Lunsumio
2ef0cf38-101c-4681-98fe-c05dc9ead443
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
LUNSUMIO is a bispecific CD20-directed CD3 T-cell engager indicated for the treatment of adult patients with relapsed or refractory follicular lymphoma after two or more lines of systemic therapy. This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). ( 1.1 )
Dosage and Administration
LUNSUMIO and LUNSUMIO VELO have different dosage and administration instructions. Administer LUNSUMIO only as an intravenous infusion. ( 2.1 ) Premedicate to reduce risk of CRS and infusion-related reactions. ( 2.3 , 5.1 ) Recommended dosage for LUNSUMIO for intravenous infusion ( 2.2 ): Day of Treatment Cycle length = 21 days Intravenous Dose of LUNSUMIO Rate of Infusion Cycle 1 Day 1 1 mg Administer over a minimum of 4 hours. Day 8 2 mg Day 15 60 mg Cycle 2 Day 1 60 mg Administer over 2 hours if infusions from Cycle 1 were well-tolerated. Cycles 3+ Day 1 30 mg See Full Prescribing Information for instructions on preparation and administration. ( 2.5 )
Contraindications
None.
Warnings and Precautions
Neurologic Toxicity, including Immune Effector Cell-Associated Neurotoxicity Syndrome : Can cause serious and life-threatening neurologic toxicity, including immune effector cell-associated neurotoxicity syndrome (ICANS). Monitor patients for signs and symptoms of neurologic toxicity during treatment; withhold or permanently discontinue based on severity. ( 5.2 ) Infections : Can cause serious or fatal infections. Monitor patients for signs and symptoms of infection, including opportunistic infections, and treat as needed. ( 5.3 ) Hemophagocytic Lymphohistiocytosis: Can cause serious or fatal reactions. For suspected cases, interrupt LUNSUMIO and evaluate and treat promptly. ( 5.4 ) Cytopenias : Monitor complete blood cell counts during treatment. ( 5.5 ) Tumor Flare : Can cause serious tumor flare reactions. Monitor patients at risk for complications of tumor flare. ( 5.6 ) Risk of Medication Errors with Incorrect Product Use : Ensure that the correct formulation is being prescribed, dispensed, and administered. ( 5.7 ) Embryo-Fetal Toxicity : May cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception. ( 5.8 , 8.1 , 8.3 )
Adverse Reactions
The following adverse reactions are described elsewhere in the labeling: Cytokine Release Syndrome [see Warnings and Precautions (5.1) ] Neurologic Toxicity, including Immune Effector Cell-associated Neurotoxicity Syndrome [see Warnings and Precautions (5.2) ] Infections [see Warnings and Precautions (5.3) ] Hemophagocytic Lymphohistiocytosis [see Warnings and Precautions (5.4) ] Cytopenias [see Warnings and Precautions (5.5) ] Tumor Flare [see Warnings and Precautions (5.6) ]
How Supplied
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, colorless, preservative-free solution for intravenous infusion supplied as follows: One 1 mg/mL single-dose vial in a carton (NDC 50242-159-01) One 30 mg/30 mL (1 mg/mL) single-dose vial in a carton (NDC 50242-142-01).
Storage and Handling
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, colorless, preservative-free solution for intravenous infusion supplied as follows: One 1 mg/mL single-dose vial in a carton (NDC 50242-159-01) One 30 mg/30 mL (1 mg/mL) single-dose vial in a carton (NDC 50242-142-01).
Description
Cytokine release syndrome (CRS), including serious or life-threatening reactions, can occur in patients receiving LUNSUMIO. Initiate treatment with the LUNSUMIO step-up dosing schedule to reduce the risk of CRS. Withhold LUNSUMIO until CRS resolves or permanently discontinue based on severity [see Dosage and Administration (2.1 and 2.4) and Warnings and Precautions (5.1) ] .
Medication Information
Warnings and Precautions
Neurologic Toxicity, including Immune Effector Cell-Associated Neurotoxicity Syndrome : Can cause serious and life-threatening neurologic toxicity, including immune effector cell-associated neurotoxicity syndrome (ICANS). Monitor patients for signs and symptoms of neurologic toxicity during treatment; withhold or permanently discontinue based on severity. ( 5.2 ) Infections : Can cause serious or fatal infections. Monitor patients for signs and symptoms of infection, including opportunistic infections, and treat as needed. ( 5.3 ) Hemophagocytic Lymphohistiocytosis: Can cause serious or fatal reactions. For suspected cases, interrupt LUNSUMIO and evaluate and treat promptly. ( 5.4 ) Cytopenias : Monitor complete blood cell counts during treatment. ( 5.5 ) Tumor Flare : Can cause serious tumor flare reactions. Monitor patients at risk for complications of tumor flare. ( 5.6 ) Risk of Medication Errors with Incorrect Product Use : Ensure that the correct formulation is being prescribed, dispensed, and administered. ( 5.7 ) Embryo-Fetal Toxicity : May cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception. ( 5.8 , 8.1 , 8.3 )
Indications and Usage
LUNSUMIO is a bispecific CD20-directed CD3 T-cell engager indicated for the treatment of adult patients with relapsed or refractory follicular lymphoma after two or more lines of systemic therapy. This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). ( 1.1 )
Dosage and Administration
LUNSUMIO and LUNSUMIO VELO have different dosage and administration instructions. Administer LUNSUMIO only as an intravenous infusion. ( 2.1 ) Premedicate to reduce risk of CRS and infusion-related reactions. ( 2.3 , 5.1 ) Recommended dosage for LUNSUMIO for intravenous infusion ( 2.2 ): Day of Treatment Cycle length = 21 days Intravenous Dose of LUNSUMIO Rate of Infusion Cycle 1 Day 1 1 mg Administer over a minimum of 4 hours. Day 8 2 mg Day 15 60 mg Cycle 2 Day 1 60 mg Administer over 2 hours if infusions from Cycle 1 were well-tolerated. Cycles 3+ Day 1 30 mg See Full Prescribing Information for instructions on preparation and administration. ( 2.5 )
Contraindications
None.
Adverse Reactions
The following adverse reactions are described elsewhere in the labeling: Cytokine Release Syndrome [see Warnings and Precautions (5.1) ] Neurologic Toxicity, including Immune Effector Cell-associated Neurotoxicity Syndrome [see Warnings and Precautions (5.2) ] Infections [see Warnings and Precautions (5.3) ] Hemophagocytic Lymphohistiocytosis [see Warnings and Precautions (5.4) ] Cytopenias [see Warnings and Precautions (5.5) ] Tumor Flare [see Warnings and Precautions (5.6) ]
Storage and Handling
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, colorless, preservative-free solution for intravenous infusion supplied as follows: One 1 mg/mL single-dose vial in a carton (NDC 50242-159-01) One 30 mg/30 mL (1 mg/mL) single-dose vial in a carton (NDC 50242-142-01).
How Supplied
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, colorless, preservative-free solution for intravenous infusion supplied as follows: One 1 mg/mL single-dose vial in a carton (NDC 50242-159-01) One 30 mg/30 mL (1 mg/mL) single-dose vial in a carton (NDC 50242-142-01).
Description
Cytokine release syndrome (CRS), including serious or life-threatening reactions, can occur in patients receiving LUNSUMIO. Initiate treatment with the LUNSUMIO step-up dosing schedule to reduce the risk of CRS. Withhold LUNSUMIO until CRS resolves or permanently discontinue based on severity [see Dosage and Administration (2.1 and 2.4) and Warnings and Precautions (5.1) ] .
Section 42229-5
Dosage Modifications for Cytokine Release Syndrome
Identify CRS based on clinical presentation [see Warnings and Precautions (5.1)]. Evaluate for and treat other causes of fever, hypoxia, and hypotension.
If CRS is suspected, withhold LUNSUMIO until CRS resolves, manage according to the recommendations in Table 4 and per current practice guidelines. Administer supportive therapy for CRS, which may include intensive care for severe or life-threatening CRS.
| Grade Based on American Society for Transplantation and Cellular Therapy (ASTCT) 2019 grading for CRS.
|
Presenting Symptoms | Actions If CRS is refractory to management, consider other causes including hemophagocytic lymphohistiocytosis [see Warnings and Precautions (5.4)].
|
|---|---|---|
| Grade 1 | Fever ≥ 100.4°F (38°C) Premedication may mask fever, therefore if clinical presentation is consistent with CRS, follow these management guidelines.
|
|
| Grade 2 | Fever ≥ 100.4°F (38°C) with: Hypotension not requiring vasopressors and/or hypoxia requiring low-flow oxygen Low-flow oxygen defined as oxygen delivered at < 6 L/minute; high-flow oxygen defined as oxygen delivered at ≥ 6 L/minute. by nasal cannula or blow-by. |
|
Recurrent Grade 2 CRS
|
||
| Grade 3 | Fever ≥ 100.4°F (38°C) with: Hypotension requiring a vasopressor (with or without vasopressin) and/or hypoxia requiring high flow oxygen by nasal cannula, face mask, non-rebreather mask, or Venturi mask. |
|
Recurrent Grade 3 CRS
|
||
| Grade 4 | Fever ≥ 100.4°F (38°C) with: Hypotension requiring multiple vasopressors (excluding vasopressin) and/or hypoxia requiring oxygen by positive pressure (e.g., CPAP, BiPAP, intubation and mechanical ventilation). |
|
Section 42231-1
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: Dec 2025 | |
|
MEDICATION GUIDE LUNSUMIO® (lun-SUM-mee-oh) (mosunetuzumab-axgb) injection, for intravenous infusion |
||
|
What is the most important information I should know about LUNSUMIO? Get medical help right away if you develop any signs or symptoms of CRS at any time, including: |
||
|
|
|
Due to the risk of CRS, you will receive LUNSUMIO on a "step-up dosing schedule".
|
||
| Your healthcare provider will check you for CRS during treatment with LUNSUMIO and may treat you in a hospital if you develop signs and symptoms of CRS. Your healthcare provider may temporarily stop or completely stop your treatment with LUNSUMIO if you have severe side effects. See "What are the possible side effects of LUNSUMIO?" for more information about side effects. |
||
|
What is LUNSUMIO?
