Isopto® Atropine
20491566-e6eb-8d4a-3083-77ea429f7bc4
34391-3
HUMAN PRESCRIPTION DRUG LABEL
Drug Facts
Composition & Product
Identifiers & Packaging
Indications and Usage
ISOPTO ® Atropine 1% is indicated for:
Dosage and Administration
2.1 In individuals from three (3) months of age or greater, 1 drop topically to the cul-de-sac of the conjunctiva, forty minutes prior to the intended maximal dilation time. 2.2 In individuals 3 years of age or greater, doses may be repeated up to twice daily as needed.
Contraindications
Atropine sulfate ophthalmic solution should not be used in anyone who has demonstrated a previous hypersensitivity or known allergic reaction to any ingredient of the formulation because it may recur.
Warnings and Precautions
Photophobia and blurred vision due to pupil unresponsiveness and cycloplegia may last up to 2 weeks. ( 5.1 ) Risk of blood pressure increase from systemic absorption ( 5.2 ) Increased adverse drug reaction susceptibility with certain central nervous system conditions ( 5.3 )
Adverse Reactions
Eye pain and stinging occurs upon instillation of atropine sulfate ophthalmic solution. Other commonly occurring adverse reactions include blurred vision, photophobia, superficial keratitis and decreased lacrimation. Allergic reactions such as papillary conjunctivitis, contact dermatitis, and eyelid edema may also occur less commonly.
Drug Interactions
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis. ( 7 )
How Supplied
ISOPTO® Atropine 1% is supplied sterile in low-density polyethylene plastic DROP-TAINER® dispensers with low-density polyethylene tips and red polypropylene caps as follows: 5 mL filled in 8-mL bottles NDC 0065-0303-55 Storage: Store ISOPTO® Atropine 1% at 2–25°C (36–77°F).
Storage and Handling
ISOPTO® Atropine 1% is supplied sterile in low-density polyethylene plastic DROP-TAINER® dispensers with low-density polyethylene tips and red polypropylene caps as follows: 5 mL filled in 8-mL bottles NDC 0065-0303-55 Storage: Store ISOPTO® Atropine 1% at 2–25°C (36–77°F).
Description
ISOPTO ® Atropine 1% is indicated for:
Medication Information
Warnings and Precautions
Photophobia and blurred vision due to pupil unresponsiveness and cycloplegia may last up to 2 weeks. ( 5.1 ) Risk of blood pressure increase from systemic absorption ( 5.2 ) Increased adverse drug reaction susceptibility with certain central nervous system conditions ( 5.3 )
Indications and Usage
ISOPTO ® Atropine 1% is indicated for:
Dosage and Administration
2.1 In individuals from three (3) months of age or greater, 1 drop topically to the cul-de-sac of the conjunctiva, forty minutes prior to the intended maximal dilation time. 2.2 In individuals 3 years of age or greater, doses may be repeated up to twice daily as needed.
Contraindications
Atropine sulfate ophthalmic solution should not be used in anyone who has demonstrated a previous hypersensitivity or known allergic reaction to any ingredient of the formulation because it may recur.
Adverse Reactions
Eye pain and stinging occurs upon instillation of atropine sulfate ophthalmic solution. Other commonly occurring adverse reactions include blurred vision, photophobia, superficial keratitis and decreased lacrimation. Allergic reactions such as papillary conjunctivitis, contact dermatitis, and eyelid edema may also occur less commonly.
Drug Interactions
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis. ( 7 )
Storage and Handling
ISOPTO® Atropine 1% is supplied sterile in low-density polyethylene plastic DROP-TAINER® dispensers with low-density polyethylene tips and red polypropylene caps as follows: 5 mL filled in 8-mL bottles NDC 0065-0303-55 Storage: Store ISOPTO® Atropine 1% at 2–25°C (36–77°F).
