Calcitonin Salmon Injection
2b8c6917-c217-45bf-a0ac-a2fa0f7d497a
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
Calcitonin Salmon synthetic injection is a calcitonin, indicated for the following conditions: Treatment of symptomatic Paget's disease of bone when alternative treatments are not suitable ( 1.1 ) Treatment of hypercalcemia ( 1.2 ) Treatment of postmenopausal osteoporosis when alternative treatments are not suitable. Fracture reduction efficacy has not been demonstrated ( 1.3 ) Limitations of Use: Due to the possible association between malignancy and calcitonin-salmon use, the need for continued therapy should be re-evaluated on a periodic basis ( 1.4 , 5.3 )
Dosage and Administration
Symptomatic Paget's disease of bone: 100 International Units daily. Ensure adequate calcium and vitamin D intake ( 2.1 , 2.5 ) Hypercalcemia: start with 4 International Units/kg body weight every 12 hours. Increase to 8 International Units/kg every 12 hours if no improvement in 1-2 days. Increase further to 8 International Units/kg every 6 hours if no improvement after 2 more days ( 2.2 ) Postmenopausal osteoporosis: 100 International Units daily. Ensure adequate calcium and vitamin D intake ( 2.3 , 2.5 )
Contraindications
Hypersensitivity to calcitonin-salmon or any of the excipients. Reactions have included anaphylaxis with death, bronchospasm, and swelling of the tongue or throat [see Warnings and Precautions ( 5.1 )] .
Warnings and Precautions
Serious hypersensitivity reactions, including reports of fatal anaphylaxis have been reported. Consider skin testing prior to treatment in patients with suspected hypersensitivity to calcitonin-salmon ( 5.1 ) Hypocalcemia has been reported. Ensure adequate intake of calcium and vitamin D ( 5.2 ) Malignancy: A meta-analysis of 21 clinical trials suggests an increased risk of overall malignancies in calcitonin-salmon- treated patients ( 5.3 , 6.1 ) Circulating antibodies to calcitonin-salmon may develop, and may cause loss of response to treatment ( 5.4 )
Adverse Reactions
The following serious adverse reactions are discussed in greater detail in other sections of the label: Hypersensitivity Reactions, including anaphylaxis [see Warnings and Precautions ( 5.1 )] Hypocalcemia [see Warnings and Precautions ( 5.2 )] Malignancy [see Warnings and Precautions ( 5.3 )]
Drug Interactions
No formal drug interaction studies have been performed with Calcitonin Salmon injection. Concomitant use of calcitonin-salmon and lithium may lead to a reduction in plasma lithium concentrations due to increased urinary clearance of lithium. The dose of lithium may require adjustment.
Description
Calcitonin Salmon synthetic injection is a calcitonin, indicated for the following conditions: Treatment of symptomatic Paget's disease of bone when alternative treatments are not suitable ( 1.1 ) Treatment of hypercalcemia ( 1.2 ) Treatment of postmenopausal osteoporosis when alternative treatments are not suitable. Fracture reduction efficacy has not been demonstrated ( 1.3 ) Limitations of Use: Due to the possible association between malignancy and calcitonin-salmon use, the need for continued therapy should be re-evaluated on a periodic basis ( 1.4 , 5.3 )
Medication Information
Warnings and Precautions
Serious hypersensitivity reactions, including reports of fatal anaphylaxis have been reported. Consider skin testing prior to treatment in patients with suspected hypersensitivity to calcitonin-salmon ( 5.1 ) Hypocalcemia has been reported. Ensure adequate intake of calcium and vitamin D ( 5.2 ) Malignancy: A meta-analysis of 21 clinical trials suggests an increased risk of overall malignancies in calcitonin-salmon- treated patients ( 5.3 , 6.1 ) Circulating antibodies to calcitonin-salmon may develop, and may cause loss of response to treatment ( 5.4 )
Indications and Usage
Calcitonin Salmon synthetic injection is a calcitonin, indicated for the following conditions: Treatment of symptomatic Paget's disease of bone when alternative treatments are not suitable ( 1.1 ) Treatment of hypercalcemia ( 1.2 ) Treatment of postmenopausal osteoporosis when alternative treatments are not suitable. Fracture reduction efficacy has not been demonstrated ( 1.3 ) Limitations of Use: Due to the possible association between malignancy and calcitonin-salmon use, the need for continued therapy should be re-evaluated on a periodic basis ( 1.4 , 5.3 )
Dosage and Administration
Symptomatic Paget's disease of bone: 100 International Units daily. Ensure adequate calcium and vitamin D intake ( 2.1 , 2.5 ) Hypercalcemia: start with 4 International Units/kg body weight every 12 hours. Increase to 8 International Units/kg every 12 hours if no improvement in 1-2 days. Increase further to 8 International Units/kg every 6 hours if no improvement after 2 more days ( 2.2 ) Postmenopausal osteoporosis: 100 International Units daily. Ensure adequate calcium and vitamin D intake ( 2.3 , 2.5 )
Contraindications
Hypersensitivity to calcitonin-salmon or any of the excipients. Reactions have included anaphylaxis with death, bronchospasm, and swelling of the tongue or throat [see Warnings and Precautions ( 5.1 )] .