LUNSUMIO is a prescription medicine used to treat adults with follicular lymphoma whose cancer has come back or did not respond to previous treatment, and who have already received two or more treatments for their cancer. It is not known if LUNSUMIO is safe and effective in children. |
||
Before receiving LUNSUMIO, tell your healthcare provider about all of your medical conditions, including if you:
|
||
|
How will I receive LUNSUMIO?
|
||
|
What should I avoid while receiving LUNSUMIO?
Do not drive, operate heavy machinery, or do other dangerous activities if you develop dizziness, confusion, tremors, sleepiness, or any other symptoms that impair consciousness until your signs and symptoms go away. These may be signs and symptoms of CRS or neurologic problems. See "What is the most important information I should know about LUNSUMIO?" and "What are the possible side effects of LUNSUMIO?" for more information about signs and symptoms of CRS and neurologic problems. |
||
|
What are the possible side effects of LUNSUMIO?
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
Your healthcare provider may temporarily stop or permanently stop treatment with LUNSUMIO if you develop severe side effects. The most common side effects of LUNSUMIO include: |
||
|
|
|
|
The most common severe abnormal blood test results with LUNSUMIO include: decreased blood cell counts, decreased phosphate, increased glucose, and increased uric acid levels. These are not all the possible side effects of LUNSUMIO. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
||
|
General information about the safe and effective use of LUNSUMIO.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. You can ask your pharmacist or healthcare provider for information about LUNSUMIO that is written for health professionals. |
||
|
What are the ingredients in LUNSUMIO? Active ingredient: mosunetuzumab-axgb Inactive ingredients: acetic acid, histidine, methionine, polysorbate 20, sucrose, and Water for Injection Manufactured by: Genentech, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 U.S. License No.: 1048 LUNSUMIO is a registered trademark of Genentech, Inc. For more information, call 1-844-832-3687 or go to www.LUNSUMIO.com. |
Section 43683-2
Section 44425-7
Store refrigerated at 2°C to 8°C (36°F to 46°F) in the original carton to protect from light.
Do not freeze. Do not shake.
11 Description
Mosunetuzumab-axgb is a bispecific CD20-directed CD3 T-cell engager. It is a humanized monoclonal anti-CD20xCD3 T-cell-dependent bispecific antibody of the immunoglobulin G1 (IgG1) isotype. Mosunetuzumab-axgb is produced in Chinese Hamster Ovary (CHO) cells by recombinant DNA technology. The approximate molecular weight is 146 kDa.
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, preservative-free, colorless solution for intravenous use.
Each single-dose vial contains a 1 mL solution of mosunetuzumab-axgb (1 mg), acetic acid (0.4 mg), histidine (1.6 mg), methionine (1.5 mg), polysorbate 20 (0.6 mg), sucrose (82.1 mg), and Water for Injection, USP. The pH is 5.8.
Each single-dose vial contains a 30 mL solution of mosunetuzumab-axgb (30 mg), acetic acid (12.8 mg), histidine (46.6 mg), methionine (44.8 mg), polysorbate 20 (18 mg), sucrose (2,462.4 mg), and Water for Injection, USP. The pH is 5.8.
5.3 Infections
LUNSUMIO can cause serious or fatal infections [see Adverse Reactions (6.1)].
Among patients who received LUNSUMIO at the recommended dosage in the clinical trial, serious infections, including opportunistic infections, occurred in 17%, with Grade 3 or 4 infections in 14% and fatal infections in 0.9% of patients. The most common Grade 3 or greater infections were pneumonia, sepsis, and upper respiratory infection.
Monitor patients for signs and symptoms of infection prior to and during treatment with LUNSUMIO and treat appropriately. LUNSUMIO should not be administered in the presence of active infection. Caution should be exercised when considering the use of LUNSUMIO in patients with a history of recurring or chronic infections (e.g., chronic, active Epstein-Barr Virus), with underlying conditions that may predispose to infections or who have had significant prior immunosuppressive treatment. Administer prophylactic antimicrobials according to guidelines.
Withhold LUNSUMIO or consider permanent discontinuation of LUNSUMIO based on severity [see Dosage and Administration (2.4)].
5.5 Cytopenias
LUNSUMIO can cause serious or severe cytopenias, including lymphopenia, neutropenia, anemia, and thrombocytopenia [see Adverse Reactions (6.1)].
Among patients who received LUNSUMIO at the recommended dosage in the clinical trial, Grade 3 or 4 decreased lymphocytes occurred in 92%, decreased neutrophils in 38%, decreased hemoglobin in 19%, and decreased platelets in 12% of patients. Grade 4 decreased lymphocytes occurred in 71%, decreased neutrophils in 19%, and decreased platelets in 5% of patients. Febrile neutropenia occurred in 2% of patients.
Monitor complete blood counts throughout treatment. Based on the severity of cytopenias, temporarily withhold, or permanently discontinue LUNSUMIO. Consider prophylactic granulocyte colony-stimulating factor administration as applicable [see Dosage and Administration (2.4)].
5.6 Tumor Flare
LUNSUMIO can cause serious or severe tumor flare [see Adverse Reactions (6.1)].
Among patients who received LUNSUMIO at the recommended dosage in the clinical trial, tumor flare occurred in 4%. Manifestations included new or worsening pleural effusions, localized pain and swelling at the sites of lymphoma lesions, and tumor inflammation.
Patients with bulky tumors or disease located in close proximity to airways or a vital organ should be monitored closely during initial therapy. Monitor for signs and symptoms of compression or obstruction due to mass effect secondary to tumor flare. If compression or obstruction develops, institute standard treatment of these complications.
8.4 Pediatric Use
The safety and efficacy of LUNSUMIO have not been established in pediatric patients.
8.5 Geriatric Use
Among the 90 patients with relapsed or refractory follicular lymphoma treated with LUNSUMIO, 33% were 65 years of age or older, and 8% were 75 years of age or older. There is an insufficient number of patients 65 years of age or older and 75 years of age or older to assess whether there are differences in safety or effectiveness in patients 65 years of age and older compared to younger adult patients.
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the study described below with the incidence of anti-drug antibodies in other studies, including those of mosunetuzumab-axgb.
During treatment in Study GO29781 (up to 12 months) [see Clinical Studies (14)], using an enzyme-linked immunosorbent assay (ELISA), no patients (N = 418) treated with LUNSUMIO developed anti-mosunetuzumab-axgb antibodies. Based on these data, the clinical relevance of anti-mosunetuzumab-axgb antibodies could not be assessed.
14 Clinical Studies
The efficacy of LUNSUMIO was evaluated in an open-label, multicenter, multi-cohort study (GO29781, NCT02500407) in patients with relapsed or refractory follicular lymphoma (FL) who had received at least two prior therapies, including an anti-CD20 monoclonal antibody and an alkylating agent. The study excluded patients with active infections, history of autoimmune disease, prior allogeneic transplant, or any history of CNS lymphoma or CNS disorders.
Patients received step-up doses of 1 mg on Cycle 1 Day 1 and 2 mg on Cycle 1 Day 8, followed by 60 mg on Cycle 1 Day 15, and 60 mg on Cycle 2 Day 1, then 30 mg via intravenous infusion every 3 weeks in subsequent cycles. A treatment cycle was 21 days. LUNSUMIO was administered for 8 cycles unless patients experienced progressive disease or unacceptable toxicity. After 8 cycles, patients with a complete response discontinued therapy; patients with a partial response or stable disease continued treatment up to 17 cycles, unless patients experienced progressive disease or unacceptable toxicity.
Among the 90 patients with relapsed or refractory FL, the median age was 60 years (range: 29 to 90 years), 33% were 65 years of age or older, 61% were male, 82% were White, 9% were Asian, 4% were Black or African American, and 8% were Hispanic or Latino. A total of 77% of patients had Stage III-IV disease, 34% had bulky disease, and all patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. The median number of prior therapies was 3 (range: 2 to 10), with 38% receiving 2 prior therapies, 31% receiving 3 prior therapies, and 31% receiving more than 3 prior therapies.
Seventy-nine percent of patients were refractory to prior anti-CD20 monoclonal antibody therapy, 53% were refractory to both anti-CD20 monoclonal antibody and alkylator therapy, 9% received prior rituximab plus lenalidomide therapy, 21% received prior autologous stem cell transplant, and 3% received prior CAR-T therapy. Fifty-two percent of patients had progression of disease within 24 months of first systemic therapy.
Efficacy was established on the basis of objective response rate (ORR) and duration of response (DOR) as assessed by an independent review facility according to standard criteria for NHL (Cheson 2007). The median follow-up for DOR was 14.9 months. The efficacy results are summarized in Table 12.
| Response | LUNSUMIO N = 90 |
|---|---|
| CI = confidence interval; NR = not reached | |
| Objective response rate (ORR), n (%) | 72 (80) |
| (95% CI) | (70, 88) |
| Complete response (CR), n (%) | 54 (60) |
| (95% CI) | (49, 70) |
| Partial response (PR), n (%) | 18 (20) |
| (95% CI) | (12, 30) |
| Duration of response (DOR) | N = 72 |
| Median DOR DOR is defined as the time from the initial occurrence of a documented PR or CR until the patient experienced an event (documented disease progression or death due to any cause).