How Supplied
ISOPTO® Atropine 1% is supplied sterile in low-density polyethylene plastic DROP-TAINER® dispensers with low-density polyethylene tips and red polypropylene caps as follows: 5 mL filled in 8-mL bottles NDC 0065-0303-55 Storage: Store ISOPTO® Atropine 1% at 2–25°C (36–77°F).
Description
ISOPTO ® Atropine 1% is indicated for:
1.1 Mydriasis
10 Overdosage
In the event of accidental ingestion or toxic overdosage with atropine sulfate ophthalmic solution supportive care may include a short acting barbiturate or diazepam as needed to control marked excitement and convulsions. Large doses for sedation should be avoided because central depressant action may coincide with the depression occurring late in atropine poisoning. Central stimulants are not recommended.
Physostigmine, given by slow intravenous injection of 1 to 4 mg (0.5 to 1 mg in pediatric populations), rapidly abolishes delirium and coma caused by large doses of atropine. Since physostigmine is rapidly destroyed, the patient may again lapse into coma after one to two hours, and repeated doses may be required.
Artificial respiration with oxygen may be necessary. Cooling measures may be needed to help to reduce fever, especially in pediatric populations.
The fatal pediatric and adult doses of atropine are not known.
8.1 Pregnancy
Risk Summary
There are no adequate and well-controlled studies with ISOPTO® Atropine 1% administration in pregnant women to inform a drug-associated risk. Adequate animal development and reproduction studies have not been conducted with atropine sulfate. In humans, 1% atropine sulfate is systemically bioavailable following topical ocular administration [see Clinical Pharmacology (12.3)]. ISOPTO® Atropine 1% should only be used during pregnancy if the potential benefit justifies the potential risk to the fetus.
8.2 Lactation
There is no information to inform risk regarding the presence of atropine in human milk following ocular administration of ISOPTO® Atropine 1% to the mother. The effects on breastfed infants and the effects on milk production are also unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ISOPTO® Atropine 1% and any potential adverse effects on the breastfed child from ISOPTO® Atropine 1%.
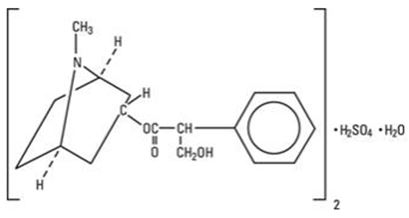
11 Description
ISOPTO® Atropine 1% is a sterile topical ophthalmic solution. Each mL of ISOPTO® Atropine 1% contains 10 mg of atropine sulfate monohydrate equivalent to 9.7 mg/mL of atropine sulfate or 8.3 mg of atropine. Atropine sulfate monohydrate is designated chemically as benzeneacetic acid, α-(hydroxymethyl)-,8-methyl-8-aza-bicyclo-[3.2.1]oct-3-yl ester, endo-(+)-, sulfate(2:1) (salt), monohydrate. Its molecular formula is (C17H23NO3)2 • H2SO4 • H2O and it is represented by the chemical structure:
Atropine sulfate monohydrate is colorless crystals or white crystalline powder and has a molecular weight of 694.83.
ISOPTO® Atropine 1% has a pH of 3.5 to 6.0.
Active ingredient: atropine sulfate monohydrate 1.0%
Preservative: benzalkonium chloride 0.01%
Inactive ingredients: hypromellose, boric acid, sodium hydroxide and/or hydrochloric acid (to adjust pH), purified water.
1.2 Cycloplegia
8.4 Pediatric Use
Due to the potential for systemic absorption of atropine sulfate ophthalmic solution the use of ISOPTO® Atropine 1% in children under the age of 3 months is not recommended and the use in children under 3 years of age should be limited to no more than one drop per eye per day. Safety and efficacy in children above the age of 3 months has been established in adequate and well controlled trials.
8.5 Geriatric Use
No overall differences in safety or effectiveness have been observed between elderly and adult patients.