Adverse Reactions
The following serious adverse reactions are discussed in greater detail in other sections of the label: Hypersensitivity Reactions, including anaphylaxis [see Warnings and Precautions ( 5.1 )] Hypocalcemia [see Warnings and Precautions ( 5.2 )] Malignancy [see Warnings and Precautions ( 5.3 )]
Drug Interactions
No formal drug interaction studies have been performed with Calcitonin Salmon injection. Concomitant use of calcitonin-salmon and lithium may lead to a reduction in plasma lithium concentrations due to increased urinary clearance of lithium. The dose of lithium may require adjustment.
Description
Calcitonin Salmon synthetic injection is a calcitonin, indicated for the following conditions: Treatment of symptomatic Paget's disease of bone when alternative treatments are not suitable ( 1.1 ) Treatment of hypercalcemia ( 1.2 ) Treatment of postmenopausal osteoporosis when alternative treatments are not suitable. Fracture reduction efficacy has not been demonstrated ( 1.3 ) Limitations of Use: Due to the possible association between malignancy and calcitonin-salmon use, the need for continued therapy should be re-evaluated on a periodic basis ( 1.4 , 5.3 )
Section 42229-5
Nausea: Nausea with or without vomiting has been noted in about 10% of patients treated with calcitonin-salmon. It is most evident when treatment is first initiated and tends to decrease or disappear with continued administration.
Section 44425-7
Storage and Handling
Store in refrigerator between 2° to 8°C (36° to 46°F). Avoid freezing.
The container closure is not made with natural rubber latex.
Section 51945-4
PACKAGE LABEL - PRINCIPAL DISPLAY – Calcitonin Salmon 2 mL Carton Panel
NDC 63323-865-02 865102
Calcitonin Salmon
Injection, USP Synthetic
400 I.U. per 2 mL
(200 I.U. per mL)
For Intramuscular or Subcutaneous Injection
Rx only 2 mL Multi-Dose Vial
10 Overdosage
The pharmacologic actions of Calcitonin Salmon injection suggest that hypocalcemic tetany could occur in overdose. Therefore, provisions for parenteral administration of calcium should be available for the treatment of overdose.
A dose of calcitonin-salmon l000 International Units subcutaneously may produce nausea and vomiting. Doses of 32 International Units per kg per day for 1 to 2 days demonstrate no other adverse effects. Data on chronic high-dose administration are insufficient to assess toxicity.
11 Description
Calcitonin is a polypeptide hormone secreted by the parafollicular cells of the thyroid gland in mammals and by the ultimobranchial gland of birds and fish.
Calcitonin Salmon Injection, USP Synthetic is a synthetic polypeptide of 32 amino acids in the same linear sequence that is found in calcitonin of salmon origin. This is shown by the following graphic formula:
It is provided in sterile solution for subcutaneous or intramuscular injection. Each milliliter contains: calcitonin-salmon 200 International Units.
Inactive Ingredients (per mL): acetic acid, USP, 2.25 mg; phenol, USP, 5.0 mg; sodium acetate trihydrate, USP, 2.0 mg; sodium chloride, USP, 7.5 mg; water for injection, USP.
The activity of Calcitonin Salmon injection is stated in International Units based on bioassay in comparison with the International Reference Preparation of calcitonin-salmon for Bioassay, distributed by the National Institute for Biological Standards and Control, Holly Hill, London.
5.3 Malignancy
In a meta-analysis of 21 randomized, controlled clinical trials with calcitonin-salmon (nasal spray or investigational oral formulations), the overall incidence of malignancies reported was higher among calcitonin-salmon-treated patients (4.1%) compared with placebo-treated patients (2.9%). This suggests an increased risk of malignancies in calcitonin-salmon-treated patients compared to placebo-treated patients. It is not possible to exclude an increased risk when calcitonin-salmon is administered long-term subcutaneously, intramuscularly, or intravenously. The benefits for the individual patient should be carefully considered against possible risks [see Adverse Reactions (6.1)].
5.2 Hypocalcemia
Hypocalcemia associated with tetany (i.e., muscle cramps, twitching) and seizure activity has been reported with Calcitonin Salmon injection therapy. Hypocalcemia must be corrected before initiating therapy. Other disorders affecting mineral metabolism (such as vitamin D deficiency) should also be effectively treated. In patients at risk for hypocalcemia, provisions for parenteral calcium administration should be available during the first several administrations of calcitonin salmon and serum calcium and symptoms of hypocalcemia should be monitored. Use of Calcitonin Salmon injection for the treatment of Paget's disease or postmenopausal osteoporosis is recommended in conjunction with an adequate intake of calcium and vitamin D [see Dosage and Administration (2.5)].
2.2 Hypercalcemia
The recommended starting dose of Calcitonin Salmon injection for early treatment of hypercalcemia is 4 International Units/kg body weight every 12 hours by subcutaneous or intramuscular injection. If the response to this dose is not satisfactory after one or two days, the dose may be increased to 8 International Units/kg every 12 hours. If the response remains unsatisfactory after two more days, the dose may be further increased to a maximum of 8 International Units/kg every 6 hours.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
Clinical studies of Calcitonin Salmon injection did not include sufficient numbers of subjects aged 65 years and older to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
14.2 Hypercalcemia
In four open-label clinical trials enrolling 53 patients, calcitonin-salmon has been shown to lower elevated serum calcium levels of patients with carcinoma (with or without metastases), multiple myeloma, and primary hyperparathyroidism (lesser response). These patients were treated with calcitonin-salmon only when other methods of lowering serum calcium (hydration, oral phosphate, corticosteroids) were unsuccessful or unsuitable. With patients' pre-therapy serum calcium levels as controls, reduction in serum calcium was evident within 1 to 2 hours of administration. The peak effect occurred within 24 to 48 hours of injection and administration of calcitonin-salmon every 12 hours maintained a hypocalcemic effect for approximately 5 to 8 days, the time period evaluated for most patients in the clinical trials. The average reduction of 8 hour post-injection serum calcium was approximately 9% (2 to 3 mg/dL). Patients with higher values of serum calcium tended to show greater reductions during calcitonin-salmon treatment.