,
Kaplan-Meier estimate. , months (95% CI) |
22.8 (10, NR) |
| Rate of continued response | |
| At 12 months, % | 62 |
| (95% CI) | (50, 74) |
| At 18 months, % | 57 |
| (95% CI) | (44, 70) |
The median time to first response was 1.4 months (range: 1.1 to 8.9).
4 Contraindications
None.
6 Adverse Reactions
The following adverse reactions are described elsewhere in the labeling:
- Cytokine Release Syndrome [see Warnings and Precautions (5.1)]
- Neurologic Toxicity, including Immune Effector Cell-associated Neurotoxicity Syndrome [see Warnings and Precautions (5.2)]
- Infections [see Warnings and Precautions (5.3)]
- Hemophagocytic Lymphohistiocytosis [see Warnings and Precautions (5.4)]
- Cytopenias [see Warnings and Precautions (5.5)]
- Tumor Flare [see Warnings and Precautions (5.6)]
12.2 Pharmacodynamics
After intravenous administration of the recommended dosage of LUNSUMIO, peripheral B-cell counts decreased to undetectable levels (< 5 cells/microliter) in most patients (95%) by Cycle 2 Day 1 and the depletion was sustained at later cycles including at Cycle 4 and Cycle 8.
LUNSUMIO caused hypogammaglobulinemia (defined as IgG levels < 500 mg/dL). Among 67 patients with baseline IgG levels ≥ 500 mg/dL, 40% had their IgG level decreased to < 500 mg/dL after administration of the recommended dosage of LUNSUMIO.
Plasma concentrations of cytokines (IL-2, IL-6, IL-10, TNF-α, and IFN-γ) were measured, and transient elevation of cytokines were observed at doses of 0.4 mg and above. After administration of the recommended dosage of LUNSUMIO, the highest elevation of cytokines was observed within 24 hours after the first dose on Cycle 1 Day 1 and after the first 60 mg dose on Cycle 1 Day 15. The elevated cytokine levels generally returned to baseline prior to the next infusion on Cycle 1 Day 8 and on Cycle 2 Day 1.
12.3 Pharmacokinetics
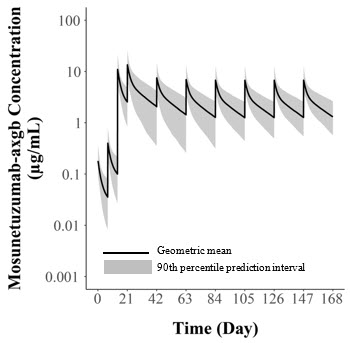
Mosunetuzumab-axgb PK exposure increased proportionally over a dose range from 0.2 mg to 60 mg (0.007 to 2 times the recommended treatment dosage). PK exposures for the recommended dosage of LUNSUMIO are summarized in Table 10 and Figure 1.
| AUC (day∙μg/mL) Values are geometric mean with geometric CV%.
|
Cmax (μg/mL) | Ctrough (μg/mL) | |
|---|---|---|---|
| All values reported are model-predicted exposure metrics. | |||
| Cycle 1 (0 ‒ 21 days) | 35.2 (36.6) | 11.1 (36.7) | 2.6 (54.0) |
| Cycle 2 (21 ‒ 42 days) | 90.3 (48.5) | 13.6 (37.7) | 2.0 (83.1) |
| Cycle 3 (42 – 63 days) | 59.0 (48.9) | 7.6 (40.1) | 1.4 (75.6) |
| Steady state Steady state values are approximated at Cycle 4 (63 ‒ 84 days).
|
52.9 (40.7) | 7.0 (37.9) | 1.3 (59.9) |
Figure 1. Model-Predicted Mosunetuzumab-axgb Intravenous Infusion Concentration Time Profile
Pharmacokinetic parameters (Table 11) were evaluated at the recommended dosage and are presented as geometric mean (CV%) unless otherwise specified.
| Parameter | LUNSUMIO via Intravenous Infusion |
|---|---|
| Tmax = time to peak concentration | |
| Tmax median (range), hours Steady-state.
|
4.0 (4.0 – 4.0) Tmax is at the end of intravenous infusion.
|
| Volume of distributiona (L) | 5.5 (31%) |
| Half-lifea (days) | 16.1 (17%) |
| Systemic clearance (L/day) | 1.1 (63%) at baseline 0.58 (18%) at steady state |
2.2 Recommended Dosage
The recommended dosage for LUNSUMIO intravenous infusion is presented in Table 1.
Administer for 8 cycles, unless patients experience unacceptable toxicity or disease progression.
For patients who achieve a complete response, no further treatment beyond 8 cycles is required. For patients who achieve a partial response or have stable disease in response to treatment with LUNSUMIO after 8 cycles, an additional 9 cycles of treatment (17 cycles total) should be administered, unless a patient experiences unacceptable toxicity or disease progression.
| Day of Treatment | Intravenous Dose of LUNSUMIO | Rate of Infusion | |
|---|---|---|---|
| Cycle 1 | Day 1 | 1 mg | Administer over a minimum of 4 hours. |
| Day 8 | 2 mg | ||
| Day 15 | 60 mg | ||
| Cycle 2 | Day 1 | 60 mg | Administer over 2 hours if infusions from Cycle 1 were well-tolerated. |
| Cycles 3+ | Day 1 | 30 mg |
| Last Intravenous Dose Administered | Time Since Last Dose Administered | Action for Next Intravenous Dose(s) |
|---|---|---|
| 1 mg Cycle 1 Day 1 |
1week to 2 weeks | Administer 2 mg (Cycle 1 Day 8), then resume the planned treatment schedule. |
| Greater than 2 weeks | Repeat 1 mg (Cycle 1 Day 1), then administer 2 mg (Cycle 1 Day 8) and resume the planned treatment schedule. | |
| 2 mg Cycle 1 Day 8 |
1 week to 2 weeks | Administer 60 mg (Cycle 1 Day 15), then resume the planned treatment schedule. |
| Greater than 2 weeks to less than 6 weeks | Repeat 2 mg (Cycle 1 Day 8), then administer 60 mg (Cycle 1 Day 15) and resume the planned treatment schedule. | |
| Greater than or equal to 6 weeks | Repeat 1 mg (Cycle 1 Day 1) and 2 mg (Cycle 1 Day 8), then administer 60 mg (Cycle 1 Day 15) and resume the planned treatment schedule. | |
| 60 mg Cycle 1 Day 15 |
1 week to less than 6 weeks | Administer 60 mg (Cycle 2 Day 1), then resume the planned treatment schedule. |
| Greater than or equal to 6 weeks | Repeat 1 mg (Cycle 2 Day 1) and 2 mg (Cycle 2 Day 8), then administer 60 mg (Cycle 2 Day 15), followed by 30 mg (Cycle 3 Day 1) and then resume the planned treatment schedule. | |
| 60 mg Cycle 2 Day 1 |
3 weeks to less than 6 weeks | Administer 30 mg (Cycle 3 Day 1), then resume the planned treatment schedule. |
| Greater than or equal to 6 weeks | Repeat 1 mg (Cycle 3 Day 1) and 2 mg (Cycle 3 Day 8), then administer 30 mg (Cycle 3 Day 15) For the Day 1, Day 8, and Day 15 doses in the next cycle, administer premedication as per Table 3 for all patients. , followed by 30 mg (Cycle 4 Day 1) and then resume the planned treatment schedule. |
|
| 30 mg Cycle 3 onwards |
3 weeks to less than 6 weeks | Administer 30 mg, then resume the planned treatment schedule. |
| Greater than or equal to 6 weeks | Repeat 1 mg on Day 1 and 2 mg on Day 8 during the next cycle, then administer 30 mg on Day 15, followed by 30 mg on Day 1 of subsequent cycles. |
1 Indications and Usage
LUNSUMIO is a bispecific CD20-directed CD3 T-cell engager indicated for the treatment of adult patients with relapsed or refractory follicular lymphoma after two or more lines of systemic therapy.
This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). (1.1)
1.1 Follicular Lymphoma
LUNSUMIO is indicated for the treatment of adult patients with relapsed or refractory follicular lymphoma after two or more lines of systemic therapy.
This indication is approved under accelerated approval based on response rate [see Clinical Studies (14)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s).
12.1 Mechanism of Action
Mosunetuzumab-axgb is a T-cell engaging bispecific antibody that binds to the CD3 receptor expressed on the surface of T-cells and CD20 expressed on the surface of lymphoma cells and some healthy B-lineage cells.
In vitro, mosunetuzumab-axgb activated T-cells, caused the release of proinflammatory cytokines, and induced lysis of B-cells.
5.8 Embryo Fetal Toxicity
Based on its mechanism of action, LUNSUMIO may cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to the fetus. Advise females of reproductive potential to use effective contraception during treatment with LUNSUMIO and for 3 months after the last dose [see Use in Specific Populations (8.1, 8.3)].
