy is detected, discontinue VASOTEC® as soon as possible.
-
•Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus (see WARNINGS, Fetal Toxicity).
Principal Display Panel 5 Mg Bottle Label (PRINCIPAL DISPLAY PANEL - 5 mg Bottle Label)
NDC 0187-0141-30
Rx only
Vasotec
®
(enalapril maleate)
Tablets
5 mg
30 Tablets
BAUSCH Health
Principal Display Panel 10 Mg Bottle Label (PRINCIPAL DISPLAY PANEL - 10 mg Bottle Label)
NDC 0187-0142-30
Vasotec
®
(enalapril maleate)
Tablets
10 mg
30 Tablets
BAUSCH Health
Principal Display Panel 20 Mg Bottle Label (PRINCIPAL DISPLAY PANEL - 20 mg Bottle Label)
NDC 0187-0143-30
Rx only
Vasotec
®
(enalapril maleate)
Tablets
20 mg
30 Tablets
BAUSCH Health
Principal Display Panel 2.5 Mg Bottle Label (PRINCIPAL DISPLAY PANEL - 2.5 mg Bottle Label)
NDC 0187-0140-30
Rx Only
Vasotec
®
(enalapril maleate)
Tablets
2.5 mg
30 Tablets
BAUSCH Health
Dual Blockade of the Renin Angiotensin System (ras) (Dual Blockade of the Renin-Angiotensin System (RAS))
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Most patients receiving the combination of two RAS inhibitors do not obtain any additional benefit compared to monotherapy. In general, avoid combined use of RAS inhibitors. Closely monitor blood pressure, renal function, and electrolytes in patients on VASOTEC and other agents that affect the RAS.
Do not coadminister aliskiren with VASOTEC in patients with diabetes. Avoid use of aliskiren with VASOTEC in patients with renal impairment (GFR <60 mL/min).
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:52:45.189574 · Updated: 2026-03-14T22:44:32.835928