6.3 Immunogenicity
Consistent with the potentially immunogenic properties of medicinal products containing peptides, administration of Calcitonin Salmon may trigger the development of anti-calcitonin antibodies. Circulating antibodies to calcitonin-salmon after 2 to 18 months of treatment have been reported in about one-half of the patients with Paget's disease in whom antibody studies were done. In some cases, high antibody titers are found; these patients usually will have a loss of response to treatment [see Warnings and Precautions (5.4)].
The incidence of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of a positive antibody test result may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of antibodies among different calcitonin-salmon products may be misleading.
4 Contraindications
Hypersensitivity to calcitonin-salmon or any of the excipients. Reactions have included anaphylaxis with death, bronchospasm, and swelling of the tongue or throat [see Warnings and Precautions (5.1)].
6 Adverse Reactions
7 Drug Interactions
No formal drug interaction studies have been performed with Calcitonin Salmon injection.
Concomitant use of calcitonin-salmon and lithium may lead to a reduction in plasma lithium concentrations due to increased urinary clearance of lithium. The dose of lithium may require adjustment.
12.3 Pharmacokinetics
The absolute bioavailability of calcitonin-salmon is approximately 66% and 71% after intramuscular or subcutaneous injection, respectively. After subcutaneous administration, peak plasma levels are reached in approximately 23 minutes. The terminal half-life is approximately 58 minutes for intramuscular administration and 59 to 64 minutes for subcutaneous administration. The apparent volume of distribution is 0.15 to 0.3 L/kg.
5.4 Antibody Formation
Circulating antibodies to calcitonin-salmon have been reported with Calcitonin Salmon injection. The possibility of antibody formation should be considered in any patient with an initial response to Calcitonin Salmon injection who later stops responding to treatment [see Adverse Reactions (6.3)].
1 Indications and Usage
Calcitonin Salmon synthetic injection is a calcitonin, indicated for the following conditions:
- Treatment of symptomatic Paget's disease of bone when alternative treatments are not suitable (1.1)
- Treatment of hypercalcemia (1.2)
- Treatment of postmenopausal osteoporosis when alternative treatments are not suitable. Fracture reduction efficacy has not been demonstrated (1.3)
Limitations of Use:
12.1 Mechanism of Action
Calcitonin-salmon is a calcitonin receptor agonist. Calcitonin-salmon acts primarily on bone, but direct renal effects and actions on the gastrointestinal tract are also recognized. Calcitonin salmon appears to have actions essentially identical to calcitonins of mammalian origin, but its potency per mg is greater and it has a longer duration of action.
The actions of calcitonin on bone and its role in normal human bone physiology are still not completely elucidated, although calcitonin receptors have been discovered in osteoclasts and osteoblasts.
5 Warnings and Precautions
- Serious hypersensitivity reactions, including reports of fatal anaphylaxis have been reported. Consider skin testing prior to treatment in patients with suspected hypersensitivity to calcitonin-salmon (5.1)
- Hypocalcemia has been reported. Ensure adequate intake of calcium and vitamin D (5.2)
- Malignancy: A meta-analysis of 21 clinical trials suggests an increased risk of overall malignancies in calcitonin-salmon- treated patients (5.3, 6.1)
- Circulating antibodies to calcitonin-salmon may develop, and may cause loss of response to treatment (5.4)
2 Dosage and Administration
- Symptomatic Paget's disease of bone: 100 International Units daily. Ensure adequate calcium and vitamin D intake (2.1, 2.5)
- Hypercalcemia: start with 4 International Units/kg body weight every 12 hours. Increase to 8 International Units/kg every 12 hours if no improvement in 1-2 days. Increase further to 8 International Units/kg every 6 hours if no improvement after 2 more days (2.2)
- Postmenopausal osteoporosis: 100 International Units daily. Ensure adequate calcium and vitamin D intake (2.3, 2.5)
2.1 Paget's Disease of Bone
The recommended dose of Calcitonin Salmon injection for treatment of symptomatic Paget's disease of bone is 100 International Units (0.5 mL) per day administered subcutaneously or intramuscularly.
14.1 Paget's Disease of Bone
The trials used for the basis of approval for calcitonin-salmon injection for treatment of Paget's disease of bone were conducted in patients with moderate to severe disease characterized by polyostotic involvement with elevated serum alkaline phosphatase and urinary hydroxyproline excretion. In open-label clinical trials of several months to two years duration with historical controls, biochemical abnormalities were substantially improved (more than 30% reduction) in about 2/3 of patients studied and bone pain was improved in a similar fraction. A small number of documented instances of reversal of neurologic deficits have occurred, including improvement in the basilar compression syndrome, and improvement of spinal cord and spinal nerve lesions.
There is too little experience to predict the likelihood of improvement of any given neurologic lesion. Hearing loss is improved infrequently (4 of 29 patients studied by audiometry). Patients with increased cardiac output due to extensive Paget's disease of bone have had measured decreases in cardiac output while receiving calcitonin-salmon. The number of treated patients in this category is too small to predict how likely such a result will be.