5 Warnings and Precautions
- Neurologic Toxicity, including Immune Effector Cell-Associated Neurotoxicity Syndrome: Can cause serious and life-threatening neurologic toxicity, including immune effector cell-associated neurotoxicity syndrome (ICANS). Monitor patients for signs and symptoms of neurologic toxicity during treatment; withhold or permanently discontinue based on severity. (5.2)
- Infections: Can cause serious or fatal infections. Monitor patients for signs and symptoms of infection, including opportunistic infections, and treat as needed. (5.3)
- Hemophagocytic Lymphohistiocytosis: Can cause serious or fatal reactions. For suspected cases, interrupt LUNSUMIO and evaluate and treat promptly. (5.4)
- Cytopenias: Monitor complete blood cell counts during treatment. (5.5)
- Tumor Flare: Can cause serious tumor flare reactions. Monitor patients at risk for complications of tumor flare. (5.6)
- Risk of Medication Errors with Incorrect Product Use: Ensure that the correct formulation is being prescribed, dispensed, and administered. (5.7)
- Embryo-Fetal Toxicity: May cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception. (5.8, 8.1, 8.3)
2 Dosage and Administration
- LUNSUMIO and LUNSUMIO VELO have different dosage and administration instructions. Administer LUNSUMIO only as an intravenous infusion. (2.1)
- Premedicate to reduce risk of CRS and infusion-related reactions. (2.3, 5.1)
- Recommended dosage for LUNSUMIO for intravenous infusion (2.2):
| Day of Treatment Cycle length = 21 days
|
Intravenous Dose of LUNSUMIO | Rate of Infusion | |
|---|---|---|---|
| Cycle 1 | Day 1 | 1 mg | Administer over a minimum of 4 hours. |
| Day 8 | 2 mg | ||
| Day 15 | 60 mg | ||
| Cycle 2 | Day 1 | 60 mg | Administer over 2 hours if infusions from Cycle 1 were well-tolerated. |
| Cycles 3+ | Day 1 | 30 mg |
- See Full Prescribing Information for instructions on preparation and administration. (2.5)
3 Dosage Forms and Strengths
LUNSUMIO is a sterile, colorless solution for intravenous infusion available as:
- Injection: 1 mg/mL in a single-dose vial
- Injection: 30 mg/30 mL (1 mg/mL) in a single-dose vial
2.3 Recommended Premedication
Premedication to reduce the risk of CRS and infusion-related reactions are outlined in Table 3 [see Warnings and Precautions (5.1)].
| Treatment Cycle | Patients Requiring Premedication | Premedication | Dosage | Administration |
|---|---|---|---|---|
| Cycle 1 and Cycle 2 | All patients | Corticosteroid | Dexamethasone 20 mg (preferred) intravenous or methylprednisolone 80 mg intravenous | Complete at least 1 hour prior to infusion |
| Antihistamine | Diphenhydramine hydrochloride 50 mg to 100 mg or equivalent oral or intravenous antihistamine | At least 30 minutes prior to infusion | ||
| Antipyretic | Oral acetaminophen (500 mg to 1,000 mg) | At least 30 minutes prior to infusion | ||
| Cycles 3+ | Patients who experienced any grade CRS with the previous dose | Corticosteroid | Dexamethasone 20 mg (preferred) intravenous or methylprednisolone 80 mg intravenous | Complete at least 1 hour prior to infusion |
| Antihistamine | Diphenhydramine hydrochloride 50 mg to 100 mg or equivalent oral or intravenous antihistamine | At least 30 minutes prior to infusion | ||
| Antipyretic | Oral acetaminophen (500 mg to 1,000 mg) | At least 30 minutes prior to infusion |
5.1 Cytokine Release Syndrome
LUNSUMIO can cause CRS, including serious or life-threatening reactions [see Adverse Reactions (6.1)].
CRS occurred in 39% of patients who received LUNSUMIO at the recommended dosage in the clinical trial, with Grade 1 CRS occurring in 28%, Grade 2 in 15%, Grade 3 in 2%, and Grade 4 in 0.5% of patients. Among 86 patients who experienced CRS, CRS recurred in 28%. Most cases of CRS occurred following doses of 1 mg on Cycle 1 Day 1 (15%), 2 mg on Cycle 1 Day 8 (5%), and 60 mg on Cycle 1 Day 15 (33%). Five percent of patients experienced CRS after receiving 60 mg on Cycle 2 Day 1 with 1% of patients experiencing CRS following subsequent dosages of LUNSUMIO.
The median time to onset of CRS from the start of administration of LUNSUMIO in Cycle 1 Day 1 was 5 hours (range: 1 hour to 3 days), Cycle 1 Day 8 was 28 hours (range: 5 hours to 3 days), Cycle 1 Day 15 was 25 hours (range: 0.1 hours to 16 days), and Cycle 2 Day 1 was 46 hours (range: 12 hours to 3 days). The median duration of CRS was 3 days (range: 1 to 29 days).
Clinical signs and symptoms of CRS included, but were not limited to, fever, chills, hypotension, tachycardia, hypoxia, and headache. Concurrent neurologic adverse reactions occurred in 6% of patients and included but were not limited to headache, confusional state, and anxiety.
Initiate therapy according to LUNSUMIO step-up dosing schedule to reduce the risk of CRS [see Dosage and Administration (2.3)]. Administer pretreatment medications to reduce the risk of CRS, ensure adequate hydration, and monitor patients following administration of LUNSUMIO accordingly.
At the first sign of CRS, immediately evaluate patients for hospitalization, manage per current practice guidelines and administer supportive care; withhold or permanently discontinue LUNSUMIO based on severity [see Dosage and Administration (2.4)].
Patients who experience CRS (or other adverse reactions that impair consciousness) should be evaluated and advised not to drive and to refrain from operating heavy or potentially dangerous machinery until resolution.
8 Use in Specific Populations
Lactation: Advise not to breastfeed. (8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The pooled safety population described in the WARNINGS AND PRECAUTIONS reflects exposure to LUNSUMIO as a single agent in GO29781 in 218 patients with hematologic malignancies in an open-label, multicenter, multi-cohort study. Patients received step-up doses of 1 mg on Cycle 1 Day 1 and 2 mg on Cycle 1 Day 8, followed by 60 mg on Cycle 1 Day 15, and 60 mg on Cycle 2 Day 1, then 30 mg every 3 weeks in subsequent cycles. Each treatment cycle was 21 days. Among 218 patients who received LUNSUMIO, 52% were exposed for at least 8 cycles and 8% were exposed for 17 cycles.
In this pooled safety population, the most common (≥ 20%) adverse reactions were CRS (39%), fatigue (36%), rash (34%), pyrexia (24%), and headache (21%). The most common Grade 3 to 4 laboratory abnormalities (≥ 10%) were decreased lymphocyte count (92%), decreased phosphate (41%), increased glucose (40%), decreased neutrophil count (38%), decreased hemoglobin (19%), increased uric acid (15%), and decreased platelets (12%).
2.1 Important Dosing Information
-
LUNSUMIO and LUNSUMIO VELO have different dosage and administration instructions [see Dosage and Administration (2.2) and Warnings and Precautions (5.7)].
- LUNSUMIO is for intravenous use only.
- Check the product label to ensure that the correct formulation (LUNSUMIO or LUNSUMIO VELO) is being prescribed and administered.
- Do not substitute LUNSUMIO for or with LUNSUMIO VELO.
- Administer LUNSUMIO to well-hydrated patients.
- Premedicate before each dose in Cycle 1 and Cycle 2 [see Dosage and Administration (2.3)].
- Administer only as an intravenous infusion through a dedicated infusion line. Do not use an in-line filter to administer LUNSUMIO. Drip chamber filters can be used to administer LUNSUMIO.
- LUNSUMIO should only be administered by a qualified healthcare professional with appropriate medical support to manage severe reactions such as CRS and neurologic toxicity, including ICANS [see Warnings and Precautions (5.1 and 5.2)].
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
2.5 Preparation and Administration
To prevent medication errors, check the vial labels to ensure that the drug being prepared and administered is LUNSUMIO for intravenous infusion. A peel-off label is provided on the LUNSUMIO Prescribing Information that should be attached to the final prepared solution. Remove the peel-off label from the Prescribing Information in the LUNSUMIO carton before discarding the carton. Affix the peel-off label to the diluted LUNSUMIO infusion bag.
Warning: Cytokine Release Syndrome
Cytokine release syndrome (CRS), including serious or life-threatening reactions, can occur in patients receiving LUNSUMIO. Initiate treatment with the LUNSUMIO step-up dosing schedule to reduce the risk of CRS. Withhold LUNSUMIO until CRS resolves or permanently discontinue based on severity [see Dosage and Administration (2.1 and 2.4) and Warnings and Precautions (5.1)].
16 How Supplied/storage and Handling
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, colorless, preservative-free solution for intravenous infusion supplied as follows:
- One 1 mg/mL single-dose vial in a carton (NDC 50242-159-01)
- One 30 mg/30 mL (1 mg/mL) single-dose vial in a carton (NDC 50242-142-01).
5.4 Hemophagocytic Lymphohistiocytosis
LUNSUMIO can cause fatal or serious hemophagocytic lymphohistiocytosis (HLH). HLH is a potentially life-threatening, hyperinflammatory syndrome that is independent of CRS. Common manifestations include fever, elevated ferritin, hemophagocytosis, cytopenias, coagulopathy, hepatitis, and splenomegaly.
Across a broader clinical trial population, HLH occurred in 0.5% (7/1536) of patients. Most cases (5/7) were identified within the first 28 days following initiation of LUNSUMIO or LUNSUMIO VELO, with 3 cases preceded by diagnosed or suspected CRS. Of the 7 cases of HLH, 6 had fatal outcomes, with 2 deaths from HLH alone and 4 deaths with concurrent unresolved HLH. Of the 7 cases of HLH, 4 occurred in the context of concurrent EBV and/or CMV infection.
Monitor for clinical signs and symptoms of HLH. Consider HLH when the presentation of CRS is atypical or prolonged, or when there are features of macrophage activation. For suspected HLH, interrupt LUNSUMIO and evaluate and treat promptly for HLH per current practice guidelines.
Principal Display Panel 1 Mg/ml Vial Carton
NDC 50242-159-01
Lunsumio®
(mosunetuzumab-axgb)
Injection
1 mg/mL
For Intravenous Infusion Only.