14 Clinical Studies
Topical administration of ISOPTO® Atropine 1% results in mydriasis and/or cycloplegia, with efficacy demonstrated in both adults and children. The maximum effect for mydriasis is achieved in about 30–40 minutes after administration, with recovery after approximately 7–10 days. The maximum effect for cycloplegia is achieved within 60–180 minutes after administration, with recovery after approximately 7–12 days.
4 Contraindications
Atropine sulfate ophthalmic solution should not be used in anyone who has demonstrated a previous hypersensitivity or known allergic reaction to any ingredient of the formulation because it may recur.
6 Adverse Reactions
The following adverse reactions are described below and elsewhere in the labeling:
- Photophobia and Blurred Vision [see Warnings and Precautions (5.1)]
- Elevation in Blood Pressure [see Warnings and Precautions (5.2)]
- Increased Adverse Drug Reaction Susceptibility with Certain Central Nervous System Conditions [see Warnings and Precautions (5.3)]
The following adverse reactions have been identified following use of atropine sulfate ophthalmic solution. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
7 Drug Interactions
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis. (7)
12.2 Pharmacodynamics
The onset of action after administration of ISOPTO Atropine 1% generally occurs in minutes with maximal effect seen in hours and the effect can last multiple days [see Clinical Studies (14)].
12.3 Pharmacokinetics
In a study of healthy subjects, after topical ocular administration of 30 µL of atropine sulfate ophthalmic solution, 1%, the mean (± SD) systemic bioavailability of l-hyoscyamine was reported to be approximately 64 ± 29% (range 19% to 95%) as compared to intravenous administration of atropine sulfate. The mean (± SD) time to maximum plasma concentration (Tmax) was approximately 28 ± 27 minutes (range 3 to 60 minutes), and the mean (±SD) peak plasma concentration (Cmax) of l-hyoscyamine was 288 ± 73 pg/mL. The mean (±SD) plasma half-life was reported to be approximately 2.5 ± 0.8 hours.
In a separate study of patients undergoing ocular surgery, after topical ocular administration of 40 µL of atropine sulfate ophthalmic solution, 1%, the mean (± SD) plasma Cmax of l‑hyoscyamine was 860 ± 402 pg/mL.
1 Indications and Usage
ISOPTO® Atropine 1% is indicated for:
12.1 Mechanism of Action
Atropine acts as a competitive antagonist of the parasympathetic (and sympathetic) acetylcholine muscarinic receptors. Topical atropine on the eye induces mydriasis by inhibiting contraction of the circular pupillary sphincter muscle normally stimulated by acetylcholine. This inhibition allows the countering radial pupillary dilator muscle to contract which results in dilation of the pupil. Additionally, atropine induces cycloplegia by paralysis of the ciliary muscle which controls accommodation while viewing objects.
5 Warnings and Precautions
2 Dosage and Administration
2.1 In individuals from three (3) months of age or greater, 1 drop topically to the cul-de-sac of the conjunctiva, forty minutes prior to the intended maximal dilation time.
2.2 In individuals 3 years of age or greater, doses may be repeated up to twice daily as needed.
3 Dosage Forms and Strengths
Ophthalmic solution: 1% atropine sulfate (10mg/mL)
6.1 Ocular Adverse Reactions
Eye pain and stinging occurs upon instillation of atropine sulfate ophthalmic solution. Other commonly occurring adverse reactions include blurred vision, photophobia, superficial keratitis and decreased lacrimation. Allergic reactions such as papillary conjunctivitis, contact dermatitis, and eyelid edema may also occur less commonly.
6.2 Systemic Adverse Reactions
Systemic effects of atropine are related to its anti-muscarinic activity. Systemic adverse events reported include dryness of skin, mouth, and throat from decreased secretions from mucus membranes; drowsiness; restlessness, irritability or delirium from stimulation of the central nervous system; tachycardia; flushed skin of the face and neck.