There is no evidence that the prophylactic use of calcitonin-salmon is beneficial in asymptomatic patients.
3 Dosage Forms and Strengths
Calcitonin Salmon Injection, USP is available as a clear, colorless, sterile solution of synthetic calcitonin salmon in individual 2 mL multi-dose vials containing 200 International Units per mL.
6.2 Postmarketing Experience
Because postmarketing adverse reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The following adverse reactions have been reported during post-approval use of Calcitonin Salmon injection.
Allergic / Hypersensitivity Reactions: Serious hypersensitivity reactions have been reported in patients receiving calcitonin-salmon injection, e.g., bronchospasm, swelling of the tongue or throat, anaphylactic shock, and death due to anaphylaxis.
Skin and subcutaneous tissue disorders: Urticaria
Hypocalcemia: Hypocalcemia with tetany (i.e. muscle cramps, twitching) and seizure activity have been reported.
Body as a Whole: influenza-like symptoms, fatigue, edema (facial, peripheral, and generalized)
Musculoskeletal: arthralgia, musculoskeletal pain
Cardiovascular: hypertension
Gastrointestinal: abdominal pain, diarrhea
Urinary System: polyuria
Nervous System: dizziness, headache, paresthesia, tremor
Vision: visual disturbance
8 Use in Specific Populations
There are no data to support use in children (8.4)
1.2 Treatment of Hypercalcemia
Calcitonin Salmon injection is indicated for the early treatment of hypercalcemic emergencies, along with other appropriate agents, when a rapid decrease in serum calcium is required, until more specific treatment of the underlying disease can be accomplished. It may also be added to existing therapeutic regimens for hypercalcemia such as intravenous fluids and furosemide, oral phosphate or corticosteroids, or other agents.
5.1 Hypersensitivity Reactions
Serious hypersensitivity reactions have been reported in patients receiving Calcitonin Salmon injection, e.g., bronchospasm, swelling of the tongue or throat, anaphylactic shock, and death due to anaphylaxis. Appropriate medical support and monitoring measures should be readily available when Calcitonin Salmon injection is administered. If anaphylaxis or other severe hypersensitivity/allergic reactions occur, initiate appropriate treatment [see Contraindications (4)].
For patients with suspected hypersensitivity to calcitonin-salmon, skin testing should be considered prior to treatment utilizing a dilute, sterile solution of Calcitonin Salmon injection. Healthcare providers may wish to refer patients who require skin testing to an allergist.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of calcitonin-salmon injection was assessed in open-label trials several months to two years in duration. The most common adverse reactions are discussed below.
2.3 Postmenopausal Osteoporosis
The recommended dose of Calcitonin Salmon injection for treatment of postmenopausal osteoporosis in women greater than 5 years postmenopause is 100 International Units (0.5 mL) per day administered subcutaneously or intramuscularly. The minimum effective dose of Calcitonin Salmon injection for the prevention of vertebral bone mineral density loss has not been established.
1.4 Important Limitations of Use
Due to the possible association between malignancy and calcitonin-salmon use, the need for continued therapy should be re-evaluated on a periodic basis [see Warnings and Precautions (5.3)].
14.3 Postmenopausal Osteoporosis
The trials used for the basis of approval for calcitonin-salmon injection for treatment of postmenopausal osteoporosis were two randomized, open-label, 2-year studies in postmenopausal women 50 to 74 years of age with total body calcium < 85% of expected normal, and vertebral osteopenia (by x-ray criteria) and/or at least one atraumatic compression fracture. The primary efficacy endpoint was total body calcium measured by neutron activation analysis. Patients were randomized to calcitonin-salmon injection 100 International Units daily (subcutaneously or intramuscularly) at bedtime, or control. All subjects received daily supplements of 1200 mg calcium carbonate and 400 International Units of vitamin D.
In both studies, total body calcium increased from baseline with calcitonin-salmon therapy at 1 year, followed by a trend to decreasing total body calcium (still above baseline) at 2 years.
Thoracic and lumbar spine X-rays (AP/lateral) were obtained yearly. For the two studies combined (34 calcitonin-salmon and 35 control subjects), in the first year there was a total of 6 new vertebral compression fractures in the calcitonin-salmon group and 5 in the control group. In the second year there were 7 new fractures in each group.
No evidence currently exists to indicate whether Calcitonin Salmon injection decreases the risk of osteoporotic fracture. A controlled study, which was prematurely discontinued, failed to demonstrate any benefit of calcitonin-salmon on fracture rate.
No adequate controlled trials have examined the effect of calcitonin-salmon injection on vertebral bone mineral density beyond 1 year of treatment. Therefore, the minimum effective dose of Calcitonin Salmon injection for prevention of vertebral bone mineral density loss has not been established.
In clinical studies of postmenopausal osteoporosis, bone biopsy and radial bone mass assessments at baseline and after 26 months of daily injectable calcitonin-salmon indicate that calcitonin therapy results in the formation of normal bone.
5.5 Urine Sediment Abnormalities
Coarse granular casts and casts containing renal tubular epithelial cells were reported in young adult volunteers at bed rest who were given injectable calcitonin-salmon to study the effect of immobilization on osteoporosis. There was no other evidence of renal abnormality and the urine sediment normalized after calcitonin-salmon was stopped. Periodic examinations of urine sediment should be considered.
17 Patient Counseling Information
- Instruct patients and other persons who may administer Calcitonin Salmon injection in sterile injection technique. Also instruct patients to dispose of needles properly [see Dosage and Administration (2.4)].