Single-Dose Vial.
Discard Unused Portion.
ATTENTION: Dispense the enclosed
Medication Guide to each patient.
1 vial
Rx only
Genentech
11042421
2.4 Dosage Modifications for Adverse Reactions
8.3 Females and Males of Reproductive Potential
LUNSUMIO may cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Principal Display Panel 30 Mg/30 Ml Vial Carton
NDC 50242-142-01
Lunsumio®
(mosunetuzumab-axgb)
Injection
30 mg/30 mL
(1 mg/mL)
For Intravenous Infusion Only.
Single-Dose Vial.
Discard Unused Portion.
ATTENTION: Dispense the enclosed
Medication Guide to each patient.
1 vial
Rx only
Genentech
11042398
5.7 Risk of Medication Errors With Incorrect Product Use
Mosunetuzumab-axgb is available in two formulations: as an injection for intravenous use (LUNSUMIO) and as an injection for subcutaneous use (LUNSUMIO VELO). Check the product labels to ensure that the correct formulation is being prescribed, dispensed, and administered to the patient [see Dosage and Administration (2.2 and 2.5)]. Do not substitute LUNSUMIO for or with LUNSUMIO VELO.
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity or genotoxicity studies have been conducted with mosunetuzumab-axgb.
No dedicated studies have been conducted to evaluate the effects of mosunetuzumab-axgb on fertility. No adverse effects on either male or female reproductive organs were identified in a 26-week repeat dose chronic toxicity study in sexually mature cynomolgus monkeys.
5.2 Neurologic Toxicity, Including Immune Effector Cell Associated Neurotoxicity Syndrome
LUNSUMIO can cause serious and life-threatening neurologic toxicity, including immune effector cell-associated neurotoxicity syndrome (ICANS) [see Adverse Reactions (6.1)].
Neurologic toxicity occurred in 39% of patients who received LUNSUMIO at the recommended dosage in the clinical trial, with Grade 3 neurologic toxicity occurring in 3% of patients. The most frequent neurologic toxicities were headache (21%), peripheral neuropathy (13%), dizziness (11%) and mental status changes (6%, including confusional state, disturbance in attention, cognitive disorder, delirium, encephalopathy, and somnolence). ICANS was reported in 1% of patients (Grade 1: 0.5%, Grade 2: 0.5%) who received LUNSUMIO at the recommended dosage in the clinical trial.
Across a broader clinical trial population, ICANS or suspected ICANS occurred in 2.2% (21/949) of patients who received LUNSUMIO or LUNSUMIO VELO. The most frequent manifestations included confusional state and lethargy. Twenty patients had Grade 1-2 events and 1 patient had a Grade 3 event. The majority of cases (75%) occurred during the first cycle of treatment. The median time to onset was 17 days (range: 1 to 48 days). In total, 88% of cases resolved after a median duration of 3 days (range: 1 to 20 days).
Coadministration of LUNSUMIO with other products that cause dizziness or mental status changes may increase the risk of neurologic toxicity.
Monitor patients for signs and symptoms of neurologic toxicity during treatment. At the first sign of neurologic toxicity, including ICANS, immediately evaluate the patient, consider neurology evaluation as appropriate, and provide supportive therapy based on severity; withhold or permanently discontinue LUNSUMIO based on severity and follow management recommendations [see Dosage and Administration (2.4)].
Patients who experience neurologic toxicity such as tremors, dizziness, insomnia, severe neurotoxicity, or any other adverse reactions that impair consciousness should be evaluated, including potential neurology evaluation, and patients at increased risk should be advised not to drive and to refrain from operating heavy or potentially dangerous machinery until resolution.
Structured Label Content
Section 42229-5 (42229-5)
Dosage Modifications for Cytokine Release Syndrome
Identify CRS based on clinical presentation [see Warnings and Precautions (5.1)]. Evaluate for and treat other causes of fever, hypoxia, and hypotension.
If CRS is suspected, withhold LUNSUMIO until CRS resolves, manage according to the recommendations in Table 4 and per current practice guidelines. Administer supportive therapy for CRS, which may include intensive care for severe or life-threatening CRS.
| Grade Based on American Society for Transplantation and Cellular Therapy (ASTCT) 2019 grading for CRS.
|
Presenting Symptoms | Actions If CRS is refractory to management, consider other causes including hemophagocytic lymphohistiocytosis [see Warnings and Precautions (5.4)].
|
|---|---|---|
| Grade 1 | Fever ≥ 100.4°F (38°C) Premedication may mask fever, therefore if clinical presentation is consistent with CRS, follow these management guidelines.
|
|
| Grade 2 | Fever ≥ 100.4°F (38°C) with: Hypotension not requiring vasopressors and/or hypoxia requiring low-flow oxygen Low-flow oxygen defined as oxygen delivered at < 6 L/minute; high-flow oxygen defined as oxygen delivered at ≥ 6 L/minute. by nasal cannula or blow-by. |
|
Recurrent Grade 2 CRS
|
||
| Grade 3 | Fever ≥ 100.4°F (38°C) with: Hypotension requiring a vasopressor (with or without vasopressin) and/or hypoxia requiring high flow oxygen by nasal cannula, face mask, non-rebreather mask, or Venturi mask. |
|
Recurrent Grade 3 CRS
|
||
| Grade 4 | Fever ≥ 100.4°F (38°C) with: Hypotension requiring multiple vasopressors (excluding vasopressin) and/or hypoxia requiring oxygen by positive pressure (e.g., CPAP, BiPAP, intubation and mechanical ventilation). |
|
Section 42231-1 (42231-1)
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: Dec 2025 | |
|
MEDICATION GUIDE LUNSUMIO® (lun-SUM-mee-oh) (mosunetuzumab-axgb) injection, for intravenous infusion |
||
|
What is the most important information I should know about LUNSUMIO? Get medical help right away if you develop any signs or symptoms of CRS at any time, including: |
||
|
|
|
Due to the risk of CRS, you will receive LUNSUMIO on a "step-up dosing schedule".
|
||
| Your healthcare provider will check you for CRS during treatment with LUNSUMIO and may treat you in a hospital if you develop signs and symptoms of CRS. Your healthcare provider may temporarily stop or completely stop your treatment with LUNSUMIO if you have severe side effects. See "What are the possible side effects of LUNSUMIO?" for more information about side effects. |
||
|
What is LUNSUMIO?
LUNSUMIO is a prescription medicine used to treat adults with follicular lymphoma whose cancer has come back or did not respond to previous treatment, and who have already received two or more treatments for their cancer. It is not known if LUNSUMIO is safe and effective in children. |
||
Before receiving LUNSUMIO, tell your healthcare provider about all of your medical conditions, including if you:
|
||
|
How will I receive LUNSUMIO?
|
||
|
What should I avoid while receiving LUNSUMIO?
Do not drive, operate heavy machinery, or do other dangerous activities if you develop dizziness, confusion, tremors, sleepiness, or any other symptoms that impair consciousness until your signs and symptoms go away. These may be signs and symptoms of CRS or neurologic problems. See "What is the most important information I should know about LUNSUMIO?" and "What are the possible side effects of LUNSUMIO?" for more information about signs and symptoms of CRS and neurologic problems. |
||
|
What are the possible side effects of LUNSUMIO?
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
Your healthcare provider may temporarily stop or permanently stop treatment with LUNSUMIO if you develop severe side effects. The most common side effects of LUNSUMIO include: |
||
|
|
|
|
The most common severe abnormal blood test results with LUNSUMIO include: decreased blood cell counts, decreased phosphate, increased glucose, and increased uric acid levels. These are not all the possible side effects of LUNSUMIO. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
||
|
General information about the safe and effective use of LUNSUMIO.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. You can ask your pharmacist or healthcare provider for information about LUNSUMIO that is written for health professionals. |
||
|
What are the ingredients in LUNSUMIO? Active ingredient: mosunetuzumab-axgb Inactive ingredients: acetic acid, histidine, methionine, polysorbate 20, sucrose, and Water for Injection Manufactured by: Genentech, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 U.S. License No.: 1048 LUNSUMIO is a registered trademark of Genentech, Inc. For more information, call 1-844-832-3687 or go to www.LUNSUMIO.com. |
Section 43683-2 (43683-2)
Section 44425-7 (44425-7)
Store refrigerated at 2°C to 8°C (36°F to 46°F) in the original carton to protect from light.
Do not freeze. Do not shake.
11 Description (11 DESCRIPTION)
Mosunetuzumab-axgb is a bispecific CD20-directed CD3 T-cell engager. It is a humanized monoclonal anti-CD20xCD3 T-cell-dependent bispecific antibody of the immunoglobulin G1 (IgG1) isotype. Mosunetuzumab-axgb is produced in Chinese Hamster Ovary (CHO) cells by recombinant DNA technology. The approximate molecular weight is 146 kDa.
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, preservative-free, colorless solution for intravenous use.
Each single-dose vial contains a 1 mL solution of mosunetuzumab-axgb (1 mg), acetic acid (0.4 mg), histidine (1.6 mg), methionine (1.5 mg), polysorbate 20 (0.6 mg), sucrose (82.1 mg), and Water for Injection, USP. The pH is 5.8.
Each single-dose vial contains a 30 mL solution of mosunetuzumab-axgb (30 mg), acetic acid (12.8 mg), histidine (46.6 mg), methionine (44.8 mg), polysorbate 20 (18 mg), sucrose (2,462.4 mg), and Water for Injection, USP. The pH is 5.8.
5.3 Infections
LUNSUMIO can cause serious or fatal infections [see Adverse Reactions (6.1)].