5.2 Elevation of Blood Pressure
Elevation in blood pressure from systemic absorption has been reported following conjunctival instillation of recommended doses of atropine sulfate ophthalmic solution, 1%.
7.1 Monoamine Oxidase Inhibitors
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis.
17 Patient Counseling Information
- Advise patients not to drive or engage in other hazardous activities while pupils are dilated.
- Advise patient that they may experience blurry vision and sensitivity to light and should protect their eyes in bright illumination during dilation. These effects may last up to a couple weeks.
- Advise patients that they may experience drowsiness.
- Advise patients not to touch the dispenser tip to any surface, as this may contaminate the solution.
ALCON®
A Novartis company
Fort Worth, Texas 76134 USA
© 2016, 2018 Novartis
5.1 Photophobia and Blurred Vision
Photophobia and blurred vision due to pupil unresponsiveness and cycloplegia may last up to 2 weeks.
16 How Supplied/storage and Handling
ISOPTO® Atropine 1% is supplied sterile in low-density polyethylene plastic DROP-TAINER® dispensers with low-density polyethylene tips and red polypropylene caps as follows:
- 5 mL filled in 8-mL bottles NDC 0065-0303-55
Storage: Store ISOPTO® Atropine 1% at 2–25°C (36–77°F).
Package Label.principal Display Panel
NDC 0065-0303-55
Alcon®
Isopto® Atropine
(atropine sulfate ophthalmic solution) 1%
5 mL Sterile
USUAL ADULT DOSAGE: One drop topically in the eye(s) up to twice daily. For other dosage information, read enclosed insert.
PRECAUTION: Do not touch dropper tip to any surface, as this may contaminate the solution.
STORAGE: Store at 2°-25°C (36°-77°F). Read enclosed insert.
Rx Only
INGREDIENTS: Each mL
contains: Active: atropine sulfate monohydrate 1.0%.
Preservative: benzalkonium chloride 0.01%.
Inactives: hypromellose 0.5%, boric acid, sodium hydroxide and/or hydrochloric acid (to adjust pH), purified water.
© 2003, 2018 Novartis
Alcon®
ALCON LABORATORIES, INC.
Fort Worth, Texas 76134 USA
Product of Germany
9016388-0618
SN:
LOT:
EXP.:
GTIN: 00300650303552
NDC 0065-0303-55
Alcon®
Isopto® Atropine
(atropine sulfate ophthalmic solution) 1%
Sterile 5mL
Rx Only
INGREDIENTS: Each mL contains:
Active: atropine sulfate monohydrate 1.0%.
Preservative: benzalkonium chloride 0.01%.
Inactives: hypromellose 0.5%, boric acid, sodium hydroxide and/or hydrochloric acid (to adjust pH), purified water.
PRECAUTION: Do not touch dropper tip to any surface, as this may contaminate the solution.
USUAL ADULT DOSAGE: One drop topically in the eye(s) up to twice daily. For other dosage information, read enclosed insert. FOR TOPICAL OPHTHALMIC USE.
STORAGE: Store at 2°-25°C (36°-77°F).
ALCON LABORATORIES, INC.
Fort Worth, Texas 76134 USA
©2018 Novartis
H15250-0318
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Atropine sulfate was negative in the Salmonella/microsome mutagenicity test. Studies to evaluate carcinogenicity and impairment of fertility have not been conducted.
1.3 Penalization of the Healthy Eye in the Treatment of Amblyopia
5.3 Increased Adverse Drug Reaction Susceptibility With Certain Central Nervous System Conditions
Individuals with Down syndrome, spastic paralysis, or brain damage are particularly susceptible to central nervous system disturbances, cardiopulmonary, and gastrointestinal toxicity from systemic absorption of atropine.
Structured Label Content
1.1 Mydriasis
10 Overdosage (10 OVERDOSAGE)
In the event of accidental ingestion or toxic overdosage with atropine sulfate ophthalmic solution supportive care may include a short acting barbiturate or diazepam as needed to control marked excitement and convulsions. Large doses for sedation should be avoided because central depressant action may coincide with the depression occurring late in atropine poisoning. Central stimulants are not recommended.