- Inform patients of the potential increase in risk of malignancy [see Warnings and Precautions (5.3)].
- Advise patients with postmenopausal osteoporosis or Paget's disease of bone to maintain an adequate calcium (at least 1000 mg elemental calcium per day) and vitamin D (at least 400 International Units per day) intake [see Dosage and Administration (2.5)].
- Instruct patients to seek emergency medical help or go to the nearest hospital emergency room right away if they develop any signs or symptoms of a serious allergic reaction [see Warnings and Precautions (5.1)].
Lake Zurich, IL 60047
www.fresenius-kabi.com/us
451661
2.4 Preparation and Administration
Visually inspect Calcitonin Salmon vials. Calcitonin Salmon injection is a clear, colorless, solution. If the solution is not clear and colorless, or contains any particles, or if the vial is damaged, do not administer the solution.
If the volume of Calcitonin Salmon injection to be injected exceeds 2 mL, intramuscular injection is preferable and the total dose should be distributed across multiple sites of injection.
Instruct patients to use sterile injection technique when administering Calcitonin Salmon injection, and to dispose of needles properly.
1.1 Treatment of Paget's Disease of Bone
Calcitonin Salmon injection is indicated for the treatment of symptomatic Paget's disease of bone in patients with moderate to severe disease characterized by polyostotic involvement with elevated serum alkaline phosphatase and urinary hydroxyproline excretion. There is no evidence that the prophylactic use of calcitonin-salmon is beneficial in asymptomatic patients. Calcitonin Salmon injection should be used only in patients who do not respond to alternative treatments or for whom such treatments are not suitable (e.g., patients for whom other therapies are contraindicated or for patients who are intolerant or unwilling to use other therapies).
1.3 Treatment of Postmenopausal Osteoporosis
Calcitonin Salmon injection is indicated for the treatment of postmenopausal osteoporosis in women greater than 5 years postmenopause. The evidence of efficacy for calcitonin-salmon injection is based on increases in total body calcium observed in clinical trials. Fracture reduction efficacy has not been demonstrated. Calcitonin Salmon injection should be reserved for patients for whom alternative treatments are not suitable (e.g., patients for whom other therapies are contraindicated or for patients who are intolerant or unwilling to use other therapies).
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity
The incidence of pituitary adenomas was increased in rats after one and two years of subcutaneous exposure to synthetic calcitonin-salmon. The significance of this finding to humans is unknown because pituitary adenomas are very common in rats as they age, the pituitary adenomas did not transform into metastatic tumors, there were no other clear treatment-related neoplasms, and synthetic calcitonin-salmon related neoplasms were not observed in mice after two years of dosing.
2.5 Recommendations for Calcium and Vitamin D Supplementation
Patients who use Calcitonin Salmon injection for treatment of postmenopausal osteoporosis should receive adequate calcium (at least 1000 mg elemental calcium per day) and vitamin D (at least 400 International Units per day).
Structured Label Content
Section 42229-5 (42229-5)
Nausea: Nausea with or without vomiting has been noted in about 10% of patients treated with calcitonin-salmon. It is most evident when treatment is first initiated and tends to decrease or disappear with continued administration.
Section 44425-7 (44425-7)
Storage and Handling
Store in refrigerator between 2° to 8°C (36° to 46°F). Avoid freezing.
The container closure is not made with natural rubber latex.
Section 51945-4 (51945-4)
PACKAGE LABEL - PRINCIPAL DISPLAY – Calcitonin Salmon 2 mL Carton Panel
NDC 63323-865-02 865102
Calcitonin Salmon
Injection, USP Synthetic
400 I.U. per 2 mL
(200 I.U. per mL)
For Intramuscular or Subcutaneous Injection
Rx only 2 mL Multi-Dose Vial
10 Overdosage (10 OVERDOSAGE)
The pharmacologic actions of Calcitonin Salmon injection suggest that hypocalcemic tetany could occur in overdose. Therefore, provisions for parenteral administration of calcium should be available for the treatment of overdose.
A dose of calcitonin-salmon l000 International Units subcutaneously may produce nausea and vomiting. Doses of 32 International Units per kg per day for 1 to 2 days demonstrate no other adverse effects. Data on chronic high-dose administration are insufficient to assess toxicity.
11 Description (11 DESCRIPTION)
Calcitonin is a polypeptide hormone secreted by the parafollicular cells of the thyroid gland in mammals and by the ultimobranchial gland of birds and fish.
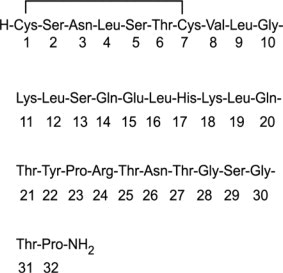
Calcitonin Salmon Injection, USP Synthetic is a synthetic polypeptide of 32 amino acids in the same linear sequence that is found in calcitonin of salmon origin. This is shown by the following graphic formula:
It is provided in sterile solution for subcutaneous or intramuscular injection. Each milliliter contains: calcitonin-salmon 200 International Units.
Inactive Ingredients (per mL): acetic acid, USP, 2.25 mg; phenol, USP, 5.0 mg; sodium acetate trihydrate, USP, 2.0 mg; sodium chloride, USP, 7.5 mg; water for injection, USP.
The activity of Calcitonin Salmon injection is stated in International Units based on bioassay in comparison with the International Reference Preparation of calcitonin-salmon for Bioassay, distributed by the National Institute for Biological Standards and Control, Holly Hill, London.