Among patients who received LUNSUMIO at the recommended dosage in the clinical trial, serious infections, including opportunistic infections, occurred in 17%, with Grade 3 or 4 infections in 14% and fatal infections in 0.9% of patients. The most common Grade 3 or greater infections were pneumonia, sepsis, and upper respiratory infection.
Monitor patients for signs and symptoms of infection prior to and during treatment with LUNSUMIO and treat appropriately. LUNSUMIO should not be administered in the presence of active infection. Caution should be exercised when considering the use of LUNSUMIO in patients with a history of recurring or chronic infections (e.g., chronic, active Epstein-Barr Virus), with underlying conditions that may predispose to infections or who have had significant prior immunosuppressive treatment. Administer prophylactic antimicrobials according to guidelines.
Withhold LUNSUMIO or consider permanent discontinuation of LUNSUMIO based on severity [see Dosage and Administration (2.4)].
5.5 Cytopenias
LUNSUMIO can cause serious or severe cytopenias, including lymphopenia, neutropenia, anemia, and thrombocytopenia [see Adverse Reactions (6.1)].
Among patients who received LUNSUMIO at the recommended dosage in the clinical trial, Grade 3 or 4 decreased lymphocytes occurred in 92%, decreased neutrophils in 38%, decreased hemoglobin in 19%, and decreased platelets in 12% of patients. Grade 4 decreased lymphocytes occurred in 71%, decreased neutrophils in 19%, and decreased platelets in 5% of patients. Febrile neutropenia occurred in 2% of patients.
Monitor complete blood counts throughout treatment. Based on the severity of cytopenias, temporarily withhold, or permanently discontinue LUNSUMIO. Consider prophylactic granulocyte colony-stimulating factor administration as applicable [see Dosage and Administration (2.4)].
5.6 Tumor Flare
LUNSUMIO can cause serious or severe tumor flare [see Adverse Reactions (6.1)].
Among patients who received LUNSUMIO at the recommended dosage in the clinical trial, tumor flare occurred in 4%. Manifestations included new or worsening pleural effusions, localized pain and swelling at the sites of lymphoma lesions, and tumor inflammation.
Patients with bulky tumors or disease located in close proximity to airways or a vital organ should be monitored closely during initial therapy. Monitor for signs and symptoms of compression or obstruction due to mass effect secondary to tumor flare. If compression or obstruction develops, institute standard treatment of these complications.
8.4 Pediatric Use
The safety and efficacy of LUNSUMIO have not been established in pediatric patients.
8.5 Geriatric Use
Among the 90 patients with relapsed or refractory follicular lymphoma treated with LUNSUMIO, 33% were 65 years of age or older, and 8% were 75 years of age or older. There is an insufficient number of patients 65 years of age or older and 75 years of age or older to assess whether there are differences in safety or effectiveness in patients 65 years of age and older compared to younger adult patients.
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the study described below with the incidence of anti-drug antibodies in other studies, including those of mosunetuzumab-axgb.
During treatment in Study GO29781 (up to 12 months) [see Clinical Studies (14)], using an enzyme-linked immunosorbent assay (ELISA), no patients (N = 418) treated with LUNSUMIO developed anti-mosunetuzumab-axgb antibodies. Based on these data, the clinical relevance of anti-mosunetuzumab-axgb antibodies could not be assessed.
14 Clinical Studies (14 CLINICAL STUDIES)
The efficacy of LUNSUMIO was evaluated in an open-label, multicenter, multi-cohort study (GO29781, NCT02500407) in patients with relapsed or refractory follicular lymphoma (FL) who had received at least two prior therapies, including an anti-CD20 monoclonal antibody and an alkylating agent. The study excluded patients with active infections, history of autoimmune disease, prior allogeneic transplant, or any history of CNS lymphoma or CNS disorders.
Patients received step-up doses of 1 mg on Cycle 1 Day 1 and 2 mg on Cycle 1 Day 8, followed by 60 mg on Cycle 1 Day 15, and 60 mg on Cycle 2 Day 1, then 30 mg via intravenous infusion every 3 weeks in subsequent cycles. A treatment cycle was 21 days. LUNSUMIO was administered for 8 cycles unless patients experienced progressive disease or unacceptable toxicity. After 8 cycles, patients with a complete response discontinued therapy; patients with a partial response or stable disease continued treatment up to 17 cycles, unless patients experienced progressive disease or unacceptable toxicity.
Among the 90 patients with relapsed or refractory FL, the median age was 60 years (range: 29 to 90 years), 33% were 65 years of age or older, 61% were male, 82% were White, 9% were Asian, 4% were Black or African American, and 8% were Hispanic or Latino. A total of 77% of patients had Stage III-IV disease, 34% had bulky disease, and all patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. The median number of prior therapies was 3 (range: 2 to 10), with 38% receiving 2 prior therapies, 31% receiving 3 prior therapies, and 31% receiving more than 3 prior therapies.
Seventy-nine percent of patients were refractory to prior anti-CD20 monoclonal antibody therapy, 53% were refractory to both anti-CD20 monoclonal antibody and alkylator therapy, 9% received prior rituximab plus lenalidomide therapy, 21% received prior autologous stem cell transplant, and 3% received prior CAR-T therapy. Fifty-two percent of patients had progression of disease within 24 months of first systemic therapy.
Efficacy was established on the basis of objective response rate (ORR) and duration of response (DOR) as assessed by an independent review facility according to standard criteria for NHL (Cheson 2007). The median follow-up for DOR was 14.9 months. The efficacy results are summarized in Table 12.
| Response | LUNSUMIO N = 90 |
|---|---|
| CI = confidence interval; NR = not reached | |
| Objective response rate (ORR), n (%) | 72 (80) |
| (95% CI) | (70, 88) |
| Complete response (CR), n (%) | 54 (60) |
| (95% CI) | (49, 70) |
| Partial response (PR), n (%) | 18 (20) |
| (95% CI) | (12, 30) |
| Duration of response (DOR) | N = 72 |
| Median DOR DOR is defined as the time from the initial occurrence of a documented PR or CR until the patient experienced an event (documented disease progression or death due to any cause).
,
Kaplan-Meier estimate. , months (95% CI) |
22.8 (10, NR) |
| Rate of continued response | |
| At 12 months, % | 62 |
| (95% CI) | (50, 74) |
| At 18 months, % | 57 |
| (95% CI) | (44, 70) |
The median time to first response was 1.4 months (range: 1.1 to 8.9).
4 Contraindications (4 CONTRAINDICATIONS)
None.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following adverse reactions are described elsewhere in the labeling:
- Cytokine Release Syndrome [see Warnings and Precautions (5.1)]
- Neurologic Toxicity, including Immune Effector Cell-associated Neurotoxicity Syndrome [see Warnings and Precautions (5.2)]
- Infections [see Warnings and Precautions (5.3)]
- Hemophagocytic Lymphohistiocytosis [see Warnings and Precautions (5.4)]
- Cytopenias [see Warnings and Precautions (5.5)]
- Tumor Flare [see Warnings and Precautions (5.6)]
12.2 Pharmacodynamics
After intravenous administration of the recommended dosage of LUNSUMIO, peripheral B-cell counts decreased to undetectable levels (< 5 cells/microliter) in most patients (95%) by Cycle 2 Day 1 and the depletion was sustained at later cycles including at Cycle 4 and Cycle 8.
LUNSUMIO caused hypogammaglobulinemia (defined as IgG levels < 500 mg/dL). Among 67 patients with baseline IgG levels ≥ 500 mg/dL, 40% had their IgG level decreased to < 500 mg/dL after administration of the recommended dosage of LUNSUMIO.
Plasma concentrations of cytokines (IL-2, IL-6, IL-10, TNF-α, and IFN-γ) were measured, and transient elevation of cytokines were observed at doses of 0.4 mg and above. After administration of the recommended dosage of LUNSUMIO, the highest elevation of cytokines was observed within 24 hours after the first dose on Cycle 1 Day 1 and after the first 60 mg dose on Cycle 1 Day 15. The elevated cytokine levels generally returned to baseline prior to the next infusion on Cycle 1 Day 8 and on Cycle 2 Day 1.
12.3 Pharmacokinetics
Mosunetuzumab-axgb PK exposure increased proportionally over a dose range from 0.2 mg to 60 mg (0.007 to 2 times the recommended treatment dosage). PK exposures for the recommended dosage of LUNSUMIO are summarized in Table 10 and Figure 1.
| AUC (day∙μg/mL) Values are geometric mean with geometric CV%.
|
Cmax (μg/mL) | Ctrough (μg/mL) | |
|---|---|---|---|
| All values reported are model-predicted exposure metrics. | |||
| Cycle 1 (0 ‒ 21 days) | 35.2 (36.6) | 11.1 (36.7) | 2.6 (54.0) |
| Cycle 2 (21 ‒ 42 days) | 90.3 (48.5) | 13.6 (37.7) | 2.0 (83.1) |
| Cycle 3 (42 – 63 days) | 59.0 (48.9) | 7.6 (40.1) | 1.4 (75.6) |
| Steady state Steady state values are approximated at Cycle 4 (63 ‒ 84 days).
|
52.9 (40.7) | 7.0 (37.9) | 1.3 (59.9) |
Figure 1. Model-Predicted Mosunetuzumab-axgb Intravenous Infusion Concentration Time Profile
Pharmacokinetic parameters (Table 11) were evaluated at the recommended dosage and are presented as geometric mean (CV%) unless otherwise specified.
| Parameter | LUNSUMIO via Intravenous Infusion |
|---|---|
| Tmax = time to peak concentration | |
| Tmax median (range), hours Steady-state.
|
4.0 (4.0 – 4.0) Tmax is at the end of intravenous infusion.
|
| Volume of distributiona (L) | 5.5 (31%) |
| Half-lifea (days) | 16.1 (17%) |
| Systemic clearance (L/day) | 1.1 (63%) at baseline 0.58 (18%) at steady state |
2.2 Recommended Dosage
The recommended dosage for LUNSUMIO intravenous infusion is presented in Table 1.