Physostigmine, given by slow intravenous injection of 1 to 4 mg (0.5 to 1 mg in pediatric populations), rapidly abolishes delirium and coma caused by large doses of atropine. Since physostigmine is rapidly destroyed, the patient may again lapse into coma after one to two hours, and repeated doses may be required.
Artificial respiration with oxygen may be necessary. Cooling measures may be needed to help to reduce fever, especially in pediatric populations.
The fatal pediatric and adult doses of atropine are not known.
8.1 Pregnancy
Risk Summary
There are no adequate and well-controlled studies with ISOPTO® Atropine 1% administration in pregnant women to inform a drug-associated risk. Adequate animal development and reproduction studies have not been conducted with atropine sulfate. In humans, 1% atropine sulfate is systemically bioavailable following topical ocular administration [see Clinical Pharmacology (12.3)]. ISOPTO® Atropine 1% should only be used during pregnancy if the potential benefit justifies the potential risk to the fetus.
8.2 Lactation
There is no information to inform risk regarding the presence of atropine in human milk following ocular administration of ISOPTO® Atropine 1% to the mother. The effects on breastfed infants and the effects on milk production are also unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ISOPTO® Atropine 1% and any potential adverse effects on the breastfed child from ISOPTO® Atropine 1%.
11 Description (11 DESCRIPTION)
ISOPTO® Atropine 1% is a sterile topical ophthalmic solution. Each mL of ISOPTO® Atropine 1% contains 10 mg of atropine sulfate monohydrate equivalent to 9.7 mg/mL of atropine sulfate or 8.3 mg of atropine. Atropine sulfate monohydrate is designated chemically as benzeneacetic acid, α-(hydroxymethyl)-,8-methyl-8-aza-bicyclo-[3.2.1]oct-3-yl ester, endo-(+)-, sulfate(2:1) (salt), monohydrate. Its molecular formula is (C17H23NO3)2 • H2SO4 • H2O and it is represented by the chemical structure:
Atropine sulfate monohydrate is colorless crystals or white crystalline powder and has a molecular weight of 694.83.
ISOPTO® Atropine 1% has a pH of 3.5 to 6.0.
Active ingredient: atropine sulfate monohydrate 1.0%
Preservative: benzalkonium chloride 0.01%
Inactive ingredients: hypromellose, boric acid, sodium hydroxide and/or hydrochloric acid (to adjust pH), purified water.
1.2 Cycloplegia
8.4 Pediatric Use
Due to the potential for systemic absorption of atropine sulfate ophthalmic solution the use of ISOPTO® Atropine 1% in children under the age of 3 months is not recommended and the use in children under 3 years of age should be limited to no more than one drop per eye per day. Safety and efficacy in children above the age of 3 months has been established in adequate and well controlled trials.
8.5 Geriatric Use
No overall differences in safety or effectiveness have been observed between elderly and adult patients.
14 Clinical Studies (14 CLINICAL STUDIES)
Topical administration of ISOPTO® Atropine 1% results in mydriasis and/or cycloplegia, with efficacy demonstrated in both adults and children. The maximum effect for mydriasis is achieved in about 30–40 minutes after administration, with recovery after approximately 7–10 days. The maximum effect for cycloplegia is achieved within 60–180 minutes after administration, with recovery after approximately 7–12 days.
4 Contraindications (4 CONTRAINDICATIONS)
Atropine sulfate ophthalmic solution should not be used in anyone who has demonstrated a previous hypersensitivity or known allergic reaction to any ingredient of the formulation because it may recur.