5.3 Malignancy
In a meta-analysis of 21 randomized, controlled clinical trials with calcitonin-salmon (nasal spray or investigational oral formulations), the overall incidence of malignancies reported was higher among calcitonin-salmon-treated patients (4.1%) compared with placebo-treated patients (2.9%). This suggests an increased risk of malignancies in calcitonin-salmon-treated patients compared to placebo-treated patients. It is not possible to exclude an increased risk when calcitonin-salmon is administered long-term subcutaneously, intramuscularly, or intravenously. The benefits for the individual patient should be carefully considered against possible risks [see Adverse Reactions (6.1)].
5.2 Hypocalcemia
Hypocalcemia associated with tetany (i.e., muscle cramps, twitching) and seizure activity has been reported with Calcitonin Salmon injection therapy. Hypocalcemia must be corrected before initiating therapy. Other disorders affecting mineral metabolism (such as vitamin D deficiency) should also be effectively treated. In patients at risk for hypocalcemia, provisions for parenteral calcium administration should be available during the first several administrations of calcitonin salmon and serum calcium and symptoms of hypocalcemia should be monitored. Use of Calcitonin Salmon injection for the treatment of Paget's disease or postmenopausal osteoporosis is recommended in conjunction with an adequate intake of calcium and vitamin D [see Dosage and Administration (2.5)].
2.2 Hypercalcemia
The recommended starting dose of Calcitonin Salmon injection for early treatment of hypercalcemia is 4 International Units/kg body weight every 12 hours by subcutaneous or intramuscular injection. If the response to this dose is not satisfactory after one or two days, the dose may be increased to 8 International Units/kg every 12 hours. If the response remains unsatisfactory after two more days, the dose may be further increased to a maximum of 8 International Units/kg every 6 hours.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
Clinical studies of Calcitonin Salmon injection did not include sufficient numbers of subjects aged 65 years and older to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
14.2 Hypercalcemia
In four open-label clinical trials enrolling 53 patients, calcitonin-salmon has been shown to lower elevated serum calcium levels of patients with carcinoma (with or without metastases), multiple myeloma, and primary hyperparathyroidism (lesser response). These patients were treated with calcitonin-salmon only when other methods of lowering serum calcium (hydration, oral phosphate, corticosteroids) were unsuccessful or unsuitable. With patients' pre-therapy serum calcium levels as controls, reduction in serum calcium was evident within 1 to 2 hours of administration. The peak effect occurred within 24 to 48 hours of injection and administration of calcitonin-salmon every 12 hours maintained a hypocalcemic effect for approximately 5 to 8 days, the time period evaluated for most patients in the clinical trials. The average reduction of 8 hour post-injection serum calcium was approximately 9% (2 to 3 mg/dL). Patients with higher values of serum calcium tended to show greater reductions during calcitonin-salmon treatment.
6.3 Immunogenicity
Consistent with the potentially immunogenic properties of medicinal products containing peptides, administration of Calcitonin Salmon may trigger the development of anti-calcitonin antibodies. Circulating antibodies to calcitonin-salmon after 2 to 18 months of treatment have been reported in about one-half of the patients with Paget's disease in whom antibody studies were done. In some cases, high antibody titers are found; these patients usually will have a loss of response to treatment [see Warnings and Precautions (5.4)].
The incidence of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of a positive antibody test result may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of antibodies among different calcitonin-salmon products may be misleading.
4 Contraindications (4 CONTRAINDICATIONS)
Hypersensitivity to calcitonin-salmon or any of the excipients. Reactions have included anaphylaxis with death, bronchospasm, and swelling of the tongue or throat [see Warnings and Precautions (5.1)].
6 Adverse Reactions (6 ADVERSE REACTIONS)
7 Drug Interactions (7 DRUG INTERACTIONS)
No formal drug interaction studies have been performed with Calcitonin Salmon injection.
Concomitant use of calcitonin-salmon and lithium may lead to a reduction in plasma lithium concentrations due to increased urinary clearance of lithium. The dose of lithium may require adjustment.
12.3 Pharmacokinetics
The absolute bioavailability of calcitonin-salmon is approximately 66% and 71% after intramuscular or subcutaneous injection, respectively. After subcutaneous administration, peak plasma levels are reached in approximately 23 minutes. The terminal half-life is approximately 58 minutes for intramuscular administration and 59 to 64 minutes for subcutaneous administration. The apparent volume of distribution is 0.15 to 0.3 L/kg.
5.4 Antibody Formation
Circulating antibodies to calcitonin-salmon have been reported with Calcitonin Salmon injection. The possibility of antibody formation should be considered in any patient with an initial response to Calcitonin Salmon injection who later stops responding to treatment [see Adverse Reactions (6.3)].
1 Indications and Usage (1 INDICATIONS AND USAGE)
Calcitonin Salmon synthetic injection is a calcitonin, indicated for the following conditions:
- Treatment of symptomatic Paget's disease of bone when alternative treatments are not suitable (1.1)
- Treatment of hypercalcemia (1.2)
- Treatment of postmenopausal osteoporosis when alternative treatments are not suitable. Fracture reduction efficacy has not been demonstrated (1.3)
Limitations of Use:
12.1 Mechanism of Action
Calcitonin-salmon is a calcitonin receptor agonist. Calcitonin-salmon acts primarily on bone, but direct renal effects and actions on the gastrointestinal tract are also recognized. Calcitonin salmon appears to have actions essentially identical to calcitonins of mammalian origin, but its potency per mg is greater and it has a longer duration of action.