Administer for 8 cycles, unless patients experience unacceptable toxicity or disease progression.
For patients who achieve a complete response, no further treatment beyond 8 cycles is required. For patients who achieve a partial response or have stable disease in response to treatment with LUNSUMIO after 8 cycles, an additional 9 cycles of treatment (17 cycles total) should be administered, unless a patient experiences unacceptable toxicity or disease progression.
| Day of Treatment | Intravenous Dose of LUNSUMIO | Rate of Infusion | |
|---|---|---|---|
| Cycle 1 | Day 1 | 1 mg | Administer over a minimum of 4 hours. |
| Day 8 | 2 mg | ||
| Day 15 | 60 mg | ||
| Cycle 2 | Day 1 | 60 mg | Administer over 2 hours if infusions from Cycle 1 were well-tolerated. |
| Cycles 3+ | Day 1 | 30 mg |
| Last Intravenous Dose Administered | Time Since Last Dose Administered | Action for Next Intravenous Dose(s) |
|---|---|---|
| 1 mg Cycle 1 Day 1 |
1week to 2 weeks | Administer 2 mg (Cycle 1 Day 8), then resume the planned treatment schedule. |
| Greater than 2 weeks | Repeat 1 mg (Cycle 1 Day 1), then administer 2 mg (Cycle 1 Day 8) and resume the planned treatment schedule. | |
| 2 mg Cycle 1 Day 8 |
1 week to 2 weeks | Administer 60 mg (Cycle 1 Day 15), then resume the planned treatment schedule. |
| Greater than 2 weeks to less than 6 weeks | Repeat 2 mg (Cycle 1 Day 8), then administer 60 mg (Cycle 1 Day 15) and resume the planned treatment schedule. | |
| Greater than or equal to 6 weeks | Repeat 1 mg (Cycle 1 Day 1) and 2 mg (Cycle 1 Day 8), then administer 60 mg (Cycle 1 Day 15) and resume the planned treatment schedule. | |
| 60 mg Cycle 1 Day 15 |
1 week to less than 6 weeks | Administer 60 mg (Cycle 2 Day 1), then resume the planned treatment schedule. |
| Greater than or equal to 6 weeks | Repeat 1 mg (Cycle 2 Day 1) and 2 mg (Cycle 2 Day 8), then administer 60 mg (Cycle 2 Day 15), followed by 30 mg (Cycle 3 Day 1) and then resume the planned treatment schedule. | |
| 60 mg Cycle 2 Day 1 |
3 weeks to less than 6 weeks | Administer 30 mg (Cycle 3 Day 1), then resume the planned treatment schedule. |
| Greater than or equal to 6 weeks | Repeat 1 mg (Cycle 3 Day 1) and 2 mg (Cycle 3 Day 8), then administer 30 mg (Cycle 3 Day 15) For the Day 1, Day 8, and Day 15 doses in the next cycle, administer premedication as per Table 3 for all patients. , followed by 30 mg (Cycle 4 Day 1) and then resume the planned treatment schedule. |
|
| 30 mg Cycle 3 onwards |
3 weeks to less than 6 weeks | Administer 30 mg, then resume the planned treatment schedule. |
| Greater than or equal to 6 weeks | Repeat 1 mg on Day 1 and 2 mg on Day 8 during the next cycle, then administer 30 mg on Day 15, followed by 30 mg on Day 1 of subsequent cycles. |
1 Indications and Usage (1 INDICATIONS AND USAGE)
LUNSUMIO is a bispecific CD20-directed CD3 T-cell engager indicated for the treatment of adult patients with relapsed or refractory follicular lymphoma after two or more lines of systemic therapy.
This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s). (1.1)
1.1 Follicular Lymphoma
LUNSUMIO is indicated for the treatment of adult patients with relapsed or refractory follicular lymphoma after two or more lines of systemic therapy.
This indication is approved under accelerated approval based on response rate [see Clinical Studies (14)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in a confirmatory trial(s).
12.1 Mechanism of Action
Mosunetuzumab-axgb is a T-cell engaging bispecific antibody that binds to the CD3 receptor expressed on the surface of T-cells and CD20 expressed on the surface of lymphoma cells and some healthy B-lineage cells.
In vitro, mosunetuzumab-axgb activated T-cells, caused the release of proinflammatory cytokines, and induced lysis of B-cells.
5.8 Embryo Fetal Toxicity (5.8 Embryo-Fetal Toxicity)
Based on its mechanism of action, LUNSUMIO may cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to the fetus. Advise females of reproductive potential to use effective contraception during treatment with LUNSUMIO and for 3 months after the last dose [see Use in Specific Populations (8.1, 8.3)].
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Neurologic Toxicity, including Immune Effector Cell-Associated Neurotoxicity Syndrome: Can cause serious and life-threatening neurologic toxicity, including immune effector cell-associated neurotoxicity syndrome (ICANS). Monitor patients for signs and symptoms of neurologic toxicity during treatment; withhold or permanently discontinue based on severity. (5.2)
- Infections: Can cause serious or fatal infections. Monitor patients for signs and symptoms of infection, including opportunistic infections, and treat as needed. (5.3)
- Hemophagocytic Lymphohistiocytosis: Can cause serious or fatal reactions. For suspected cases, interrupt LUNSUMIO and evaluate and treat promptly. (5.4)
- Cytopenias: Monitor complete blood cell counts during treatment. (5.5)
- Tumor Flare: Can cause serious tumor flare reactions. Monitor patients at risk for complications of tumor flare. (5.6)
- Risk of Medication Errors with Incorrect Product Use: Ensure that the correct formulation is being prescribed, dispensed, and administered. (5.7)
- Embryo-Fetal Toxicity: May cause fetal harm. Advise females of reproductive potential of the potential risk to the fetus and to use effective contraception. (5.8, 8.1, 8.3)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
- LUNSUMIO and LUNSUMIO VELO have different dosage and administration instructions. Administer LUNSUMIO only as an intravenous infusion. (2.1)
- Premedicate to reduce risk of CRS and infusion-related reactions. (2.3, 5.1)
- Recommended dosage for LUNSUMIO for intravenous infusion (2.2):
| Day of Treatment Cycle length = 21 days
|
Intravenous Dose of LUNSUMIO | Rate of Infusion | |
|---|---|---|---|
| Cycle 1 | Day 1 | 1 mg | Administer over a minimum of 4 hours. |
| Day 8 | 2 mg | ||
| Day 15 | 60 mg | ||
| Cycle 2 | Day 1 | 60 mg | Administer over 2 hours if infusions from Cycle 1 were well-tolerated. |
| Cycles 3+ | Day 1 | 30 mg |
- See Full Prescribing Information for instructions on preparation and administration. (2.5)
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
LUNSUMIO is a sterile, colorless solution for intravenous infusion available as:
- Injection: 1 mg/mL in a single-dose vial
- Injection: 30 mg/30 mL (1 mg/mL) in a single-dose vial
2.3 Recommended Premedication
Premedication to reduce the risk of CRS and infusion-related reactions are outlined in Table 3 [see Warnings and Precautions (5.1)].
| Treatment Cycle | Patients Requiring Premedication | Premedication | Dosage | Administration |
|---|---|---|---|---|
| Cycle 1 and Cycle 2 | All patients | Corticosteroid | Dexamethasone 20 mg (preferred) intravenous or methylprednisolone 80 mg intravenous | Complete at least 1 hour prior to infusion |
| Antihistamine | Diphenhydramine hydrochloride 50 mg to 100 mg or equivalent oral or intravenous antihistamine | At least 30 minutes prior to infusion | ||
| Antipyretic | Oral acetaminophen (500 mg to 1,000 mg) | At least 30 minutes prior to infusion | ||
| Cycles 3+ | Patients who experienced any grade CRS with the previous dose | Corticosteroid | Dexamethasone 20 mg (preferred) intravenous or methylprednisolone 80 mg intravenous | Complete at least 1 hour prior to infusion |
| Antihistamine | Diphenhydramine hydrochloride 50 mg to 100 mg or equivalent oral or intravenous antihistamine | At least 30 minutes prior to infusion | ||
| Antipyretic | Oral acetaminophen (500 mg to 1,000 mg) | At least 30 minutes prior to infusion |
5.1 Cytokine Release Syndrome
LUNSUMIO can cause CRS, including serious or life-threatening reactions [see Adverse Reactions (6.1)].
CRS occurred in 39% of patients who received LUNSUMIO at the recommended dosage in the clinical trial, with Grade 1 CRS occurring in 28%, Grade 2 in 15%, Grade 3 in 2%, and Grade 4 in 0.5% of patients. Among 86 patients who experienced CRS, CRS recurred in 28%. Most cases of CRS occurred following doses of 1 mg on Cycle 1 Day 1 (15%), 2 mg on Cycle 1 Day 8 (5%), and 60 mg on Cycle 1 Day 15 (33%). Five percent of patients experienced CRS after receiving 60 mg on Cycle 2 Day 1 with 1% of patients experiencing CRS following subsequent dosages of LUNSUMIO.
The median time to onset of CRS from the start of administration of LUNSUMIO in Cycle 1 Day 1 was 5 hours (range: 1 hour to 3 days), Cycle 1 Day 8 was 28 hours (range: 5 hours to 3 days), Cycle 1 Day 15 was 25 hours (range: 0.1 hours to 16 days), and Cycle 2 Day 1 was 46 hours (range: 12 hours to 3 days). The median duration of CRS was 3 days (range: 1 to 29 days).