6 Adverse Reactions (6 ADVERSE REACTIONS)
The following adverse reactions are described below and elsewhere in the labeling:
- Photophobia and Blurred Vision [see Warnings and Precautions (5.1)]
- Elevation in Blood Pressure [see Warnings and Precautions (5.2)]
- Increased Adverse Drug Reaction Susceptibility with Certain Central Nervous System Conditions [see Warnings and Precautions (5.3)]
The following adverse reactions have been identified following use of atropine sulfate ophthalmic solution. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
7 Drug Interactions (7 DRUG INTERACTIONS)
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis. (7)
12.2 Pharmacodynamics
The onset of action after administration of ISOPTO Atropine 1% generally occurs in minutes with maximal effect seen in hours and the effect can last multiple days [see Clinical Studies (14)].
12.3 Pharmacokinetics
In a study of healthy subjects, after topical ocular administration of 30 µL of atropine sulfate ophthalmic solution, 1%, the mean (± SD) systemic bioavailability of l-hyoscyamine was reported to be approximately 64 ± 29% (range 19% to 95%) as compared to intravenous administration of atropine sulfate. The mean (± SD) time to maximum plasma concentration (Tmax) was approximately 28 ± 27 minutes (range 3 to 60 minutes), and the mean (±SD) peak plasma concentration (Cmax) of l-hyoscyamine was 288 ± 73 pg/mL. The mean (±SD) plasma half-life was reported to be approximately 2.5 ± 0.8 hours.
In a separate study of patients undergoing ocular surgery, after topical ocular administration of 40 µL of atropine sulfate ophthalmic solution, 1%, the mean (± SD) plasma Cmax of l‑hyoscyamine was 860 ± 402 pg/mL.
1 Indications and Usage (1 INDICATIONS AND USAGE)
ISOPTO® Atropine 1% is indicated for:
12.1 Mechanism of Action
Atropine acts as a competitive antagonist of the parasympathetic (and sympathetic) acetylcholine muscarinic receptors. Topical atropine on the eye induces mydriasis by inhibiting contraction of the circular pupillary sphincter muscle normally stimulated by acetylcholine. This inhibition allows the countering radial pupillary dilator muscle to contract which results in dilation of the pupil. Additionally, atropine induces cycloplegia by paralysis of the ciliary muscle which controls accommodation while viewing objects.
5 Warnings and Precautions (5 WARNINGS AND PRECAUTIONS)
2 Dosage and Administration (2 DOSAGE AND ADMINISTRATION)
2.1 In individuals from three (3) months of age or greater, 1 drop topically to the cul-de-sac of the conjunctiva, forty minutes prior to the intended maximal dilation time.
2.2 In individuals 3 years of age or greater, doses may be repeated up to twice daily as needed.
3 Dosage Forms and Strengths (3 DOSAGE FORMS AND STRENGTHS)
Ophthalmic solution: 1% atropine sulfate (10mg/mL)
6.1 Ocular Adverse Reactions
Eye pain and stinging occurs upon instillation of atropine sulfate ophthalmic solution. Other commonly occurring adverse reactions include blurred vision, photophobia, superficial keratitis and decreased lacrimation. Allergic reactions such as papillary conjunctivitis, contact dermatitis, and eyelid edema may also occur less commonly.
6.2 Systemic Adverse Reactions
Systemic effects of atropine are related to its anti-muscarinic activity. Systemic adverse events reported include dryness of skin, mouth, and throat from decreased secretions from mucus membranes; drowsiness; restlessness, irritability or delirium from stimulation of the central nervous system; tachycardia; flushed skin of the face and neck.
5.2 Elevation of Blood Pressure
Elevation in blood pressure from systemic absorption has been reported following conjunctival instillation of recommended doses of atropine sulfate ophthalmic solution, 1%.
7.1 Monoamine Oxidase Inhibitors
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis.
17 Patient Counseling Information (17 PATIENT COUNSELING INFORMATION)
- Advise patients not to drive or engage in other hazardous activities while pupils are dilated.