The actions of calcitonin on bone and its role in normal human bone physiology are still not completely elucidated, although calcitonin receptors have been discovered in osteoclasts and osteoblasts.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
- Serious hypersensitivity reactions, including reports of fatal anaphylaxis have been reported. Consider skin testing prior to treatment in patients with suspected hypersensitivity to calcitonin-salmon (5.1)
- Hypocalcemia has been reported. Ensure adequate intake of calcium and vitamin D (5.2)
- Malignancy: A meta-analysis of 21 clinical trials suggests an increased risk of overall malignancies in calcitonin-salmon- treated patients (5.3, 6.1)
- Circulating antibodies to calcitonin-salmon may develop, and may cause loss of response to treatment (5.4)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
- Symptomatic Paget's disease of bone: 100 International Units daily. Ensure adequate calcium and vitamin D intake (2.1, 2.5)
- Hypercalcemia: start with 4 International Units/kg body weight every 12 hours. Increase to 8 International Units/kg every 12 hours if no improvement in 1-2 days. Increase further to 8 International Units/kg every 6 hours if no improvement after 2 more days (2.2)
- Postmenopausal osteoporosis: 100 International Units daily. Ensure adequate calcium and vitamin D intake (2.3, 2.5)
2.1 Paget's Disease of Bone
The recommended dose of Calcitonin Salmon injection for treatment of symptomatic Paget's disease of bone is 100 International Units (0.5 mL) per day administered subcutaneously or intramuscularly.
14.1 Paget's Disease of Bone
The trials used for the basis of approval for calcitonin-salmon injection for treatment of Paget's disease of bone were conducted in patients with moderate to severe disease characterized by polyostotic involvement with elevated serum alkaline phosphatase and urinary hydroxyproline excretion. In open-label clinical trials of several months to two years duration with historical controls, biochemical abnormalities were substantially improved (more than 30% reduction) in about 2/3 of patients studied and bone pain was improved in a similar fraction. A small number of documented instances of reversal of neurologic deficits have occurred, including improvement in the basilar compression syndrome, and improvement of spinal cord and spinal nerve lesions.
There is too little experience to predict the likelihood of improvement of any given neurologic lesion. Hearing loss is improved infrequently (4 of 29 patients studied by audiometry). Patients with increased cardiac output due to extensive Paget's disease of bone have had measured decreases in cardiac output while receiving calcitonin-salmon. The number of treated patients in this category is too small to predict how likely such a result will be.
There is no evidence that the prophylactic use of calcitonin-salmon is beneficial in asymptomatic patients.
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Calcitonin Salmon Injection, USP is available as a clear, colorless, sterile solution of synthetic calcitonin salmon in individual 2 mL multi-dose vials containing 200 International Units per mL.
6.2 Postmarketing Experience
Because postmarketing adverse reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The following adverse reactions have been reported during post-approval use of Calcitonin Salmon injection.
Allergic / Hypersensitivity Reactions: Serious hypersensitivity reactions have been reported in patients receiving calcitonin-salmon injection, e.g., bronchospasm, swelling of the tongue or throat, anaphylactic shock, and death due to anaphylaxis.
Skin and subcutaneous tissue disorders: Urticaria
Hypocalcemia: Hypocalcemia with tetany (i.e. muscle cramps, twitching) and seizure activity have been reported.
Body as a Whole: influenza-like symptoms, fatigue, edema (facial, peripheral, and generalized)
Musculoskeletal: arthralgia, musculoskeletal pain
Cardiovascular: hypertension
Gastrointestinal: abdominal pain, diarrhea
Urinary System: polyuria
Nervous System: dizziness, headache, paresthesia, tremor
Vision: visual disturbance
8 Use in Specific Populations (8 USE IN SPECIFIC POPULATIONS)
There are no data to support use in children (8.4)
1.2 Treatment of Hypercalcemia
Calcitonin Salmon injection is indicated for the early treatment of hypercalcemic emergencies, along with other appropriate agents, when a rapid decrease in serum calcium is required, until more specific treatment of the underlying disease can be accomplished. It may also be added to existing therapeutic regimens for hypercalcemia such as intravenous fluids and furosemide, oral phosphate or corticosteroids, or other agents.
5.1 Hypersensitivity Reactions
Serious hypersensitivity reactions have been reported in patients receiving Calcitonin Salmon injection, e.g., bronchospasm, swelling of the tongue or throat, anaphylactic shock, and death due to anaphylaxis. Appropriate medical support and monitoring measures should be readily available when Calcitonin Salmon injection is administered. If anaphylaxis or other severe hypersensitivity/allergic reactions occur, initiate appropriate treatment [see Contraindications (4)].
For patients with suspected hypersensitivity to calcitonin-salmon, skin testing should be considered prior to treatment utilizing a dilute, sterile solution of Calcitonin Salmon injection. Healthcare providers may wish to refer patients who require skin testing to an allergist.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of calcitonin-salmon injection was assessed in open-label trials several months to two years in duration. The most common adverse reactions are discussed below.
2.3 Postmenopausal Osteoporosis
The recommended dose of Calcitonin Salmon injection for treatment of postmenopausal osteoporosis in women greater than 5 years postmenopause is 100 International Units (0.5 mL) per day administered subcutaneously or intramuscularly. The minimum effective dose of Calcitonin Salmon injection for the prevention of vertebral bone mineral density loss has not been established.