Clinical signs and symptoms of CRS included, but were not limited to, fever, chills, hypotension, tachycardia, hypoxia, and headache. Concurrent neurologic adverse reactions occurred in 6% of patients and included but were not limited to headache, confusional state, and anxiety.
Initiate therapy according to LUNSUMIO step-up dosing schedule to reduce the risk of CRS [see Dosage and Administration (2.3)]. Administer pretreatment medications to reduce the risk of CRS, ensure adequate hydration, and monitor patients following administration of LUNSUMIO accordingly.
At the first sign of CRS, immediately evaluate patients for hospitalization, manage per current practice guidelines and administer supportive care; withhold or permanently discontinue LUNSUMIO based on severity [see Dosage and Administration (2.4)].
Patients who experience CRS (or other adverse reactions that impair consciousness) should be evaluated and advised not to drive and to refrain from operating heavy or potentially dangerous machinery until resolution.
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
Lactation: Advise not to breastfeed. (8.2)
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The pooled safety population described in the WARNINGS AND PRECAUTIONS reflects exposure to LUNSUMIO as a single agent in GO29781 in 218 patients with hematologic malignancies in an open-label, multicenter, multi-cohort study. Patients received step-up doses of 1 mg on Cycle 1 Day 1 and 2 mg on Cycle 1 Day 8, followed by 60 mg on Cycle 1 Day 15, and 60 mg on Cycle 2 Day 1, then 30 mg every 3 weeks in subsequent cycles. Each treatment cycle was 21 days. Among 218 patients who received LUNSUMIO, 52% were exposed for at least 8 cycles and 8% were exposed for 17 cycles.
In this pooled safety population, the most common (≥ 20%) adverse reactions were CRS (39%), fatigue (36%), rash (34%), pyrexia (24%), and headache (21%). The most common Grade 3 to 4 laboratory abnormalities (≥ 10%) were decreased lymphocyte count (92%), decreased phosphate (41%), increased glucose (40%), decreased neutrophil count (38%), decreased hemoglobin (19%), increased uric acid (15%), and decreased platelets (12%).
2.1 Important Dosing Information
-
LUNSUMIO and LUNSUMIO VELO have different dosage and administration instructions [see Dosage and Administration (2.2) and Warnings and Precautions (5.7)].
- LUNSUMIO is for intravenous use only.
- Check the product label to ensure that the correct formulation (LUNSUMIO or LUNSUMIO VELO) is being prescribed and administered.
- Do not substitute LUNSUMIO for or with LUNSUMIO VELO.
- Administer LUNSUMIO to well-hydrated patients.
- Premedicate before each dose in Cycle 1 and Cycle 2 [see Dosage and Administration (2.3)].
- Administer only as an intravenous infusion through a dedicated infusion line. Do not use an in-line filter to administer LUNSUMIO. Drip chamber filters can be used to administer LUNSUMIO.
- LUNSUMIO should only be administered by a qualified healthcare professional with appropriate medical support to manage severe reactions such as CRS and neurologic toxicity, including ICANS [see Warnings and Precautions (5.1 and 5.2)].
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
2.5 Preparation and Administration
To prevent medication errors, check the vial labels to ensure that the drug being prepared and administered is LUNSUMIO for intravenous infusion. A peel-off label is provided on the LUNSUMIO Prescribing Information that should be attached to the final prepared solution. Remove the peel-off label from the Prescribing Information in the LUNSUMIO carton before discarding the carton. Affix the peel-off label to the diluted LUNSUMIO infusion bag.
Warning: Cytokine Release Syndrome (WARNING: CYTOKINE RELEASE SYNDROME)
Cytokine release syndrome (CRS), including serious or life-threatening reactions, can occur in patients receiving LUNSUMIO. Initiate treatment with the LUNSUMIO step-up dosing schedule to reduce the risk of CRS. Withhold LUNSUMIO until CRS resolves or permanently discontinue based on severity [see Dosage and Administration (2.1 and 2.4) and Warnings and Precautions (5.1)].
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
LUNSUMIO (mosunetuzumab-axgb) injection is a sterile, colorless, preservative-free solution for intravenous infusion supplied as follows:
- One 1 mg/mL single-dose vial in a carton (NDC 50242-159-01)
- One 30 mg/30 mL (1 mg/mL) single-dose vial in a carton (NDC 50242-142-01).
5.4 Hemophagocytic Lymphohistiocytosis
LUNSUMIO can cause fatal or serious hemophagocytic lymphohistiocytosis (HLH). HLH is a potentially life-threatening, hyperinflammatory syndrome that is independent of CRS. Common manifestations include fever, elevated ferritin, hemophagocytosis, cytopenias, coagulopathy, hepatitis, and splenomegaly.
Across a broader clinical trial population, HLH occurred in 0.5% (7/1536) of patients. Most cases (5/7) were identified within the first 28 days following initiation of LUNSUMIO or LUNSUMIO VELO, with 3 cases preceded by diagnosed or suspected CRS. Of the 7 cases of HLH, 6 had fatal outcomes, with 2 deaths from HLH alone and 4 deaths with concurrent unresolved HLH. Of the 7 cases of HLH, 4 occurred in the context of concurrent EBV and/or CMV infection.
Monitor for clinical signs and symptoms of HLH. Consider HLH when the presentation of CRS is atypical or prolonged, or when there are features of macrophage activation. For suspected HLH, interrupt LUNSUMIO and evaluate and treat promptly for HLH per current practice guidelines.
Principal Display Panel 1 Mg/ml Vial Carton (PRINCIPAL DISPLAY PANEL - 1 mg/mL Vial Carton)
NDC 50242-159-01
Lunsumio®
(mosunetuzumab-axgb)
Injection
1 mg/mL
For Intravenous Infusion Only.
Single-Dose Vial.
Discard Unused Portion.
ATTENTION: Dispense the enclosed
Medication Guide to each patient.
1 vial
Rx only
Genentech
11042421
2.4 Dosage Modifications for Adverse Reactions
8.3 Females and Males of Reproductive Potential
LUNSUMIO may cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Principal Display Panel 30 Mg/30 Ml Vial Carton (PRINCIPAL DISPLAY PANEL - 30 mg/30 mL Vial Carton)
NDC 50242-142-01
Lunsumio®
(mosunetuzumab-axgb)
Injection
30 mg/30 mL
(1 mg/mL)
For Intravenous Infusion Only.
Single-Dose Vial.
Discard Unused Portion.
ATTENTION: Dispense the enclosed
Medication Guide to each patient.
1 vial
Rx only
Genentech
11042398
5.7 Risk of Medication Errors With Incorrect Product Use (5.7 Risk of Medication Errors with Incorrect Product Use)
Mosunetuzumab-axgb is available in two formulations: as an injection for intravenous use (LUNSUMIO) and as an injection for subcutaneous use (LUNSUMIO VELO). Check the product labels to ensure that the correct formulation is being prescribed, dispensed, and administered to the patient [see Dosage and Administration (2.2 and 2.5)]. Do not substitute LUNSUMIO for or with LUNSUMIO VELO.
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity or genotoxicity studies have been conducted with mosunetuzumab-axgb.
No dedicated studies have been conducted to evaluate the effects of mosunetuzumab-axgb on fertility. No adverse effects on either male or female reproductive organs were identified in a 26-week repeat dose chronic toxicity study in sexually mature cynomolgus monkeys.
5.2 Neurologic Toxicity, Including Immune Effector Cell Associated Neurotoxicity Syndrome (5.2 Neurologic Toxicity, including Immune Effector Cell-Associated Neurotoxicity Syndrome)
LUNSUMIO can cause serious and life-threatening neurologic toxicity, including immune effector cell-associated neurotoxicity syndrome (ICANS) [see Adverse Reactions (6.1)].
Neurologic toxicity occurred in 39% of patients who received LUNSUMIO at the recommended dosage in the clinical trial, with Grade 3 neurologic toxicity occurring in 3% of patients. The most frequent neurologic toxicities were headache (21%), peripheral neuropathy (13%), dizziness (11%) and mental status changes (6%, including confusional state, disturbance in attention, cognitive disorder, delirium, encephalopathy, and somnolence). ICANS was reported in 1% of patients (Grade 1: 0.5%, Grade 2: 0.5%) who received LUNSUMIO at the recommended dosage in the clinical trial.
Across a broader clinical trial population, ICANS or suspected ICANS occurred in 2.2% (21/949) of patients who received LUNSUMIO or LUNSUMIO VELO. The most frequent manifestations included confusional state and lethargy. Twenty patients had Grade 1-2 events and 1 patient had a Grade 3 event. The majority of cases (75%) occurred during the first cycle of treatment. The median time to onset was 17 days (range: 1 to 48 days). In total, 88% of cases resolved after a median duration of 3 days (range: 1 to 20 days).
Coadministration of LUNSUMIO with other products that cause dizziness or mental status changes may increase the risk of neurologic toxicity.
Monitor patients for signs and symptoms of neurologic toxicity during treatment. At the first sign of neurologic toxicity, including ICANS, immediately evaluate the patient, consider neurology evaluation as appropriate, and provide supportive therapy based on severity; withhold or permanently discontinue LUNSUMIO based on severity and follow management recommendations [see Dosage and Administration (2.4)].
Patients who experience neurologic toxicity such as tremors, dizziness, insomnia, severe neurotoxicity, or any other adverse reactions that impair consciousness should be evaluated, including potential neurology evaluation, and patients at increased risk should be advised not to drive and to refrain from operating heavy or potentially dangerous machinery until resolution.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:51:34.234335 · Updated: 2026-03-14T22:40:50.579212