- Advise patient that they may experience blurry vision and sensitivity to light and should protect their eyes in bright illumination during dilation. These effects may last up to a couple weeks.
- Advise patients that they may experience drowsiness.
- Advise patients not to touch the dispenser tip to any surface, as this may contaminate the solution.
ALCON®
A Novartis company
Fort Worth, Texas 76134 USA
© 2016, 2018 Novartis
5.1 Photophobia and Blurred Vision
Photophobia and blurred vision due to pupil unresponsiveness and cycloplegia may last up to 2 weeks.
16 How Supplied/storage and Handling (16 HOW SUPPLIED/STORAGE AND HANDLING)
ISOPTO® Atropine 1% is supplied sterile in low-density polyethylene plastic DROP-TAINER® dispensers with low-density polyethylene tips and red polypropylene caps as follows:
- 5 mL filled in 8-mL bottles NDC 0065-0303-55
Storage: Store ISOPTO® Atropine 1% at 2–25°C (36–77°F).
Package Label.principal Display Panel (PACKAGE LABEL.PRINCIPAL DISPLAY PANEL)
NDC 0065-0303-55
Alcon®
Isopto® Atropine
(atropine sulfate ophthalmic solution) 1%
5 mL Sterile
USUAL ADULT DOSAGE: One drop topically in the eye(s) up to twice daily. For other dosage information, read enclosed insert.
PRECAUTION: Do not touch dropper tip to any surface, as this may contaminate the solution.
STORAGE: Store at 2°-25°C (36°-77°F). Read enclosed insert.
Rx Only
INGREDIENTS: Each mL
contains: Active: atropine sulfate monohydrate 1.0%.
Preservative: benzalkonium chloride 0.01%.
Inactives: hypromellose 0.5%, boric acid, sodium hydroxide and/or hydrochloric acid (to adjust pH), purified water.
© 2003, 2018 Novartis
Alcon®
ALCON LABORATORIES, INC.
Fort Worth, Texas 76134 USA
Product of Germany
9016388-0618
SN:
LOT:
EXP.:
GTIN: 00300650303552
NDC 0065-0303-55
Alcon®
Isopto® Atropine
(atropine sulfate ophthalmic solution) 1%
Sterile 5mL
Rx Only
INGREDIENTS: Each mL contains:
Active: atropine sulfate monohydrate 1.0%.
Preservative: benzalkonium chloride 0.01%.
Inactives: hypromellose 0.5%, boric acid, sodium hydroxide and/or hydrochloric acid (to adjust pH), purified water.
PRECAUTION: Do not touch dropper tip to any surface, as this may contaminate the solution.
USUAL ADULT DOSAGE: One drop topically in the eye(s) up to twice daily. For other dosage information, read enclosed insert. FOR TOPICAL OPHTHALMIC USE.
STORAGE: Store at 2°-25°C (36°-77°F).
ALCON LABORATORIES, INC.
Fort Worth, Texas 76134 USA
©2018 Novartis
H15250-0318
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Atropine sulfate was negative in the Salmonella/microsome mutagenicity test. Studies to evaluate carcinogenicity and impairment of fertility have not been conducted.
1.3 Penalization of the Healthy Eye in the Treatment of Amblyopia (1.3 Penalization of the healthy eye in the treatment of amblyopia)
5.3 Increased Adverse Drug Reaction Susceptibility With Certain Central Nervous System Conditions (5.3 Increased Adverse Drug Reaction Susceptibility with Certain Central Nervous System Conditions)
Individuals with Down syndrome, spastic paralysis, or brain damage are particularly susceptible to central nervous system disturbances, cardiopulmonary, and gastrointestinal toxicity from systemic absorption of atropine.
Advanced Ingredient Data
Raw Label Data
All Sections (JSON)
Additional Information
Back to search View SPL set listing Open on DailyMed ↗
Source: dailymed · Ingested: 2026-02-15T11:37:19.295134 · Updated: 2026-03-14T21:49:42.549823