1.4 Important Limitations of Use
Due to the possible association between malignancy and calcitonin-salmon use, the need for continued therapy should be re-evaluated on a periodic basis [see Warnings and Precautions (5.3)].
14.3 Postmenopausal Osteoporosis
The trials used for the basis of approval for calcitonin-salmon injection for treatment of postmenopausal osteoporosis were two randomized, open-label, 2-year studies in postmenopausal women 50 to 74 years of age with total body calcium < 85% of expected normal, and vertebral osteopenia (by x-ray criteria) and/or at least one atraumatic compression fracture. The primary efficacy endpoint was total body calcium measured by neutron activation analysis. Patients were randomized to calcitonin-salmon injection 100 International Units daily (subcutaneously or intramuscularly) at bedtime, or control. All subjects received daily supplements of 1200 mg calcium carbonate and 400 International Units of vitamin D.
In both studies, total body calcium increased from baseline with calcitonin-salmon therapy at 1 year, followed by a trend to decreasing total body calcium (still above baseline) at 2 years.
Thoracic and lumbar spine X-rays (AP/lateral) were obtained yearly. For the two studies combined (34 calcitonin-salmon and 35 control subjects), in the first year there was a total of 6 new vertebral compression fractures in the calcitonin-salmon group and 5 in the control group. In the second year there were 7 new fractures in each group.
No evidence currently exists to indicate whether Calcitonin Salmon injection decreases the risk of osteoporotic fracture. A controlled study, which was prematurely discontinued, failed to demonstrate any benefit of calcitonin-salmon on fracture rate.
No adequate controlled trials have examined the effect of calcitonin-salmon injection on vertebral bone mineral density beyond 1 year of treatment. Therefore, the minimum effective dose of Calcitonin Salmon injection for prevention of vertebral bone mineral density loss has not been established.
In clinical studies of postmenopausal osteoporosis, bone biopsy and radial bone mass assessments at baseline and after 26 months of daily injectable calcitonin-salmon indicate that calcitonin therapy results in the formation of normal bone.
5.5 Urine Sediment Abnormalities
Coarse granular casts and casts containing renal tubular epithelial cells were reported in young adult volunteers at bed rest who were given injectable calcitonin-salmon to study the effect of immobilization on osteoporosis. There was no other evidence of renal abnormality and the urine sediment normalized after calcitonin-salmon was stopped. Periodic examinations of urine sediment should be considered.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
- Instruct patients and other persons who may administer Calcitonin Salmon injection in sterile injection technique. Also instruct patients to dispose of needles properly [see Dosage and Administration (2.4)].
- Inform patients of the potential increase in risk of malignancy [see Warnings and Precautions (5.3)].
- Advise patients with postmenopausal osteoporosis or Paget's disease of bone to maintain an adequate calcium (at least 1000 mg elemental calcium per day) and vitamin D (at least 400 International Units per day) intake [see Dosage and Administration (2.5)].
- Instruct patients to seek emergency medical help or go to the nearest hospital emergency room right away if they develop any signs or symptoms of a serious allergic reaction [see Warnings and Precautions (5.1)].
Lake Zurich, IL 60047
www.fresenius-kabi.com/us
451661
2.4 Preparation and Administration
Visually inspect Calcitonin Salmon vials. Calcitonin Salmon injection is a clear, colorless, solution. If the solution is not clear and colorless, or contains any particles, or if the vial is damaged, do not administer the solution.
If the volume of Calcitonin Salmon injection to be injected exceeds 2 mL, intramuscular injection is preferable and the total dose should be distributed across multiple sites of injection.
Instruct patients to use sterile injection technique when administering Calcitonin Salmon injection, and to dispose of needles properly.
1.1 Treatment of Paget's Disease of Bone
Calcitonin Salmon injection is indicated for the treatment of symptomatic Paget's disease of bone in patients with moderate to severe disease characterized by polyostotic involvement with elevated serum alkaline phosphatase and urinary hydroxyproline excretion. There is no evidence that the prophylactic use of calcitonin-salmon is beneficial in asymptomatic patients. Calcitonin Salmon injection should be used only in patients who do not respond to alternative treatments or for whom such treatments are not suitable (e.g., patients for whom other therapies are contraindicated or for patients who are intolerant or unwilling to use other therapies).
1.3 Treatment of Postmenopausal Osteoporosis
Calcitonin Salmon injection is indicated for the treatment of postmenopausal osteoporosis in women greater than 5 years postmenopause. The evidence of efficacy for calcitonin-salmon injection is based on increases in total body calcium observed in clinical trials. Fracture reduction efficacy has not been demonstrated. Calcitonin Salmon injection should be reserved for patients for whom alternative treatments are not suitable (e.g., patients for whom other therapies are contraindicated or for patients who are intolerant or unwilling to use other therapies).
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity
The incidence of pituitary adenomas was increased in rats after one and two years of subcutaneous exposure to synthetic calcitonin-salmon. The significance of this finding to humans is unknown because pituitary adenomas are very common in rats as they age, the pituitary adenomas did not transform into metastatic tumors, there were no other clear treatment-related neoplasms, and synthetic calcitonin-salmon related neoplasms were not observed in mice after two years of dosing.
2.5 Recommendations for Calcium and Vitamin D Supplementation
Patients who use Calcitonin Salmon injection for treatment of postmenopausal osteoporosis should receive adequate calcium (at least 1000 mg elemental calcium per day) and vitamin D (at least 400 International Units per day).
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:44:14.991545 · Updated: 2026-03-14T22:19:26.002754